Even when taking medication, some patients with bipolar disorder experience breakthrough symptoms and relapse. Though studies suggest that a combination of medication and psychotherapy may reduce relapse risk in patients with bipolar disorder, psychotherapy is often out of reach for many patients. A
report in
JAMA Psychiatry now suggests a smartphone app that assists users in tracking their mood and function may help to reduce relapse risk in some patients with bipolar disorder.
“Smartphone-based interventions provide a promising means for increasing access to self-management strategies derived from bipolar disorder psychotherapies,” wrote Evan Goulding, M.D., Ph.D., and colleagues. Goulding is an assistant professor of psychiatry and behavioral sciences at Northwestern University Feinberg School of Medicine.
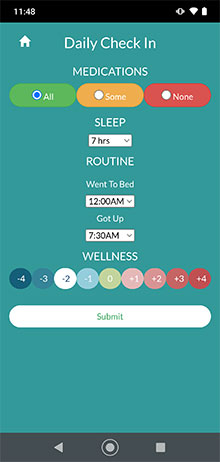
The smartphone intervention that Goulding and colleagues tested is called
LiveWell, a coach-supported app that monitors daily medication adherence, sleep duration, routine, and wellness levels. Based on this information, the app provides feedback, directs users to relevant app content, and encourages outreach to mental health professionals when needed.
LiveWell helps users track their highs and lows over the course of a day, Goulding told Psychiatric News. Such daily check-ins can help people to identify warning signs of a potential manic or depressive episode (for example, repeatedly getting up later than usual) and take early action. LiveWell also offers trained coaches who encourage the use of the app, review the app data, and offer feedback.
“The coach serves as a concierge in a way,” Goulding explained. “They may notice someone is becoming withdrawn and direct the user to app content that says ‘don’t turn down offers to do things,’ and help [the user] make a plan to be more active.”
To test whether patients with bipolar disorder benefitted from use of LiveWell, Goulding and colleagues recruited adults with bipolar disorder I. To be included in the study, the patients had to have experienced an acute mood episode within the past two years, but not be currently experiencing a manic, depressive, or mixed episode, according to DSM-IV criteria. Of the 205 people enrolled in the trial, 124 received access to the LiveWell app in addition to their usual care, which could include medications, psychosocial interventions such as bipolar psychoeducation, and/or light therapy. The other 81 participants in the study continued with their usual care alone (control group).
The participants who were assigned to LiveWell were asked to use the app daily for 16 weeks. During this time, they met face-to-face with a coach for training on how to use the app and completed six follow-up phone calls with the coach (after 1, 2, 3, 4, 6, and 16 weeks). The participants continued to have access to the app and support as needed for 32 more weeks after the 16-week active intervention ended.
At 48 weeks, 29.6% of the participants in the LiveWell group and 42.9% in the control group experienced a relapse (a new manic, depressive, or mixed episode). Though lower, the relapse rates in the LiveWell group were not statistically superior to those of the control group.
When examining the data from the participants who were classified as being at low risk for relapse at the start of the study (defined as no moderate symptoms at entry and two or fewer moderate symptoms over the previous eight weeks), differences between the groups emerged: After 48 weeks, only 12.1% of low-risk participants using LiveWell experienced relapse, compared with 37.2% of low-risk participants with usual care alone.
“These results were not totally surprising. Previous research has shown that adjunctive therapies like talk therapy may work better for patients with a lower risk of relapse,” Goulding said. “About 40% of our participants [met the criteria for] low risk, so it gives me hope this app could work for many patients in the real world.”
“I am always excited to see an evidence-informed mental health app take a step forward toward public use,” said Emma Morton, Ph.D., a postdoctoral researcher at the University of British Columbia’s CREST.BD, a collaborative network of researchers, people living with bipolar disorder, health care providers, and family members and supporters. Morton also works with digital mental health interventions and is currently conducting studies of people using
PolarUs—an app that enables people with bipolar disorder to monitor their quality-of-life ratings and identify avenues for improvement.
Morton lauded LiveWell’s focus on developing personalized wellness plans for users, which may have helped boost long-term engagement with the app (68% of users participated in all six coaching calls). “But while the coaching is a strength, it can also be a barrier to scalability,” she said. “Not all health systems can meet the needs of this app.”
Goulding conceded that questions about the app remain. For one, the LiveWell platform includes a secure website with detailed summaries of participants’ daily and weekly reports, but only a quarter of the participants accessed this resource. In addition, the participants assigned to the LiveWell group had the option of allowing their mental health providers access to the website, but only 32 of the 105 care providers contacted agreed to participate. He said that he believes a tool like LiveWell would work best when the patients, their care professionals, and coaches are all engaged.
This study was funded by a grant from the National Institute of Mental Health. ■