Mental health help-seeking behavior in a native African society usually involves a household decision-making process, very often influenced by the community's concept of mental illness (
1). Usually, the relations of individuals with a mental illness decide on their behalf where to seek help. A community's belief system about the causes of mental illness influences a family's opinion about the likely cause of mental illness experienced by a family member (
2).
Furthermore, many African societies believe supernatural forces cause mental illness, and this affects the choice of mental health healers. In general, the choices of mental health healers in Western countries sharply contrast with those in Nigeria, where most psychiatric patients consult nonmedical alternative mental health healers (
2,
3). In addition, religion plays a great role in most modern Africa societies and fortifies a belief in an all-powerful creator and carer to whom one supplicates in times of need (
2,
4–
6). In such societies, many psychiatric patients and their relations (
2,
6) usually see religious clerics first.
Unfortunately, efforts to raise awareness among primary health providers in Nigeria about the importance of treating mental illness have not progressed. The National Strategic Health Development Plan, launched in 2010, did not include raising mental health caring standards as a priority (
7). Therefore, primary health providers in Nigeria may not detect or properly manage psychiatric problems experienced by their clients. Yet early and appropriate treatment minimizes the negative biological and psychosocial impact of psychiatric illnesses (
8).
This cross-sectional study investigated the types of healers that psychiatric patients and their relations visited before seeking treatment from the mental health services at the Aminu Kano Teaching Hospital. It examined associations between the beliefs of the patients and their relations about the cause of illness and the types of healers they had visited.
Methods
The study was conducted at Aminu Kano Teaching Hospital, a well-utilized tertiary health care facility in northwestern Nigeria. The hospital is located in a metropolitan area of about 3.5 million adults. A psychiatry outpatient clinic runs thrice weekly, and teaching rounds are held twice weekly.
Patients who came to the hospital for psychiatric consultations between April 1 and September 30, 2008, were eligible for inclusion if they had never used the hospital's psychiatric services in the past and consented to be interviewed. The study received approval from the hospital's ethics committee. The respondents were informed that their responses would be kept confidential.
Data were collected by an interviewer with a 17-item questionnaire similar to the encounter form used by the World Health Organization in its pathway studies. The encounter form was previously used in a similar study in western Nigeria (
2). The first sets of questions were about basic demographic characteristics such as sex, religion, tribe, age, place of residence, and educational status. This section also documented patients' file numbers and the patients' consent to use them for easy retrieval of information from the patients' file.
The main section of the questionnaire asked about the informant, when illness was first noticed, the patient's
ICD-10 diagnosis (
9), and the types of healers seen before coming to the hospital's mental health facility. Two questions asked about the initiator of the patient's first treatment contact and about beliefs of the patients and their relations about the cause of illness. The questionnaire was pretested with 15 consenting patients and their relations, who found the questions easy to understand. Administration of the questionnaire took between ten and 15 minutes. The questionnaire was administered by the trainee psychiatrists and the consultant psychiatrists either during an outpatient clinic period or—if the patient was admitted—on the accident and emergency unit.
Data were analyzed with SPSS, version 10, statistical software (
10). Absolute percentages were used to summarize categorical values, and summary statistics (means and standard deviations) were used to describe quantitative data. Tests of association were determined with chi square analysis.
Results
All new patients (N=219) who came for treatment within the period of the survey consented to the interview. A majority (N=216, 99%) were Muslims and members of the Hausa-Fulani ethnic group. The sample had a mean age of 30.9±11.4. A total of 140 (64%) were females, and 153 (70%) resided in the city of Kano. Among the patients, 164 (75%) were in secondary school at illness onset, and 161 (98%) had not completed their secondary education. Another 22 (10%) patients had enrolled in a tertiary institution but had interrupted their education, and 33 (15%) patients had only a primary education. Among the 217 informants whose identity was noted, 185 (85%) were the accompanying relations of the patients, 22 (10%) were patients, and ten (5%) were both patients and relations who corroborated to provide the illness history. The mean duration of illness before the psychiatric consultation was 4.5±1.6 years.
Schizophrenia was the ICD-10 diagnosis for 114 (53%) patients; 74 patients (34%) had bipolar disorder, 20 (9%) had unipolar depression, nine (4%) had somatoform disorder, and two (1%) had unspecified psychosis. A cross-tabulation analysis of data from 215 patients that compared the interval from illness onset to the time of receiving orthodox treatment and the type of illness was not statistically significant. In the course of illness, 62 (28%) respondents had gone to a traditional mental health healer, 152 (69%) had visited religious healers, 52 (24%) had consulted general practitioners, and six (3%) had consulted other health professionals.
For 186 (86%) patients, contact with the first healer was started by the patients' relations; six (3%) first contacts were initiated by patients, followed by 13 (6%) by family friends and 12 (6%) by general practitioners.
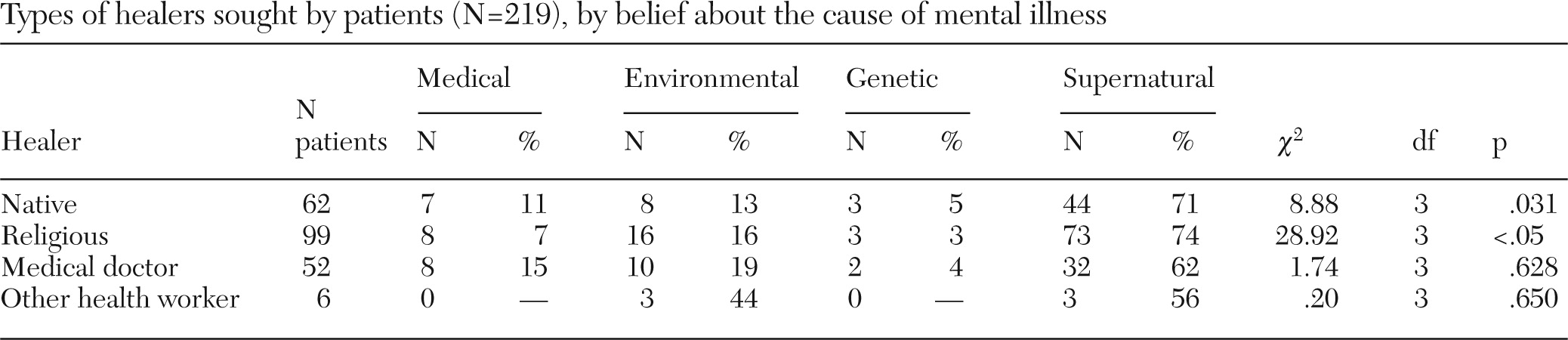
Most (N=152, 69%) respondents felt the illness was caused by supernatural forces, 36 (16%) and 23 (11%) felt the causes were due to environmental or medical problems, respectively, and eight (4%) felt the cause was genetic. A cross-tabulation analysis of belief about the cause of illness and the first type of healer seen showed that 44 (71%) of the 62 respondents who consulted a native healer believed that the illness was due to supernatural forces. Likewise, 73 (74%) of the 99 respondents who sought religious healing attributed the illness to supernatural forces. Belief about the cause of illness by the patients and their relations was significantly related to seeking native or religious care in the course of illness (p<.05) (
Table 1). Eighteen (78%), six (75%), and 20 (54%) respondents who believed in medical, genetic, and environmental causes of mental illness, respectively, but only 46 (30%) who believed in environmental and supernatural causes, respectively, had psychiatric consultations within six months of illness onset. On the other hand, 106 (70%) respondents who believed in a supernatural cause of illness consulted a psychiatrist within five years of illness onset.
Discussion
Findings from the study showed that most patients were in their late adolescence or early adulthood at the time of illness onset and were not in school. Usually, the patients' relations offered the history. Schizophrenia was the diagnosis for more than half of the patients. None of the patients first sought treatment from a psychiatrist, and the mean length of illness before psychiatric evaluation was more than four years. Usually the relations recommended and started the first treatment contact.
More than seven in ten patients received treatment from native and religious healers in the course of the illness. More than three in every five respondents, and a majority of those who sought traditional or religious healing, believed in the influence of supernatural forces on the cause of illness. Even among those who saw a general practitioner or a health worker at the onset of illness, more than half believed in a supernatural cause of illness. Notably, many respondents who felt the illness had a medical or genetic cause came for psychiatric consultation within six months of onset versus fewer than half of those who felt the cause of illness was environmental or supernatural. About half of those who believed in supernatural causes of illness and one-third of those who believed in environmental causes came for psychiatric consultation within five years of onset. Fewer than one in 20 respondents who attributed the cause of illness to genetic or medical factors came for psychiatric consultation within five years of onset.
These findings relate to those of similar studies conducted earlier in other parts of Nigeria. Abiodun (
11) claimed that 95 (40%) respondents reported that their first mental health contact was a traditional or religious healer, and decisions were made mainly by the relations of the patients. Gureje and others (
2) found that traditional and religious healers were consulted by many respondents and that a large proportion of patients consulted such healers first. However, Patel and others (
12), in Zimbabwe, claimed that psychiatric patients consulted biomedical practitioners first, mainly, but consulted traditional and faith healers when biomedical treatments failed. In Ghana, patients residing in urban areas consulted first with pastors, followed later by traditional mental health healers and last by providers of orthodox psychiatric treatment (
13). In that study, many respondents came for orthodox treatment when religious healing was unsatisfactory. However, this pattern did not seem to affect their beliefs in the role of spiritism in their illness. A study of 134 Malayan psychiatric patients showed that on the basis of their beliefs and those of their relations and friends, 69% had visited traditional healers, or
bomoh, for treatment and had consulted a psychiatrist only after a significant delay (
14).
In Europe, most psychiatric patients and their relations believe in the biological and environmental causes of mental illness (
3). Therefore, most patients seek psychiatric care through general practitioners, direct access, and hospital doctors. A Japanese finding mirrors that of Europe, given that a majority of patients had access to psychiatrists directly or through general hospitals (
15). However, patients who went first to nonpsychiatrist formal mental health healers took longer to consult a psychiatrist than those who did not seek out nonpsychiatrists.
Results from the study indicate a delay in seeking orthodox mental health care by a high percentage of respondents who believed in the spiritual etiology of mental illness. These findings emphasize the strong role played by both native existential ideologies and modern religious doctrines in a community's belief in the active influence of spirits, evildoers, demons, jinn, or other supernatural creatures in illness causation. Moreover, common psychiatric disorders often lack discernible pathologies. Nonetheless, treating complex mental and emotional problems with only prayers or other forms of spiritual healing appears too simplistic and is likely an ineffective care practice.
The predominance among the respondents of one religion and the collection of data from one hospital unit possibly affected the results of the study. Because of the prolonged delay between illness onset and treatment seeking at the hospital, response bias when giving the history of illness probably occurred. The generalization of the findings to other psychiatric problems is limited because most respondents had received a diagnosis of schizophrenia or bipolar disorder. Accessibility to the study hospital should not have been a significant hindrance to the respondents' first choice of healer because a majority of the respondents had easy access to the hospital's services. However, it is important to note that an earlier study in Nigeria by Gureje and others (
2) found that access to place of care was not a significant factor in the first choice of healer.
Conclusions
Findings from this study showed that a community's belief in the influence of supernatural forces in psychiatric illnesses was related to the first choice of healer. Therefore, raising awareness about mental illness among alternative mental health healers and family members of people with mental disorders would improve mental health services in such societies.
In addition, mental health policy makers should encourage mental health healers to provide realistic psychoeducation to patients and their relations in the course of treatment to improve their understanding of the illness.
Acknowledgments and disclosures
This research was funded by the management of Aminu Kano Teaching Hospital.
The author reports no competing interests.