In the 1980s, a new point of view on recovery emerged in psychiatry, based on the consumer's perspective (
1). From this perspective, the focus is not on traditional (medical) outcomes but on individually defined and more subjective constructs, such as personal growth, hope, and autonomy (
2). Several concepts are commonly regarded as important to recovery: empowerment, hope and optimism, life satisfaction, self-esteem, connection with others, social relationships, and social support (
1,
3–
8).
A potentially powerful tool to enhance the recovery of people with major psychiatric problems is peer support. Several studies have shown that peer support improves symptoms, reduces hospitalizations, offers hope, facilitates coping, and increases social networks and quality of life among people with severe psychiatric disorders (
9–
12). Peers also have the potential to engage people with serious mental illness in services (
13). Moreover, most people with mental disorders do not get professional help, although many need care (
14).
Peer-run services have expanded rapidly during the past two decades (
15,
16), and the increasing popularity of these services illustrates the demand for this type of intervention. Despite the advantages of peer-run services, they are still not generally provided as a mental health service, and research on the effectiveness of, for example, self-help groups has been limited and poorly controlled (
15,
17,
18). Few studies have assessed the effects of peer-run interventions on recovery of people with major psychiatric problems (
19–
22). Two randomized controlled trials have found positive effects (
19,
22).
The aim of this longitudinal study was to evaluate in a randomized controlled trial the effects of a peer-run course on the recovery of people with major psychiatric problems in the Netherlands. Self-report instruments were used, because recovery implies a subjective state (
2). At the time of the study, no Dutch instrument was available to measure recovery. In line with other studies, four key elements of recovery were measured: hope, quality of life, self-efficacy beliefs, and empowerment (
1,
3,
5). These key elements reflect the internal conditions or life satisfaction of individuals who are recovering (
1). Furthermore, loneliness was measured because several studies have shown that social relationships support recovery (
1,
3,
6–
8). The hypothesis was that the peer-run course would result in higher levels of recovery.
Methods
Participants
Recruitment took place in the Netherlands between September 2006 and July 2008. People with major psychiatric problems were recruited by fellow clients involved in the research project; by means of advertisements in free local papers and posters in hospitals, psychiatric care services, and primary care settings; and by mental health care providers. Two inclusion criteria were used: self-reported psychosis, personality disorder, affective disorder, anxiety disorder, addiction problems, eating disorders, or other psychiatric problems; and self-report of having experienced disruptive periods in life from which the person was recovering. Exclusion criteria were illiteracy, inability to speak Dutch, suicidal ideation, florid psychotic symptoms, or substance abuse during the peer-run course. To determine whether persons were eligible to participate in the study, they were interviewed by course instructors and their supervisors on admission to the course.
Procedure
At the time of the study, the course was organized at 18 mental health care institutions and patients' associations in the Netherlands. Clients of 13 of these organizations were eligible for study participation. Although most eligible clients participated, a minority took part only in the course because they did not want to participate in the study. The study was explained orally and in writing to each participant, and written informed consent was obtained. At each organization, participants were invited to meet with the researchers and research assistants and asked to complete several questionnaires. Participants who could not attend the meeting returned the questionnaires by mail. All participants were paid ¢7.50 for the assessment session.
At baseline, participants were randomly assigned to the experimental or control condition by a research assistant who drew lots. Participants were assigned numbers so that researchers and research assistants were blind to their condition. Data for participants in both conditions were gathered simultaneously in one meeting at baseline and at three months and six months. Participants in the experimental condition started the course within one week after randomization and completed the course in three months. Thus the effect of the intervention was evaluated by comparing recovery among persons in the experimental and control conditions at three months and assessing whether any difference persisted at six months (three months after course completion). Participants in the control group enrolled in the course at six months (that is, after participating in this study). [Results of the intervention for the control group are presented in an online appendix to this report at
ps.psychiatryonline.org.]
Individuals in both conditions were free to participate in other recovery-related activities and continued their treatment as usual. Before the study began, approval was obtained from the Medical Ethics Committee for mental health institutions in the Netherlands. The trial registration number was ISRCTN47331661.
Intervention
The course “Recovery Is Up to You” was developed in 1996 by clients and two mental health professionals. It consists of 12 weekly two-hour sessions. Each group was led by two trained course instructors who had previously participated in the course themselves and who had then successfully completed a train-the-trainer course—that is, they received on-the-job training and learned by experience while working with experienced course instructors. The course instructors were employed either at the Knowledge Center for Self Help and Consumer Expertise or at one of the participating organizations. To become a course instructor, individuals had to be in an advanced state of their recovery process—that is, they had to be living “beyond their illness” (
23). Instructors closely followed a standardized manual, which precisely described the goals of each session and the steps to attain the goals. Each session had the same structure and was organized around a specific, recovery-related theme. Themes were the meaning of recovery to participants, personal experiences of recovery, personal desires for the future, making choices, goal setting, participation in society, roles in daily life, personal values, how to get social support, abilities and personal resources, and empowerment and assertiveness. The participants used a standardized workbook that described the theme of each session and contained assignments for the session and homework assignments. Themes were discussed in a group setting, individuals shared experiences, and skills were practiced. Important elements of the course were the presence of role models, psychoeducation and illness management, learning from other's experiences, social support, and homework assignments.
To assess protocol adherence, course instructors in the study were asked to complete a checklist after each session. On a 10-point scale they indicated to what extent they had adhered to aspects of the protocol, such as structure and content, and whether the goals of the session as described in the manual had been met. The checklist also evaluated process-related aspects, such as the atmosphere and social support in the group (
24).
Outcome measures
We assessed hope with the Herth Hope Index (HHI), which consists of 12 items with scores ranging from 1, strongly disagree, to 4, strongly agree (
25,
26). The Dutch version has a Cronbach's alpha of .84 and a one-week test-retest reliability of .79; its construct validity was satisfactory, with medium to large correlations in the expected direction (
26).
Quality of life was assessed with the 12 subjective items of the Manchester Short Assessment of Quality of Life (MANSA); the items use a 7-point Likert scale, from 1, could not be worse, to 7, could not be better (
27,
28). Cronbach's alphas ranged from .73 to .85 in various samples (van Nieuwenhuizen C, Nugter A, Priebe S, unpublished manuscript, 2011).
Self-efficacy beliefs were measured with the 16-item Mental Health Confidence Scale (MHCS), which uses a 6-point Likert scale from 1, totally no confidence, to 6, full confidence (
29,
30). Cronbach's alpha was .93, and the scale's validity was satisfactory, with correlations ranging from medium to large (
30).
Empowerment was assessed by using a newly developed instrument, the Dutch Empowerment Scale (
31). The scale consists of 40 items with a 5-point Likert scale ranging from 1, strongly disagree, to 5, strongly agree. Cronbach's alpha was .93. Correlations with related instruments ranged from small to large in the expected directions, indicating satisfactory construct validity (
31).
Loneliness was assessed with the Loneliness Scale, which consists of 11 items with a 5-point Likert scale ranging from 1, yes, for sure, to 5, no, certainly not (
32,
33). Cronbach's alpha ranged from .8 to .9 (
33). Correlations with related scales ranged from small to large in the expected direction (
34).
On all instruments, except the Loneliness Scale, higher scores indicate more recovery. In this study, we used the mean item scores as dependent variables in the analyses. Cronbach's alphas from baseline to six months ranged from .85 to .88 for the HHI, .84 to .88 for the MANSA, .91 to .94 for the MHCS, .93 to .95 for the Dutch Empowerment Scale, and .90 to .93 for the Loneliness Scale. For all instruments, missing values were treated as described in the manual for each scale.
Statistical analysis
For both conditions, means and standard deviations were calculated at baseline and the two follow-ups for the four recovery outcomes and for loneliness. Cohen's d (
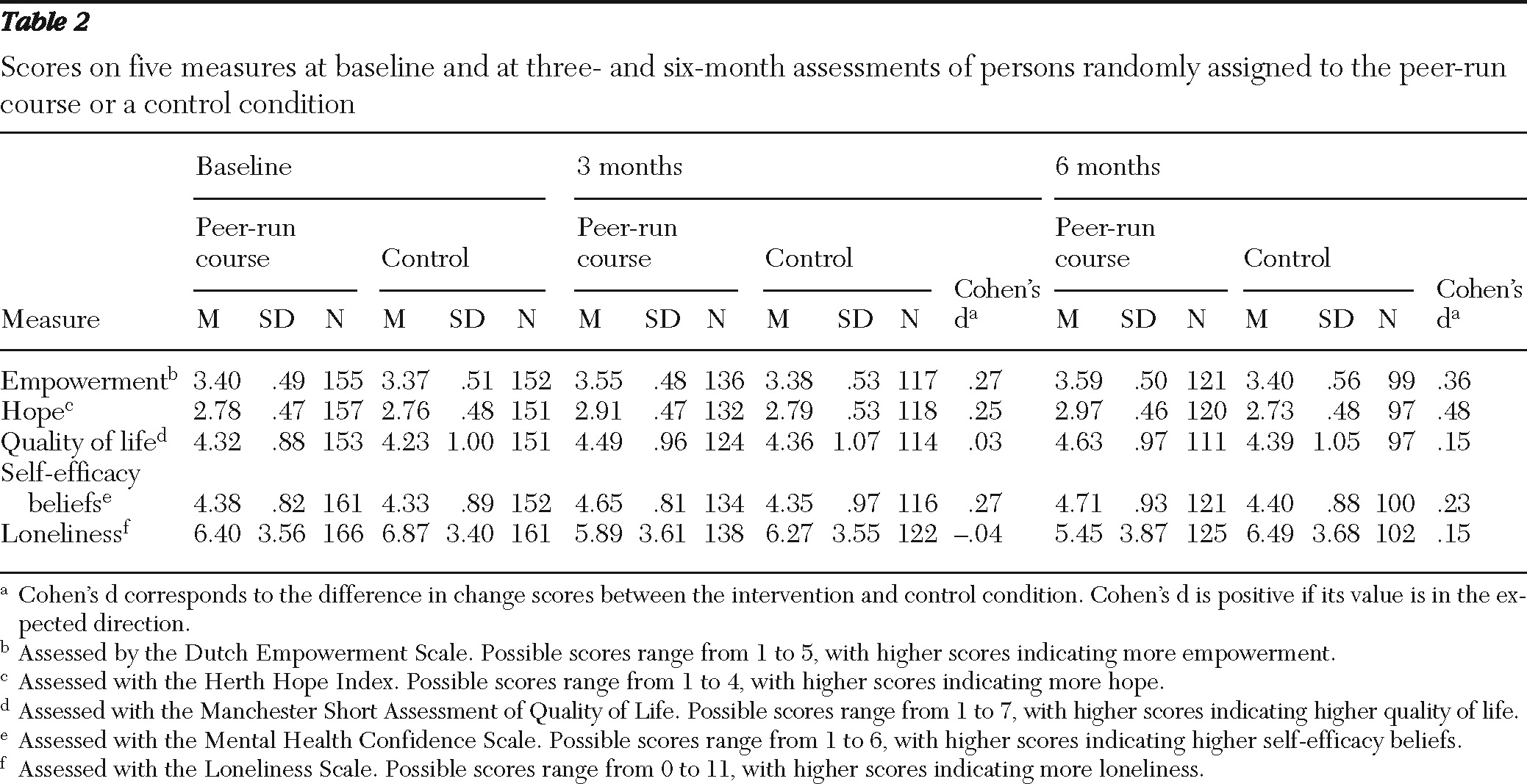
35) was calculated by using the change scores from baseline to assess the effect of the course at three months and the persistence of the effect three months after the course. Power analysis indicated that at least 50 participants in each condition were needed to obtain a power of .8 to detect a moderate effect size of d=.5, at a significance level of .05.
The data had a three-level structure. Occasions were nested in individuals, and individuals were nested in groups attending the same course. Multilevel analyses with these three levels revealed that 6% or less of the variance was explained by the third-level group. Therefore, group was not included as an additional level in our final analyses. Intraclass correlation coefficients as measures of the systematic individual differences in recovery are reported below.
The effects of the intervention on recovery were estimated by using linear mixed modeling. This approach is superior to more traditional methods, such as repeated-measures analysis of variance and multivariate analysis of variance (
36). For instance, unlike the traditional methods, linear mixed modeling can accommodate missing values and time-varying covariates and has been found to yield relatively few statistical errors when missing outcomes are missing at random (
37).
Hypotheses were tested with mixed modeling by using maximum likelihood of the procedure MIXED in SPSS, version 17.0. In all analyses an unstructured covariance matrix for the dependence structure was estimated. The unstructured covariance matrix makes no assumptions about the dependency structure of the data and at the same time ensures accurate p values of tests of the effects of interest. First, an overall test was conducted of differences in recovery between the control and experimental conditions by comparing the fit of the model with factor time to the fit of the model with time, condition, and time × condition, using a likelihood ratio or deviance test. The latter model incorporated two interaction contrasts. One assessed whether the intervention had an effect on recovery at three months, and the other assessed whether the intervention had an effect on recovery at six months. The interaction contrast tested whether the change in recovery from baseline in the intervention condition was different from the change from baseline in the control condition. We also assessed whether the effect of the intervention at six months was different from the effect of the intervention at three months by testing the difference between the two interaction contrasts.
In addition, we tested whether background variables (gender, age, education, and marital status) and attendance rates had an effect on the dependent variables and whether the effect of the intervention interacted with disorders (psychotic, affective, anxiety, and personality disorder). Because no such effects were observed, the results of these tests are not reported.
Results
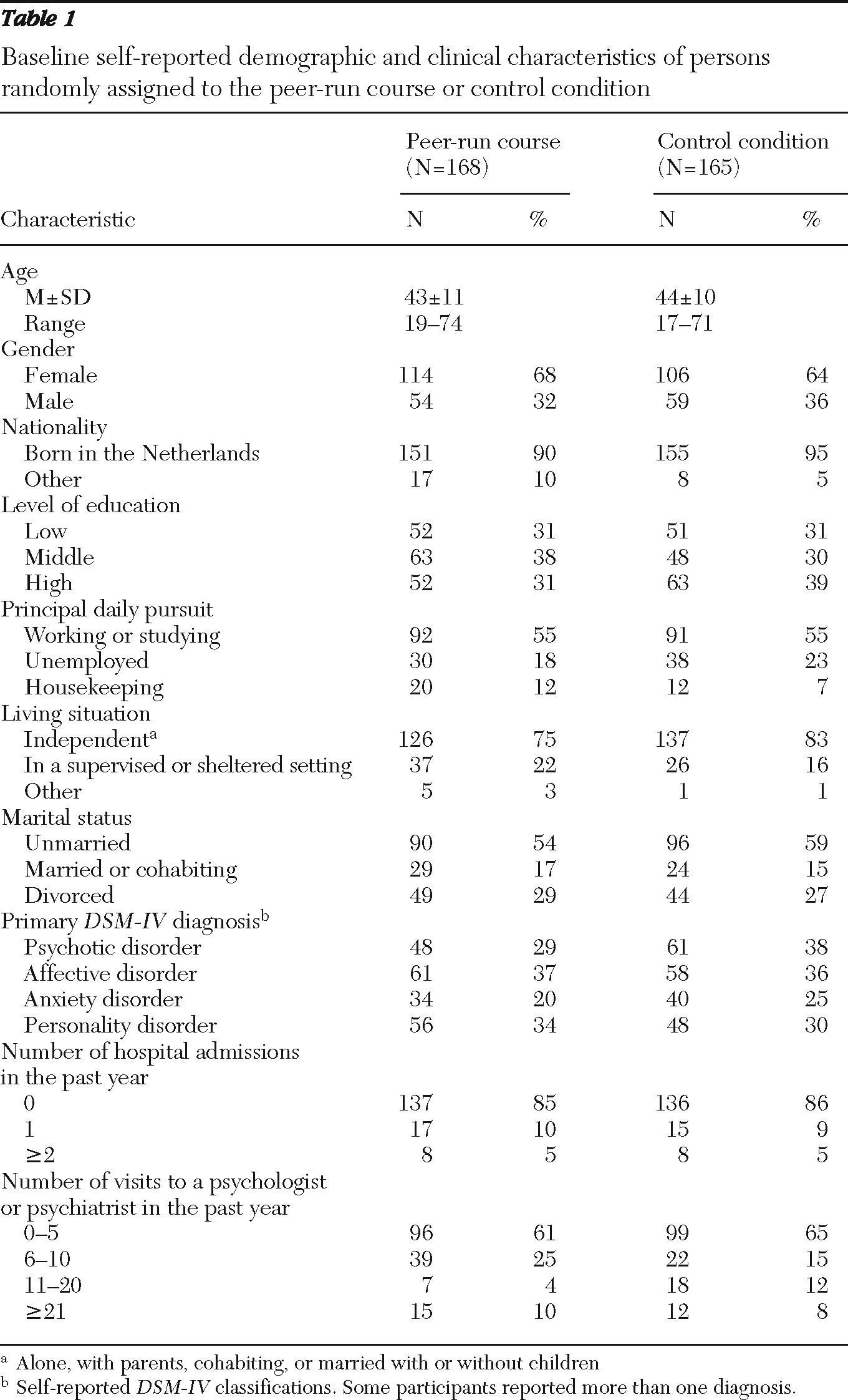
Of the 333 participants, 168 were randomly assigned to the experimental condition and 165 to the control condition. Demographic and clinical characteristics of the two groups are summarized in
Table 1. Chi square tests of independence and t tests showed no significant differences at baseline in demographic and psychiatric characteristics between persons assigned to the two conditions. Nine persons assigned to the peer-run course did not attend any sessions, and two dropped out. Fifteen persons did not accept random assignment to the control condition and participated in the course, and two persons assigned to the control condition dropped out of the study. Overall rates of dropout from the study were 20% and 30% at three and six months, respectively, with significantly more dropout in the control condition than in the experimental condition (35% versus 25% at six months, p=.01). Those who dropped out, however, did not differ on background variables from those who did not drop out. [A flowchart showing recruitment and study assignment is included in the online appendix at
ps.psychiatryonline.org.]
Course participation
In total, 38 separate 12-week courses were provided. Each location had its own course instructors. A total of 37 instructors were involved in the study. The mean±SD number of participants per course was 7.0±2.1 (range of three to 12). Participants attended a mean of 9.0±3.3 sessions (range of one to 12). Checklist results indicated that the course instructors' adherence to the protocol was high (
24,
38). At three months, 57%(N=80) of participants in the experimental condition reported that they had sought information on recovery outside the peer-run course and 26% (N=36) participated in other recovery-related activities, compared with 51% (N=63) and 10% (N=12), respectively, of persons in the control condition.
Preliminary analyses
The means, standard deviations, sample sizes, and Cohen's d for all measures at baseline and the two follow-up assessments are shown in
Table 2. The average correlation between the outcome measures was .67 at baseline, .76 at three months, and .77 at six months. The effect of the intervention (Cohen's d) was small to moderate on empowerment and hope and small on self-efficacy beliefs, quality of life, and loneliness. A total of 920 observations for 327 participants were used for the mixed modeling analyses.
Mixed modeling
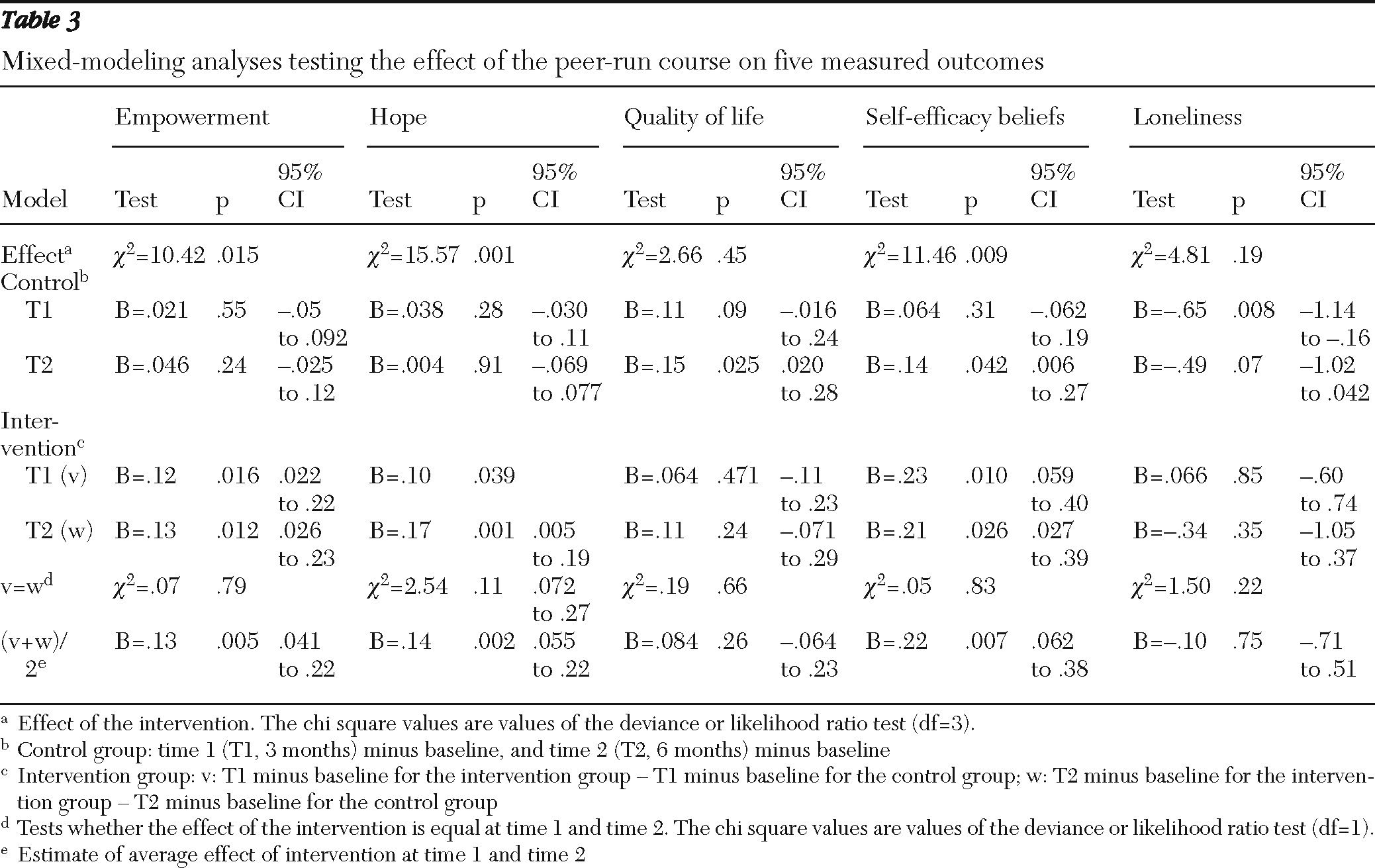
The intraclass correlation coefficients for the dependent variables were between .70 and .76, indicating large systematic individual differences in recovery. The intervention had a significant effect on empowerment, hope, and self-efficacy beliefs but not on quality of life and loneliness (
Table 3, row 1). Data for participants in the control condition indicated less loneliness at three months and greater recovery as measured by quality of life and self-efficacy beliefs at six months. Data for intervention participants indicated greater recovery at three and six months compared with persons in the control condition as measured by scores on empowerment, hope, and self-efficacy beliefs. The effect of the intervention at three months was not significantly different from its effect at six months. The combined effect of the intervention at three and six months was significant (p<.01) as measured by empowerment, hope, and self-efficacy beliefs.
Discussion
In a randomized controlled trial the effects of a peer-run course on recovery were longitudinally assessed in a large sample of persons with major psychiatric problems. Confirming our hypothesis, we found a positive effect of the peer-run course on participants' empowerment, hope, and self-efficacy beliefs. These effects persisted until at least three months after the intervention and were observed for participants in the control condition after they completed the peer-run course (see online appendix). No effect of the intervention on quality of life and loneliness was found.
The effects of the course on important elements of recovery—empowerment, hope, and self-efficacy beliefs—are comparable to effects found in three recent studies. Two of these studies also assessed the effects of a 12-week, peer-run intervention for people with major psychiatric problems. One of these studies, a randomized controlled trial with a total of 33 participants, found effects on hope, empowerment, and recovery (
22). The second study, which had a total of 47 participants and was not a randomized trial, showed improvement for participants in self-esteem, self-efficacy, spiritual well-being, social support, and psychiatric symptoms (
21). The third study was a recent randomized controlled trial with 519 participants in which an eight-week, peer-run, illness self-management intervention focusing on recovery showed effects on participants' symptom severity, hopefulness, and quality of life (
19). These outcomes underline the importance of peer-led interventions for recovery of people with major psychiatric problems.
Several factors can account for the effects of the peer-run course assessed in this study: the presence of role models and sharing of personal experience in dealing with serious mental illness (
10,
12,
15,
39) and elements of psychoeducation and illness management, which are well-known evidence-based methods (
40). Peer education, peer support, and a clear structure of the intervention are also common elements of peer-run interventions that have yielded similar results.
Fellow mental health clients played a considerable role in the recruitment procedure, and most people participated in the study on their own initiative, which may have resulted in a less disabled population than if recruitment had been conducted only by professionals. For instance, participants visited their psychiatrist on average seven times in the previous year and reported few hospital admissions in the past year. Moreover, only about 20% resided in sheltered living, and more than 50% of the sample was working or studying.
It is of interest that no effects of the intervention were found on loneliness or quality of life. It may take a longer time before loneliness decreases and social networks are developed, as was found in other studies of self-help groups and peer support (
11,
12).
Several limitations of the study need to be addressed. Methodologically, the absence of a control condition in which participants received the same level of attention as the intervention participants means that the Hawthorne effect cannot be ruled out (
41). The intervention results may also have been affected by dropout of participants who were not motivated to attend the peer-run course. However, it is unlikely that these two factors are responsible for the positive effects found, because the effects were not found for all outcome measures and persisted for at least three months. Another limitation is that it is unclear precisely which ingredients contributed to the effect of the peer-run course and how often participants should attend the course to benefit from it. Further research on peer-run services is necessary to obtain greater knowledge about the ingredients that are useful for recovery. Third, all instruments were self-report. Although subjective outcome measures were deliberately chosen, more objective outcome measures, such as for employment, would have added valuable information. Fourth, although this sample of the Dutch population included people with major psychiatric problems, it is unknown whether the results can be generalized to populations of other countries or specific subgroups, such as people who are more severely disabled by their mental illness.
Conclusions
Participation in the peer-run course “Recovery Is Up to You” led to improvements in important domains of recovery—empowerment, hope, and self-efficacy beliefs—and these effects persisted for at least three months. Currently, peer-run services, such as “Recovery Is Up to You,” add value to recovery-oriented mental health services because they offer participants an opportunity to make an active start on their recovery.
Acknowledgments and disclosures
This work was supported by grant 100003017 from the Netherlands Organization for Health Research and Development (ZonMw). The authors honor Joop van den Bogaard, Ph.D., who passed away unexpectedly. He initiated the study and managed the research project for two years. The authors thank the study participants, the participating organizations, and especially Goris van den Langenberg, M.Sc., Leonie Kusenuh, and Sabine Smits.
The authors report no competing interests.