Homelessness has been a public issue in the United States since the early 1980s. It took two decades, however, and a major shift in viewpoint before attention focused on chronic homelessness—defined as long-term or repeated homelessness among single adults with disabilities. The first programs to offer permanent supportive housing, which has proved to be an important part of the solution, began appearing in the mid-1990s. By the early 2000s both the federal government and an increasing number of communities were committing themselves to ending chronic homelessness and using permanent supportive housing as their central strategy (
1).
As part of the federal government's commitment to end chronic homelessness, the U.S. Department of Housing and Urban Development (HUD) and various federal partners launched major demonstration projects in 2003 to identify effective approaches. One of these projects was Ending Chronic Homelessness Through Employment and Housing, a partnership involving HUD and the U.S. Departments of Labor (DOL) and Veterans Affairs (VA) (
2,
3). This demonstration brought together supported employment, an evidence-based practice with an extensive research history for housed people with serious mental illness (
4–
6), and permanent supportive housing, a practice with an equally impressive record of effectiveness (
7–
13) and cost-effectiveness (
14–
18) in the field of interventions to end homelessness. This initiative funded five projects, including Los Angeles' Homeless Opportunity Providing Employment, or LA's HOPE, the focus of this article. Supported employment programs mostly do not serve people who have long histories of homelessness or active co-occurring substance use disorders, and supportive housing programs normally deal with employment services for tenants only by referral. Combining these services in a housing and service delivery structure intended to move people with long histories of homelessness into housing and employment was an ambitious goal, not least because its success depended on establishing effective relationships among public and private agencies in three different systems—mental health, employment, and homelessness—without much history of joint work.
Five-year grant funding for LA's HOPE and the other four HUD-DOL demonstrations was awarded in late 2003; LA's HOPE operations approached a steady state in spring 2004. The program offered permanent housing, support services, and employment assistance to people who were chronically homeless. This target population would be considered “hard to serve” by anyone's definition, coming largely from the streets of the Skid Row area of Los Angeles (shelter use was sporadic at best), having a major mental illness but being unattached to the mental health system, having co-occurring substance use and chronic medical conditions, and having long histories of homelessness.
The structure of LA's HOPE
LA's HOPE involved four public agencies and their contract service delivery programs—the City of Los Angeles' Community Development Department (CDD), which runs the city's workforce development centers and was responsible for the employment-related and general case management aspects of the demonstration; the Los Angeles County Department of Mental Health (DMH), which was responsible for the mental health services component through three of its contract agencies; the Housing Authority of the City of Los Angeles (HACLA), which administered the HUD Shelter Plus Care certificates that provided rental assistance, and the VA Medical Center, which supplied a social worker. CDD sponsored the evaluation of LA's HOPE (
19).
Enrollment entailed several steps. CDD case managers housed at Goodwill Industries, one of CDD's workforce development centers, recruited prospective participants. Selection criteria included being chronically homeless, having an axis I diagnosis, and expressing an interest in being housed and employed. Candidates were referred to DMH for eligibility determination and, once deemed eligible for the program, were enrolled in one of the three contract mental health agencies as clients in a special state-funded program known as AB2034. This program provided supportive services and housing assistance to people with serious mental illness who were homeless or at imminent risk of homelessness (
20). Although technically AB2034 clients, participants in the LA's HOPE demonstration received substantially greater assistance with housing (including long-term rental assistance) and employment than clients of other AB2034 programs.
After AB2034 enrollment, participants got help to apply for a Shelter Plus Care certificate through HACLA and to locate and secure a suitable housing unit, which was usually an efficiency apartment. During the time between enrollment and moving into their own unit, which could take as much as two or three months, participants often received temporary housing.
Employment was the final step in program engagement. LA's HOPE had several avenues through which participants could move toward employment. Its own case managers helped participants prepare for employment and connect with the workforce development centers. In addition, each AB2034 agency had an employment specialist who was expected to work with LA's HOPE clients, the demonstration's case managers, and workforce development center staff to promote client employment. The demonstration project had resources to provide participants with training, work uniforms, equipment, and other work supports and could also support work readiness and supported employment activities if needed before clients sought competitive work. Each AB2034 agency was linked to two nearby workforce development centers that worked with LA's HOPE participants, providing accommodations as needed to help participants get the most out of center offerings. The intervention design also called for coordination among the CDD and Goodwill case managers and staff working with LA's HOPE clients at the AB2034 agencies and workforce development centers. [Details on program operations are available as an online appendix to this article at
ps.psychiatryonline.org.]
Methods
Design and participants
All LA's HOPE clients were enrolled in one of three of the county's 18 AB2034 programs, located in community mental health centers (CMHCs). All AB2034 programs reported preenrollment, enrollment, and postenrollment client data to the same statewide Caminar data system. A marker for the Los Angeles County programs designated LA's HOPE clients. The availability of Caminar data made it possible to construct a comparison group of clients in the remaining 15 AB2034 programs and to assess housing and employment outcomes for them and for demonstration clients using identical data fields, definitions, and reporting requirements. The groups included in the analysis were LA's HOPE participants who enrolled between July 1, 2004, and May 17, 2005 (N=56), and clients who enrolled in the remaining 15 AB2034 programs in the county during the same period (N=415).
All participants qualified for county mental health services—usually with an axis I diagnosis of schizophrenia or affective disorder. All were homeless at enrollment or at extremely high risk of homelessness—for example, by being about to leave a jail or hospital with no place to live and having been homeless before incarceration or hospitalization. DMH and the Los Angeles County Sheriff's Department collaborated to identify about-to-be-discharged inmates with mental illness who had been homeless at jail intake for the county's AB2034 programs. Finally, all participants were about equally likely to have a co-occurring substance use disorder.
Data and human subjects considerations
All data reported in this article were deidentified client-level data from the Caminar data system. After the Urban Institute and DMH reviewed the project and gave institutional review board (IRB) approval, the researcher and DMH staff agreed on selection criteria and the required data fields approved by the IRBs and conveyed them to Caminar system managers. Data on employment and housing were collected through June 30, 2007, giving each enrollee at least 13 months of follow-up. Caminar data for clients matching the selection criteria were extracted and sent to DMH, which deidentified the data and sent them to the researcher. No individual informed consent was obtained, nor deemed necessary by either IRB.
Analytic methods
All analyses reported here were done with Stata software. Because significant differences existed between the groups on many important variables, propensity score matching was indicated (
21–
23). Weights for comparison group data were derived from the odds ratios of the predicted probability of being in LA's HOPE versus the comparison group. The 11 variables in the analysis to predict LA's HOPE participation were the same as those used in the final analytic models. Weighting succeeded in reducing before-weighting baseline differences to nonsignificance between the groups on all 11 variables (
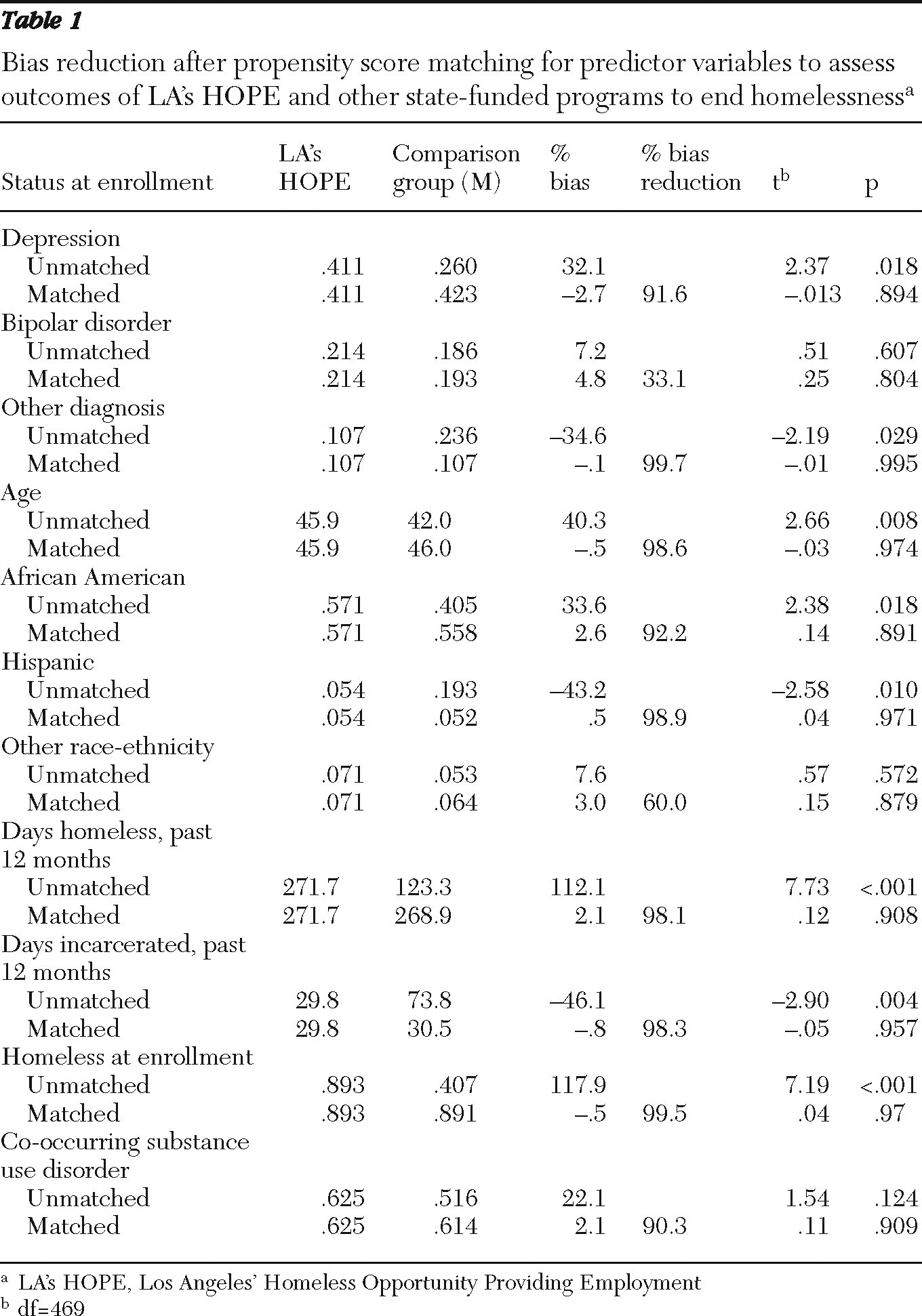
Table 1). Weighted models for binary dependent variables were run with logistical regression. Models for dependent variables reflecting time from enrollment to housing or to employment were analyzed with weighted Cox proportional hazard models to show the likelihood of the outcome at any given moment for LA's HOPE versus comparison group members. Weighted ordinary least squares regression was used to assess the effects of independent variables on continuous dependent variables (the average number of days a person spent in housing or employment).
Results
Baseline characteristics
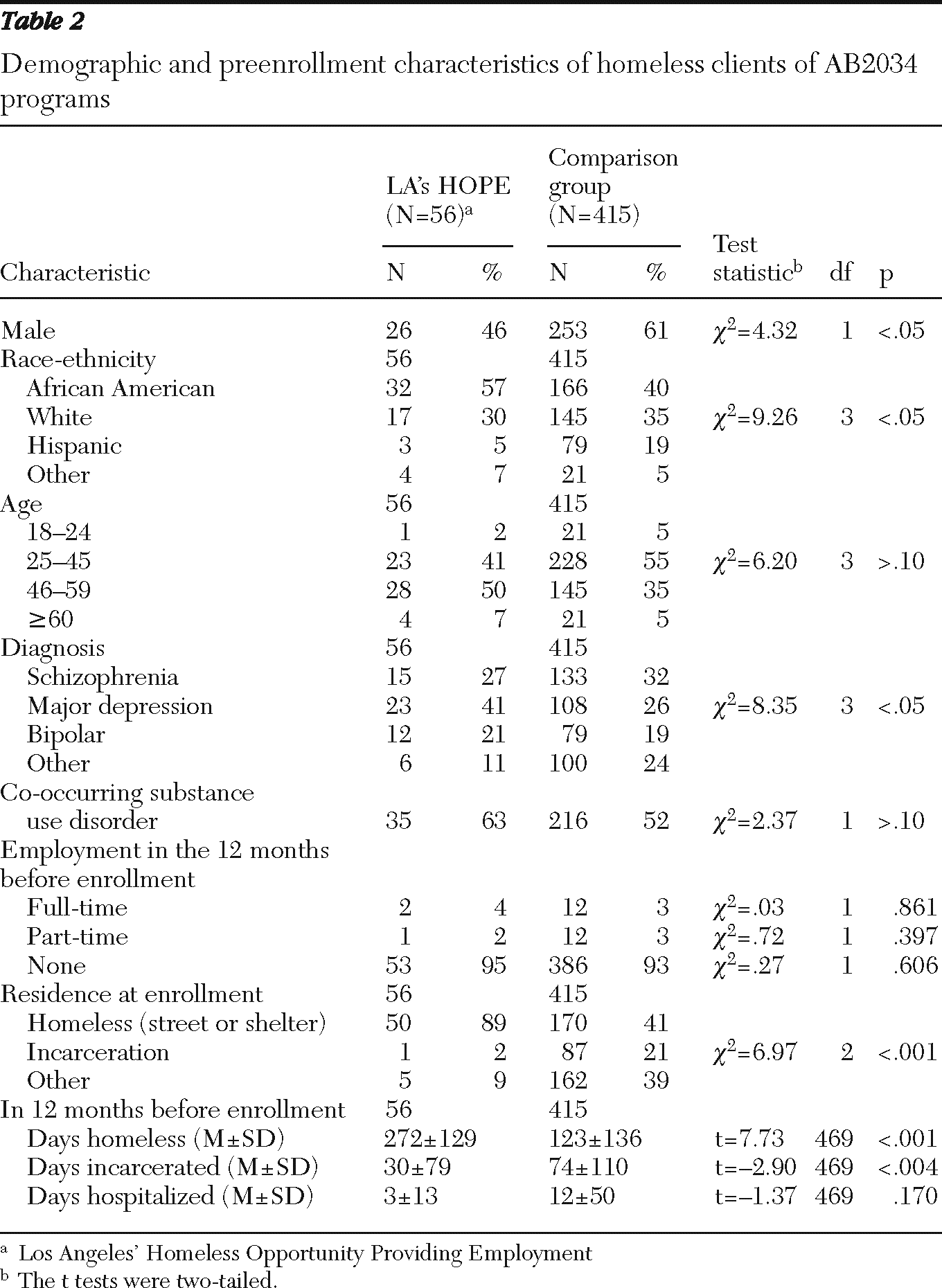
Table 2 shows demographic, diagnostic, and other preenrollment characteristics for the two groups. The groups were similar on age, the presence of a co-occurring substance use disorder, and preenrollment employment. They differed significantly on gender, race and ethnicity, axis I diagnosis (more LA's HOPE than comparison group clients had major depression or bipolar disorder and fewer had other diagnoses), homelessness at enrollment, preenrollment homeless days (greater among LA's HOPE clients), and preenrollment incarceration (greater for the comparison group).
Outcomes
Housing outcomes for LA's HOPE participants and members of the comparison group appear in
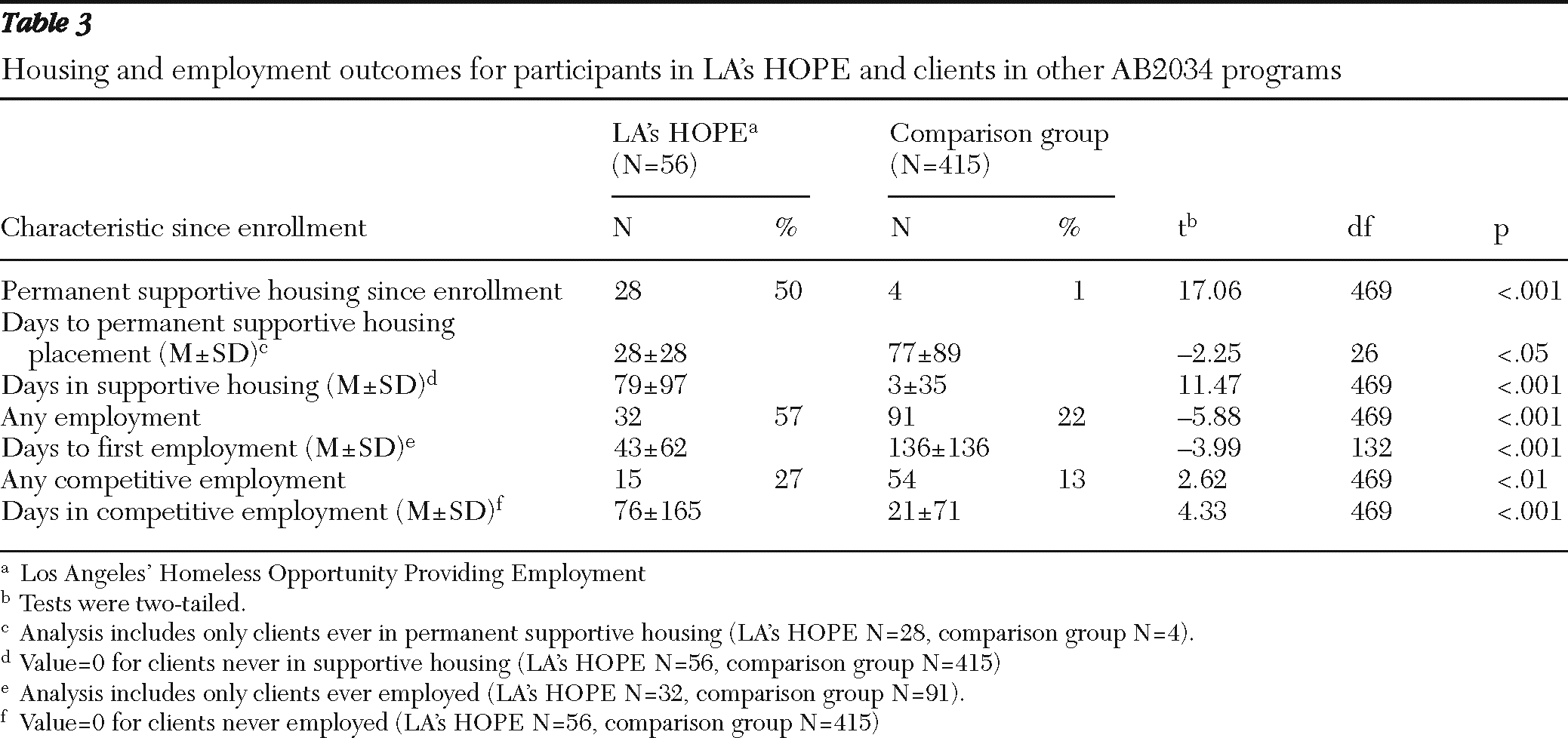
Table 3. Tenancy in permanent supportive housing was the housing goal for LA's HOPE clients; housing stability was also a primary goal of all AB2034 programs. Among LA's HOPE clients, 50% had lived in permanent supportive housing since enrollment, whereas only 1% in the comparison group had done so. LA's HOPE clients placed in housing took many fewer days after enrollment to move in than was true for the few comparison group members housed. Among those who were in supportive housing after enrollment, LA's HOPE clients spent far more days housed than comparison group members did (LA's HOPE mean±SD=79±97 days; comparison group 3±35 days).
With respect to employment, 57% of LA's HOPE clients participated in employment (27% in competitive employment) at some time during the demonstration period—rates more than double those of the comparison group (22% attaining any employment; 13% competitive employment) (
Table 3). This work rate is very high for any group of people with the characteristics of LA's HOPE participants. LA's HOPE participants were more likely to have worked in a full-time (not shown) or part-time job (not shown) and in a competitive position and were far less likely to have had no employment at all while in the program. The LA's HOPE participants who entered employment took fewer days postenrollment to do so and worked significantly more days in competitive employment than members of the comparison group. At least half of the days worked by LA's HOPE participants were in competitive employment, not sheltered or transitional jobs at the AB2034 programs or elsewhere (not shown). Thus LA's HOPE appears to have succeeded at one of its primary goals—increasing employment among formerly chronically homeless single adults with serious mental illness.
Factors affecting outcomes
The substantial differences in the groups' baseline characteristics were handled with weighting based on propensity score matching. Analyses examined whether group membership affected the outcomes and whether any individual client characteristics did so as well. DMH was particularly interested in whether a client's diagnosis made a difference, and it was also important to assess the independent effects on the core outcomes of a co-occurring substance use disorder, age, race or ethnic background, and experiences during the 12 months before enrollment.
Table 4 displays the results for housing outcomes;
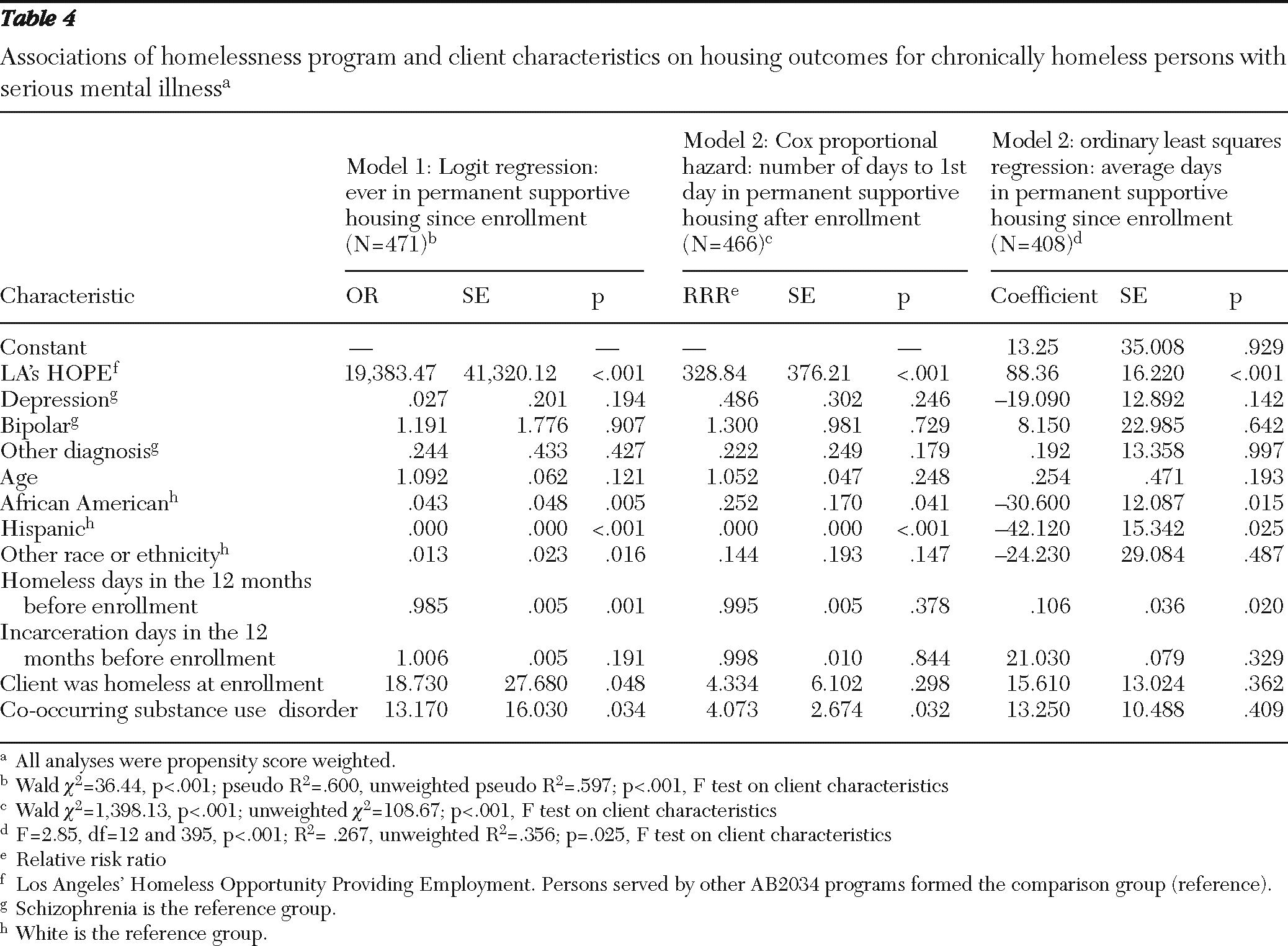
Table 5 does the same for employment outcomes. Being in LA's HOPE significantly improved the three housing outcomes—ever in supportive housing since enrollment, days to first day in permanent supportive housing after enrollment, and number of days living in permanent supportive housing (the latter only for those who entered supportive housing).
LA's HOPE clients were many times more likely than comparison group members to have lived in supportive housing since enrollment. The differences between the groups on time to housing placement and number of days spent living in supportive housing since enrollment were equally dramatic, with LA's HOPE clients being housed sooner and staying longer.
Housing outcomes were consistently affected by some client characteristics in addition to group membership. In particular, race-ethnicity affected all three outcomes. Compared with white clients, African-American and Hispanic clients were much less likely to have been in supportive housing since enrollment, took longer to receive that placement, and spent many fewer days in permanent supportive housing.
Two other client characteristics affected two of the three housing outcomes. The more days clients spent homeless in the 12 months before enrollment, the less likely they were to move into supportive housing and the less time they spent there. Also, clients with a co-occurring substance use disorder were more likely than those without to have lived in supportive housing since enrollment and to have taken fewer days to move in.
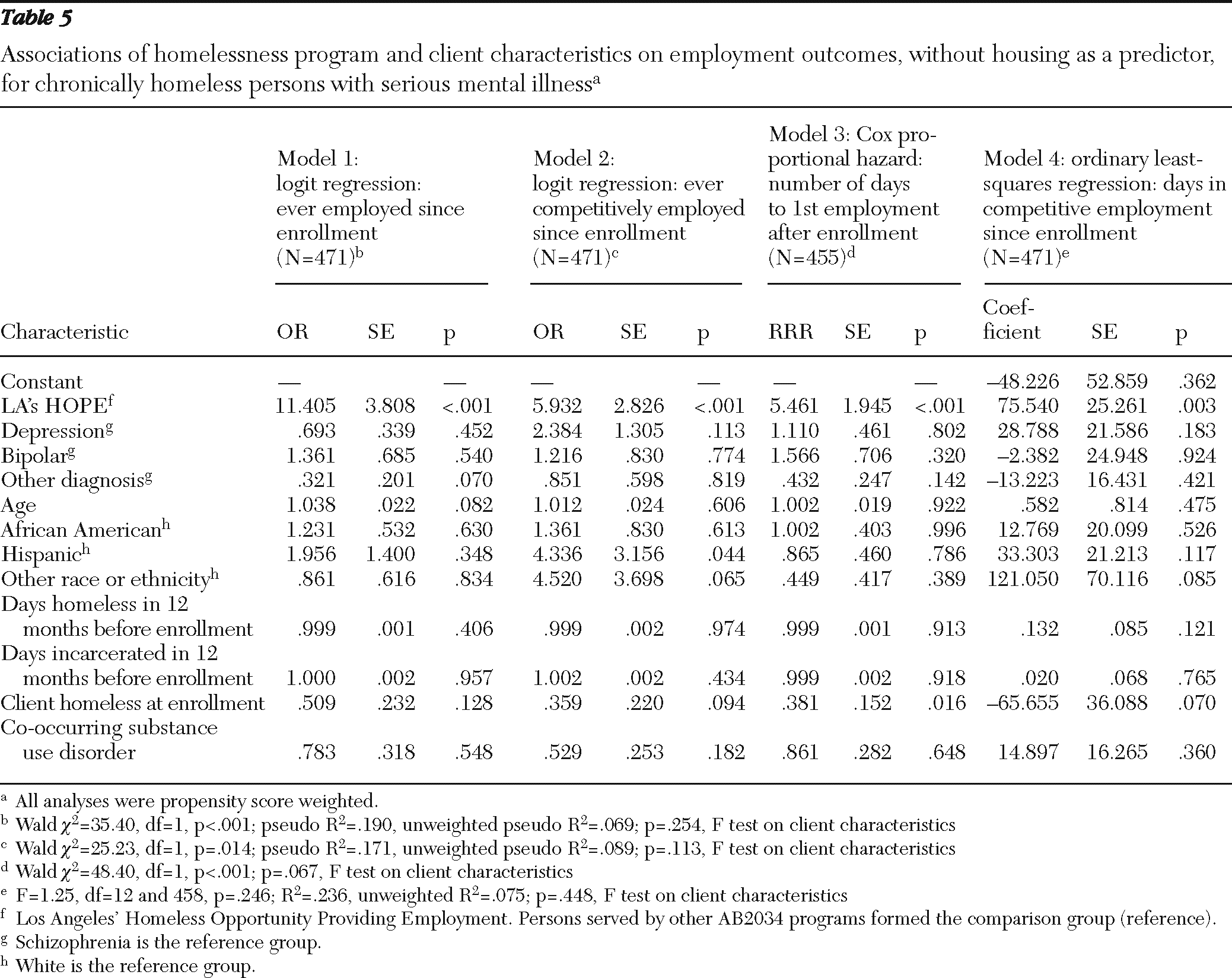
Table 5 shows four employment measures—ever employed and ever competitively employed since enrollment, the number of days that elapsed postenrollment before starting one's first paid employment (if ever), and the average days in competitive employment since enrollment.
The only consistent finding across all four employment variables was that participants in LA's HOPE had better employment outcomes than members of the comparison group. LA's HOPE clients were more than 11 times more likely than comparison group members to have been employed since enrollment (model 1) and six times more likely to have worked in a competitive job (model 2). Further, comparison group members who worked took longer than LA's HOPE clients to find jobs (model 3) and were employed about 48 fewer days (model 4). No client characteristic consistently affected all of the employment outcomes.
The employment models were also run with “ever in supportive housing since enrollment” as a predictor along with individual characteristics to test whether being housed contributed to employment outcomes. Too little is known about how having housing affects various nonhousing outcomes for homeless people. Because this data set contained the relevant variables and the employment-related aspects of LA's HOPE occurred only after clients were housed, it seemed reasonable to conduct an analysis of this issue. Results were mixed. “Ever in supportive housing” increased the variance explained in model 1 (any employment) by 5% and was also a significant predictor in model 3 (time to first employment). For these two models, “ever in supportive housing” split the effect of being in LA's HOPE; both were significant predictors, suggesting that at least half of the effect of LA's HOPE might be attributable to housing stability. The housing variable did not, however, have a significant effect in models 2 (any competitive employment) and 4 (days in competitive employment).
Discussion
LA's HOPE was able to house participants and facilitate their acquisition of jobs and work experience at rates significantly higher than happened for members of the study's comparison group. Firm conclusions from this study are limited by the post facto use of a comparison group rather than random assignment, but demographic, diagnostic, and preenrollment histories of the two groups as well as the use of propensity score matching boost confidence in the results. Further, the comparison group met the three conditions identified in the literature (
21) as providing the best approximation to random assignment—coming essentially from the same population, having baseline assessment of outcome variables to use as predictors, and measuring treatment and comparison groups with the same instrumentation. If anything, compared with the clients of the other AB2034 programs, LA's HOPE clients may have been harder to move toward these outcomes, having experienced more homelessness and marginally greater prevalence of co-occurring substance use problems. Diagnosis was not a significant predictor in any model.
LA's HOPE had the structure and resources to promote these outcomes in greater degree than the programs serving the comparison group. AB2034 programs had resources that could be used for transitional housing situations, but LA's HOPE had permanent rental assistance to offer in the form of Shelter Plus Care certificates. LA's HOPE operated on a “housing first” basis, moving people with active substance abuse issues and mental illnesses uncontrolled by medications into housing and working on those issues once clients were stably housed, in contrast to common practice for many AB2034 programs that clients must be “housing ready”—with stabilized psychiatric symptoms and drug free. LA's HOPE had case managers devoted to engaging clients in employment-related activities and supporting clients' work effort once clients got jobs, using many techniques known to increase the effectiveness of supported employment (
3,
6), whereas other AB2034 programs ran employment support groups but did much less by way of actively promoting work. LA's HOPE had resources it could use to pay for training; classes; work clothing, uniforms, and equipment; and other essentials, none of which were available to other AB2034 programs.
Finally, the demonstration's efforts to coordinate the activities of a city agency, a county agency, a housing authority, and the VA to bring employment, mental health, and housing services to bear ultimately benefited LA's HOPE clients (
6,
24). It is difficult enough, and not always guaranteed, to influence outcomes when one is trying to do so and has resources to help; it is virtually impossible to achieve the same outcomes when one is not focused on them completely. This is the difference observed between LA's HOPE outcomes and those of the comparison group.
Conclusions
LA's HOPE fulfilled its purpose, demonstrating what provision of housing and employment services, offered in a coordinated manner, can mean for people with disabilities who have been homeless a long time. In doing so it adds to the substantial separate literatures on the effectiveness of supported employment and permanent supportive housing by showing what the two can do together. The employment outcomes for LA's HOPE participants versus those of the comparison group supply particularly important new information, and the housing outcomes confirm similar findings found in previous research. Despite the limitations of its quasi-experimental design, this study showed that even AB2034 clients, whose behavioral health impairments and homeless histories are substantial, can participate in work activities and competitive employment to an extent similar to participants in supported employment programs for housed people with mental illness if they are adequately housed and receive carefully targeted assistance to enter the workforce and retain jobs once there. However, in the absence of rental assistance, housing stabilization supports, and employment supports, these outcomes occur far more rarely.
Acknowledgments and disclosures
This research was supported by contract 03-1188-S2 with the Community Development Department of the City of Los Angeles, which in turn operated LA's HOPE under cooperative agreement E9-4-3-0108 from the U.S. Department of Labor Office of Disability Employment.
The author acknowledges the assistance of Jaime Nahman, Los Angeles County Department of Mental Health, for accessing the data used and Monica Davis, Mental Health Association of Greater Los Angeles, for extracting the data from the Caminar data system. Lisa Jordan, Human Solutions, LLC, integrated all of the LA's HOPE case records and ensured that on matters of common content, such as jobs and housing, the case records and Caminar data agreed. Daniel Kuehn, Urban Institute, assisted with integrating data sets and conducting the analyses. The author greatly appreciates the research, logistical, and interpretive support of Susan Quigley, Community Development Department.
The author reports no competing interests.