Stigmatization of people with mental disorders has been called the central issue of mental health (
1). Worldwide, negative attitudes toward persons with a mental illness contribute to housing and employment difficulties, reticence to seek mental health care, limited funding for psychopathology research, shame, and the stress of concealing psychiatric problems (
2,
3).
As neuroscience advances (
4), the biological mechanisms of psychopathology are better understood, and the general public increasingly is exposed to these findings. Advocacy groups like the National Alliance on Mental Illness have embraced this trend (
5), presumably because biological portrayals have been seen as a promising means of limiting the ascription of blame and responsibility to sufferers of mental disorders. Indeed, empirical evidence suggests that describing mental disorders as biologically caused can reduce blame (
6).
Nonetheless, other evidence suggests that biomedical accounts of mental illness are not always effective in reducing expressions of stigmatization other than blame and may exacerbate negative attitudes. For example, biological attributions have been linked to the perception that individuals with mental disorders are dangerous and to laypeople's reluctance to interact with them (so-called social distance) (
7). Moreover, biomedical conceptualizations appear to render mental disorders as “natural kinds”—categories perceived to occur naturally as opposed to those invented by humans—suggesting that they have immutable essences and, therefore, poor prognoses (
8). Given the rising emphasis on biological explanations, strategies to counteract these negative effects are imperative.
In this study, we considered whether providing information about biomedical conceptualizations of psychopathology and about treatment of mental illness contributes to reducing mental illness stigma. We proposed that disseminating information about mental disorders' treatability may challenge the prognostic pessimism linked to biomedical conceptualizations (
9). That is, treatability information would contradict the belief that mental disorders, when biologically caused, are untreatable, lifelong conditions. Thus treatability information would counteract stigmatization of mental illness. In contrast, nonbiological accounts of mental disorders have not been associated with pessimistic prognoses. Therefore, attitudes about persons with mental illness should respond more favorably to treatability information if mental disorders are described as having biological versus nonbiological causes.
In this study, we presented vignettes describing the symptoms of a person with a mental disorder. Each vignette was paired with either a biological or nonbiological causal attribution and presented with or without information describing treatments proven effective for the disorder. Participants who viewed the vignettes were asked to rate how comfortable they would feel interacting with the individuals described in the vignettes by completing a scale measuring social distance. The main hypothesis of the study was that treatment information would be more effective in reducing social distance if paired with biological versus nonbiological attributions of mental illness.
Methods
Participants were 249 individuals recruited through
Amazon.com's Mechanical Turk (mTurk) Web site between December 8, 2010, and December 31, 2010 (
10). Participation was limited to people 18 or older living in the United States. All participants provided informed consent after reading a complete description of the study, which was approved by the Institutional Review Board of Yale University. [Research supporting the use of mTurk for participant recruitment is available online as a data supplement to this report.]
The stimuli were a set of vignettes describing people with mental disorders: Gary, with schizophrenia, and Paula, with borderline personality disorder. To enhance the validity of the information, the vignettes about symptoms, possible causes, and treatments for each disorder were adapted as much as possible from information presented in the Web site of the National Institute of Mental Health (NIMH) (
11).
For each disorder, four experimental conditions and one control condition were created by using different versions of the vignette. The control condition included a description of the symptoms of the disorder and no discussion of its cause or treatability. The four experimental versions included the same symptom description plus a paragraph attributing the disorder to either a biological cause (genes and brain abnormalities) or a nonbiological cause (childhood trauma or negative life events) provided with or without an additional paragraph discussing general medical and psychosocial treatments that have been proven effective for the disorder. To test whether merely mentioning an effective treatment would be sufficient to reduce social distance, unlike previous work that used treatment information to reduce social stigmatization, we did not specify whether the individuals portrayed in the vignettes had received any treatment (
9).
After reading a vignette, the participants were asked to briefly summarize it in writing to ensure that they had thought about its content. The participants' stigmatizing attitudes were assessed by measuring social distance toward Paula and Gary (
12). Social distance was measured on a scale of 1, definitely no, to 7, definitely yes, reflecting the desirability of five types of social interaction with Paula or Gary. The interactions were working closely together on a job, living next door, socializing together for one evening, becoming relatives by marriage, and being friends. These scales were taken from the General Social Survey (
13).
After participants proceeded through the entire task at their own pace, they were presented with optional questions about their demographic characteristics and were fully debriefed about the purposes of the study and the fictitious nature of the vignettes. [The full text of the vignettes used in the study is available from the first author.]
Results
In response to the optional demographic questions, 101 (41%) of the 249 participants identified themselves as female, 62 (25%) identified themselves as male, and 86 (34 %) did not provide a gender. A total of 129 (52%) participants identified themselves as white, 147 (59%) as not Hispanic or Latino, eight (3%) as Hispanic or Latino, five (2%) as American Indian or Alaska Native, 15 (6%) as Asian, 11 (4%) as black or African American, one (.4%) as Native Hawaiian or Pacific Islander, and six (4%) as more than once race (it was possible to select multiple responses). [Further discussion of the participants' demographic characteristics and their relation to other variables is available online as a data supplement to this report.]
Because Cronbach's alpha across the social distance scales was .88, participants' responses for the five scales were averaged together and used as a dependent variable in all subsequent analyses. A 5 (condition) × 2 (disorder) analysis of variance (ANOVA) found no significant interaction (p=.53), so the data from both disorders were collapsed for all subsequent analyses.
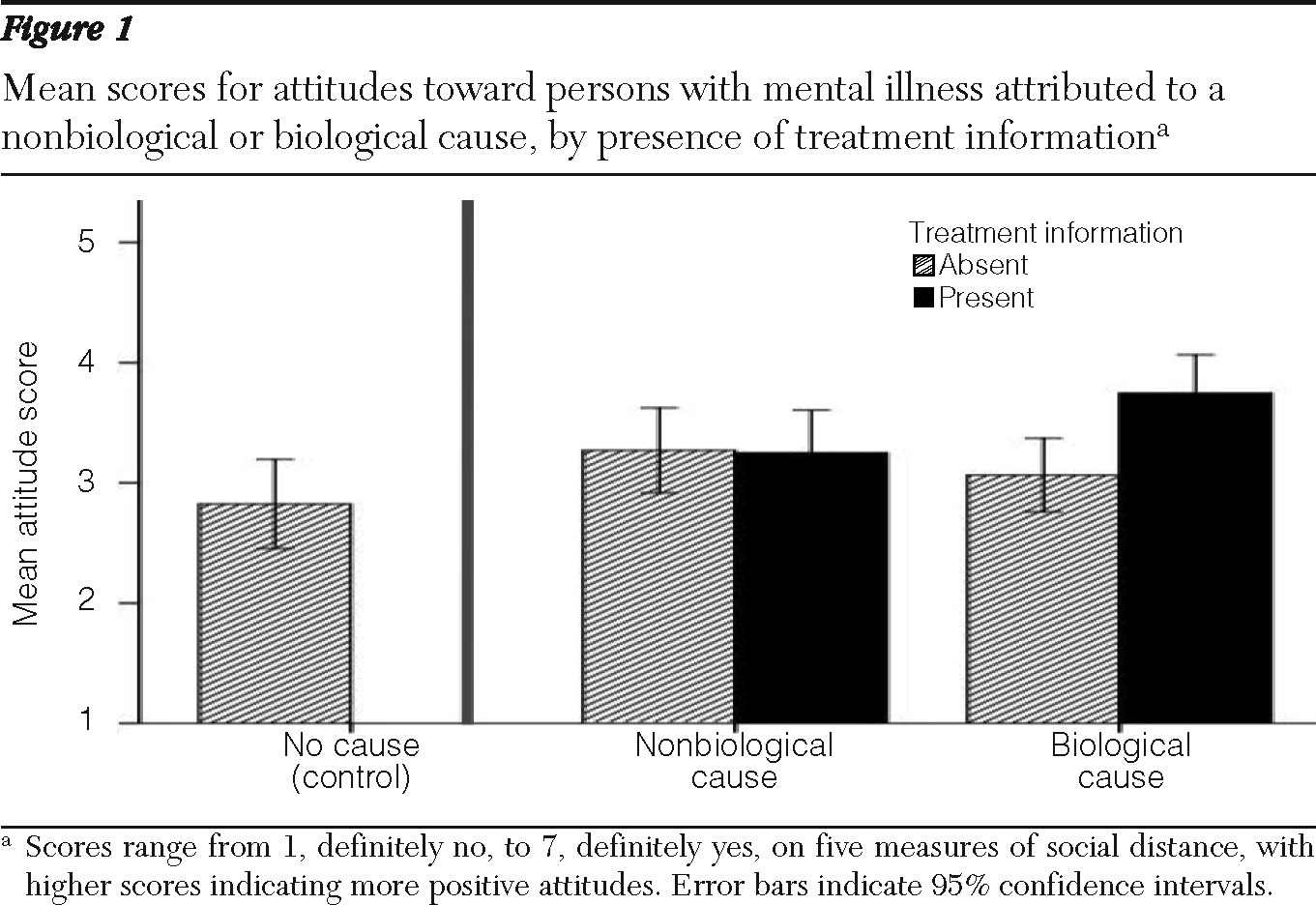
A 2 × 2 ANOVA of biological versus nonbiological causal explanation and presence or absence of treatability information found no significant main effect of causal explanation but found a significant main effect of treatment information (F=3.96, df=1 and 196, p<.05). However, this effect was qualified by a significant interaction effect (F=6.16, df=1 and 196, p=.04) (
Figure 1). Simple effects analyses revealed that mean social distance scores were not affected by whether treatment information was available if the information was paired with nonbiological accounts of mental illness (3.25 versus 3.27, respectively, with and without treatment information). Yet in the context of a biological causal attribution, mean social distance scores were significantly higher (indicating more positive attitudes) when treatment information was provided (3.07 versus 3.75, respectively, with and without treatment information; F=9.61, df=1 and 99, p<.01). This finding supported our prediction that treatment information would have a greater effect on attitudes toward a person with a mental illness if the disorder was attributed to biological causes.
A one-way ANOVA comparing mean social distance scores for the control condition and the four experimental conditions revealed a significant main effect (F=3.95, df=4 and 244, p<.01) (
Figure 1). Simple weighted contrasts comparing each experimental condition with the control condition revealed that availability of treatment information paired with information about a biological cause yielded significantly higher scores (t=3.81, df=244, p<.01). Scores were marginally higher if information about nonbiological causes was provided without treatment information (p=.06) and if information about nonbiological causes was provided with treatment information (p=.08). Scores for the experimental condition involving a biological cause and no treatment information did not differ significantly from scores for the control condition. That is, by itself information about a biological cause failed to reduce social distance.
Discussion
This study explored the effects of information about biological causes of psychopathology provided in conjunction with treatability information. Our main hypothesis was based on previous findings that biological conceptualizations of mental disorders are consistently associated with more pessimistic perceptions of prognosis (
6). As such, we predicted that information about treatment—which can challenge unfavorable prognostic assumptions—would be significantly more helpful in improving attitudes toward individuals with a mental illness if it was paired with a biological versus a nonbiological attribution of illness. Our results supported this hypothesis.
In contrast, providing treatment information failed to produce any additional positive effect on attitudes when the disorder was attributed to a nonbiological cause, possibly because mental disorders that are attributed to nonbiological causes may be assumed to be treatable. Such an assumption would, in a sense, have rendered the pairing of information about treatability and information about nonbiological causation redundant and explain why such a pairing conferred no added benefit.
Replicating previous studies (
7), the study found that providing information about nonbiological causes of mental illness with or without information about treatment produced a positive effect on attitudes about persons with mental illness, presumably because it encouraged laypeople to understand psychiatric symptoms as normal reactions to life events, reducing social distance (
7). Additionally, also replicating previous studies, the study found that information about biological causes alone did not reduce social distance, suggesting that biomedical descriptions cannot be a primary strategy for destigmatizing mental disorders.
Nevertheless, the field of clinical neuroscience has assumed a prominent place in current thinking about psychopathology; the NIMH's research domain criteria proposal is but one important example (
14). Our findings suggest that providing information about treatability may be a promising means of curtailing any negative associations with biological construals, such as those documented in previous studies, that can affect the public's attitudes toward individuals with a mental illness.
Our results also suggest several directions for future research. For example, causal attributions for psychopathology can differentially affect distinct kinds of attitudes, such as pessimism about prognosis or blame for a disorder. We included only a limited set of attitude measures, all of which were related to social distance. We speculate that the results would have been similar if we had measured predictions about prognosis because information about treatability implies better expectations of outcomes. Our findings, however, may not generalize to ascriptions of blame. Whereas biological causality may decrease blame (
6), adding treatment information might seem irrelevant to the question of whether an individual is responsible for his or her problems. Therefore, the interaction effect found in this study would be less likely to occur.
Also, this study was limited to descriptions of individuals with schizophrenia and borderline personality disorder, but other mental disorders may be stigmatized in distinct ways. For instance, among the general public, people with schizophrenia may be more likely than people with depression to be perceived as dangerous (
15). Thus for some types of psychopathology social distance may not be subject to the interaction effect we observed in this study.
Finally, our findings cannot be used to determine whether there is a particular advantage in presenting information about treatment and biological causation together, above and beyond any beneficial effect on attitudes that would be conferred by providing treatment information alone. The answer to this question might depend on whether the disorder being considered is presumed by default to be biologically caused, in which case treatability information could have destigmatizing effects even without the addition of information emphasizing a biological cause.
Conclusions
Stigmatizing attitudes among the public are responsible for a wide array of harms endured by individuals with psychiatric disorders (
2). As such, research that investigates approaches to reducing stigma is important for both its social and clinical implications. As biomedical accounts of psychopathology become increasingly prevalent, it is ever more crucial to understand how to present information about the biological processes involved in mental disorders to minimize stigmatization. Our results suggest that pairing biological explanations of mental disorders with treatment information can diminish negative attitudes toward persons with mental disorders.
Using treatment information may also be more practical than employing causal attributions. The question of what truly causes mental disorders is complicated and murky, and simple answers are difficult to come by (
2). Thus attempts to change attitudes by relying on only one type of causal information may be seen as disingenuous because such attempts may rely on inaccurate or incomplete information. By contrast, information about effective treatments sidesteps this issue and can rely entirely on empirically supported facts.
Acknowledgments and disclosures
This study was supported by grant R01 MH57737 from the National Institute of Mental Health.
The authors report no competing interests.