Persons with serious mental illness suffer from increased rates of comorbidity and die, on average, 25 years earlier than persons in the general population (
1). Such morbidity has prompted searches for remedies, which have focused both on patients' lifestyle (for example, smoking) and clinical practice (for example, physician-directed action). According to one recent study, compared with patients without mental health indications, psychiatric patients are more likely to smoke and be sedentary, and they have a threefold increased incidence of mortality (
2). Even after adjustment for smoking and exercise, a twofold increase in mortality persists, indicating that other factors substantially influence the health of persons with mental illness.
Poor general medical care is an important correlate of morbidity among populations with mental illness (
3). Among Medicare enrollees, use of referral-sensitive surgery, such as insertion of an artificial pacemaker, was lower among persons with mental illness than among those in a control group without mental illness (
4). Beren and others (
5) found that Arizona Medicaid enrollees with mental illness consumed fewer general medical resources, in 1999 dollars, than those in a control group ($1,431 versus $1,750), despite higher rates of emergency department use. Moreover, delayed care was reflected in the result that urgent care for enrollees with a mental illness often correlated with the treatment of genitourinary disease, whereas enrollees without a mental illness typically received such care in outpatient office settings. Likewise, data from California and Nevada revealed that veterans with a mental illness—even those with conditions warranting ongoing medical attention, such as diabetes and hypertension—used fewer somatic care services than others (
6). In yet another example, a national study of over 80,000 Medicare patients demonstrated that myocardial infarction care for persons with mental disorders was below standard (
7).
Such morbidity and mortality statistics renew attention to somatic care for persons with mental illness. The National Council for Community Behavioral Healthcare (NCCBH), representing nonprofit U.S. treatment centers, strongly advocates holistic care through greater integration of mental health and other medical domains (
8). Somatic care needs of persons with mental illness are relevant to the popular notion of “person-centered” care (
9). Two components of the patient-centered care model advocated by NCCBH are the subject of this study: preventive services and women's health.
Women with mental illness have unique health care needs that extend beyond brain and behavioral pathology. Compared with men with mental illness, women with mental illness generally have more reproductive health concerns secondary to sexual abuse and their biology (
10–
14), and they typically experience lower income and age-adjusted physical functioning (
15).
Methods exist for early detection of cervical and breast cancers, diseases that can be deadly to women (
16), but these screens are used less frequently by women with mental illness than by others. In a study of 109,240 Canadian women, Chochinov and others (
17) found that after adjustment for age, region, continuity of care, and comorbid conditions, mammography use among women who had been diagnosed as having schizophrenia (N=1,448) was reduced by 36% compared with use among women in a control group. This finding replicated a private insurance-based study in the United States that demonstrated that mammography among women with mental illness decreased as severity of mood, anxiety, psychotic, and substance abuse disorders increased (
18).
Reduced cervical cancer screening among women with mental illness has also been observed. Martens and others (
19) reviewed records of 338,514 Canadian women; after adjustment for demographic characteristics, including income, they found a 30% decrease in Pap screening rates among women with schizophrenia. This finding was replicated in a random, clinical sample of 169 women with or without mental illness (
20). Substance use disorders are frequently comorbid with other mental illnesses and are known to increase risk of somatic diseases and inhibit preventive screening (
14,
21–
23).
This report reviewed cervical cancer screening rates for women with and without mental illness who participated in Maryland's Medicaid program. Reviewing Medicaid is important because the program covers disproportionate numbers of women of childbearing age and persons with mental illness (
24,
25).
Methods
Data
This report is based on administrative records for all females (N=494,025) who were enrolled in Maryland's Medicaid program in fiscal year 2005 (July 2004–June 2005). Only the subset of women who had 12 months of enrollment (N=325,338), were aged 19 to 64 years (N=129,013), had no pregnancies during the study year (N=107,302), and had benefits that included preventive screening were included in the final sample (N=105,681). Undocumented aliens, for example, receive emergency medical assistance with a federal match but do not qualify for preventive services.
Outcomes
The main outcome measure was the presence or absence of cervical cancer screening. A secondary outcome was acute primary and specialty care visits, where cervical cancer screening is likely to occur or be advocated (
26–
28). A tertiary outcome was any genital cancer, viewed cautiously because such cancers are rare and tied to special Medicaid eligibility. Outcomes were identified from diagnostic or procedure codes from individual Medicaid records corresponding to all inpatient, outpatient, home health, long-term care, and all other nonpharmacy medical transactions. Evaluation and management or gynecological examination codes were used as indicators of acute primary and specialty care visits. Code lists (available upon request) were checked against published HEDIS criteria (
29) and Ingenix EncoderPro (Salt Lake City, Utah) to optimize face validity.
Main predictors
Variables of interest were any Medicaid claim with a diagnosis of psychosis (schizophrenia and related disorders); substance use disorder, excluding tobacco only; bipolar disorder or mania in the absence of psychosis or substance use; depression absent the other three diagnoses; and all others (control group). Although similar categories were utilized previously (
30), for this study we further separated bipolar disorder or mania cases from cases of unipolar depression only to increase diagnostic specificity. Diagnostic assignment for each individual corresponds to the presence of one or more Medicaid claims (thereby affording high sensitivity to disease) for psychosis (
ICD-9 codes 295 and 297), substance use disorders (303–305, except tobacco), bipolar disorder or mania (296, except depression), and unipolar depression (296.2–296.3, 311). Substance use with or without psychosis was separately identified for each individual because psychosis was of principal interest, and a substantial percentage of individuals with psychosis have a comorbid substance use problem (
22,
30).
Although we chose to focus on psychosis while making adjustments for substance use, it is notable that we also included diagnostic markers for other severe types of affective disorders, for example, bipolar disorder, mania, and major depressive disorders. Previous studies of preventive care among patients with mental illness have similarly focused on psychotic patients (
17–
20), although some studies have also considered the impact of other types of mental illness (
17,
20,
31).
Demographic covariates
Our modeling included age, because recommendations for cervical cancer screening vary for women of different ages (
32); race (white, black, or other), to account for possible racial disparities (
33); and region, to account for differences suggested by other research between the state's urban (Baltimore and Washington, D.C., suburbs and Baltimore City) and rural (Western Maryland, Southern Maryland, and the Eastern Shore) areas (
28).
Disease covariates
Infectious diseases variables were constructed for the presence or absence of sexually transmitted diseases (STDs), including HIV-AIDS and human papilloma virus (HPV). These diseases correlate with increased risk for cervical cancer (
32). The STD category captured candidiasis, chlamydia, gonorrhea, syphilis, and hepatitis B and C (codes available upon request).
Statistical methods
Logistic regressions were used to consider the effects of psychiatric diagnosis on the odds of cervical cancer screening, acute care visits, or cancer. For the cancer-screening analysis, women with a history of genital cancer or hysterectomy were excluded, and HPV status was included in the regression as a separate covariate. Cancer or hysterectomy cases were removed to focus on primary cervical cancer prevention (
32). All genital cancers (cervical, uterine, ovarian, and vaginal) were combined because of their low prevalence, because oncological processes in these organs may be related, and because screening decisions are influenced by personal history (
34). These indicators removed or flagged only a small portion (1.7%, N=1,797) of the entire population (N=298, HPV; N=634, cancer; and N=1,007, hysterectomy).
Separate regressions were modeled with the three outcomes (screening, acute care visit, or cancer) by using the general form:
Ln (odds of outcome) = b0 + b1
× psychosis + b2 × substance use
+ b3 × bipolar disorder or mania
+ b5 × control + b6 × age
+ b7 × age2 + b8 × race + b9
+ b10 × geography + b11 × STD
The betas are regression coefficients, representing either the intercept term (b
0) or slope coefficients (b
1–b
12) for each parameter. Variables were binary, reflecting presence or absence, except for Medicaid eligibility (six categories), region (six categories), years of age (continuous units converted to ten-year increments), and race (three categories). Medicaid eligibility was a proxy for overall morbidity and benefits covered (
35–
37).
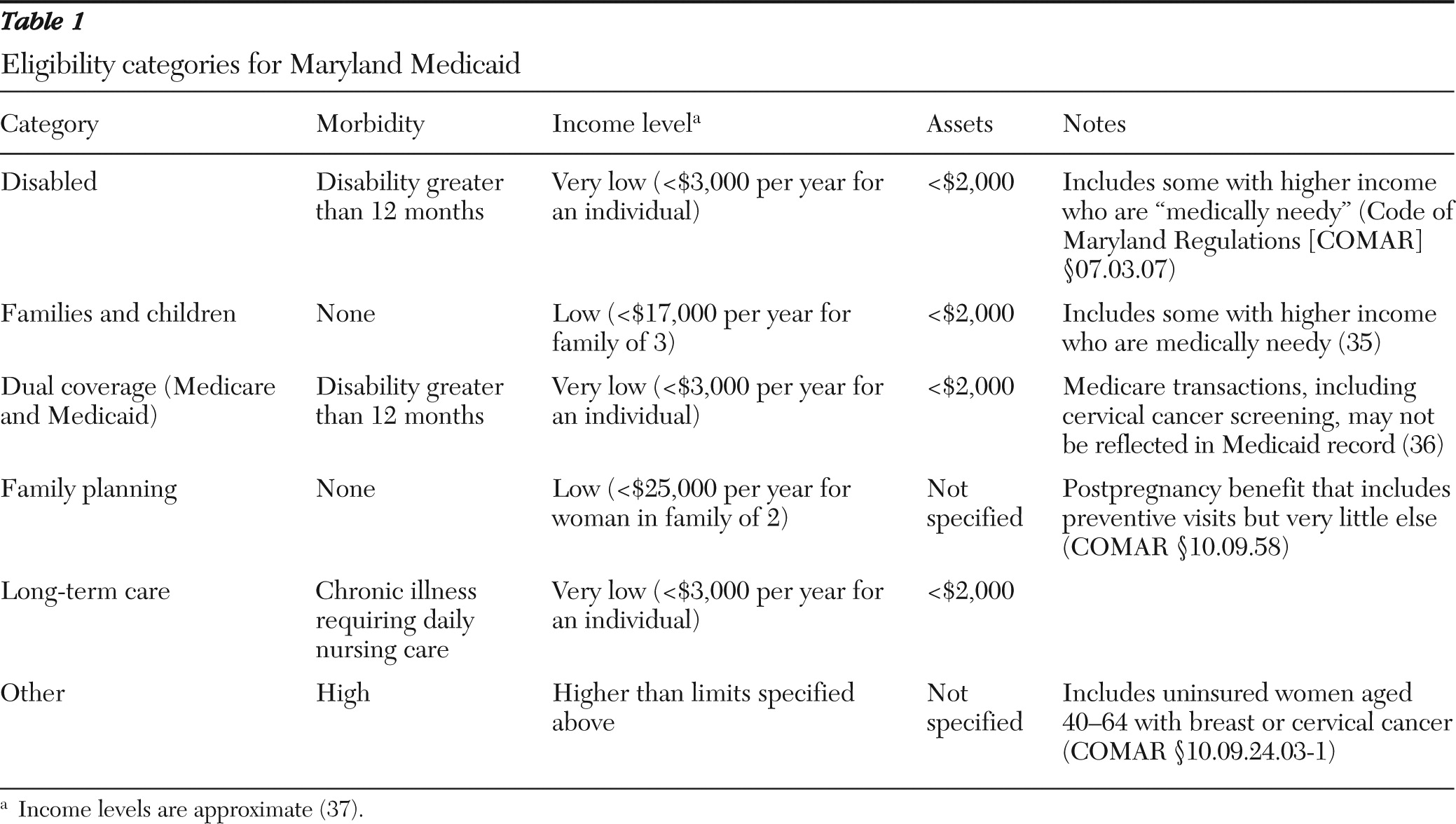
Table 1 lists Maryland Medicaid's eligibility criteria for categories of care.
Alternative specifications were used to consider the impact of comorbid psychosis and substance use on the odds of each outcome (
30). One specification used an interaction term between psychosis and substance use disorder, and another used six hierarchical mutually exclusive dummy variable diagnostic categories. These alternative specifications contrasted slightly with the main model's hierarchical and potentially overlapping categories of psychosis, substance use disorder, bipolar disorder or mania, depression, and control. Sensitivity analyses removed persons whose symptoms were coded as remitted (N=56) for each diagnosis by using the
ICD-9 fifth digit and persons with other mental disorders (
ICD-9 codes 290–317) (N=2,217) from the control groups. Sensitivity analyses also removed those with limited coverage (only family planning benefits, N=40,581), or with insurance by Medicare (N=14,858) because their full medical utilization was not visible in Medicaid records (
36).
Finally, the main screening regression was rerun with acute care visits as an added predictor, and separate chi square analyses were used to quantify the effect of such visits on rates of cancer screening. The appended regression tested directly whether differences in cancer rates among groups of patients remained after adjustment for the expected effects of continuity of care (
19,
20).
Analyses were conducted with SAS, version 9.2. Two-tailed p values <.05 were considered significant. Model fits were assessed with Hosmer and Lemeshow chi square tests, receiver operator curves (ROC), and the SAS max-rescaled R
2. This latter statistic is an “R
2-like” indicator for logistic regression in the sense that it reflects the fraction of the variance of the dependent variable that is explained by the model (
38).
An institutional review board (IRB) waiver was obtained from Maryland's Department of Health and Mental Hygiene to permit use of these Medicaid administrative data. Additional IRB approval was received from the National Institute on Drug Abuse, which funded the study. To protect the confidentiality of the sample, all reporting censored cells of fewer than 12 persons.
Results
Unadjusted statistics
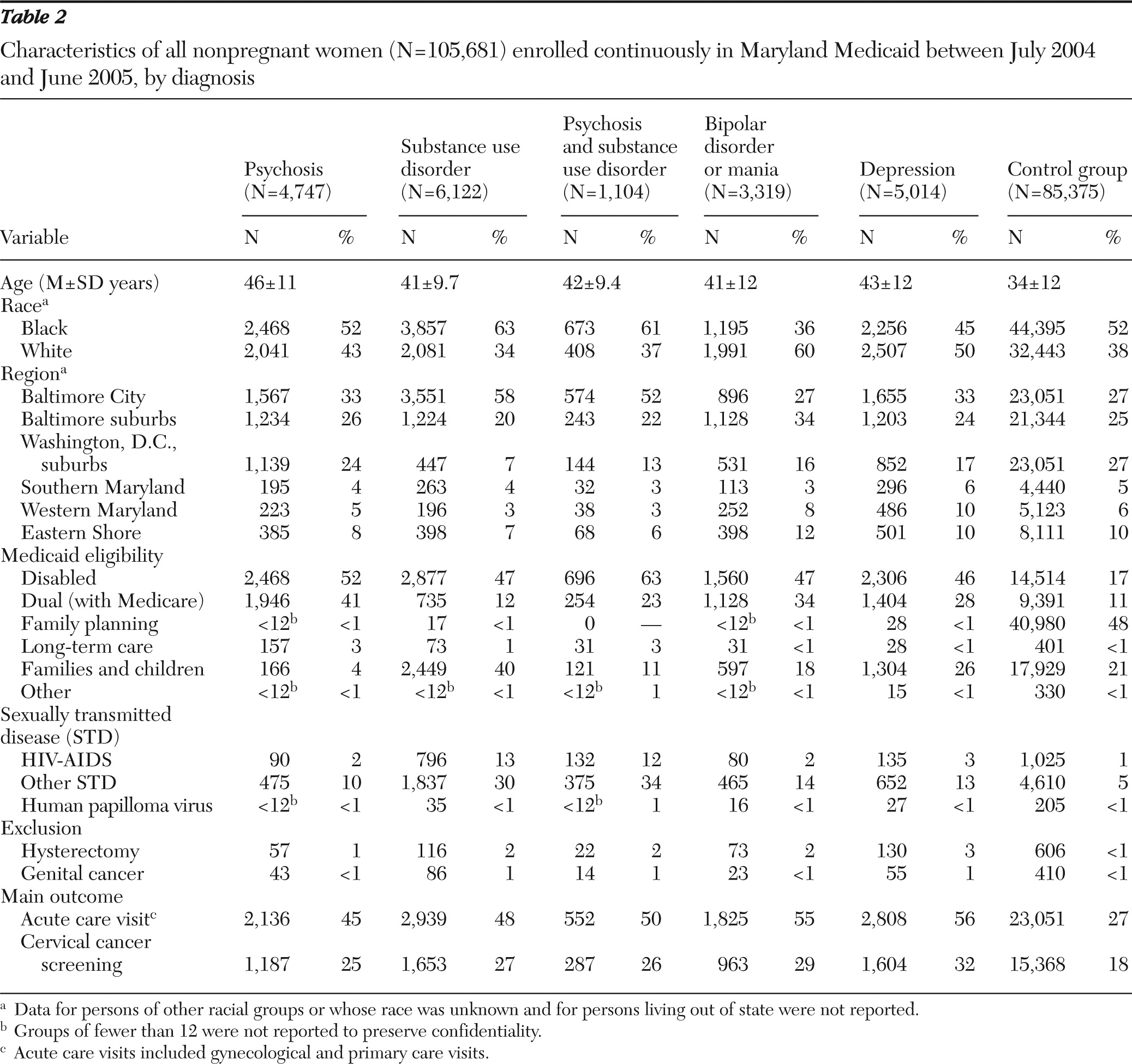
Table 2 offers summary statistics for the 105,681 enrollees stratified by diagnostic group. Use of cancer screening and acute care services was greater among enrollees with psychosis (25% and 45%, respectively), bipolar disorder or mania (29% and 55%), and depression (32% and 56%) than in the control group (18% and 27%). The prevalence of cancer was lower among those in the control group (<.5%) than among any diagnostic group (range <1%–1.4%).
Logistic regression
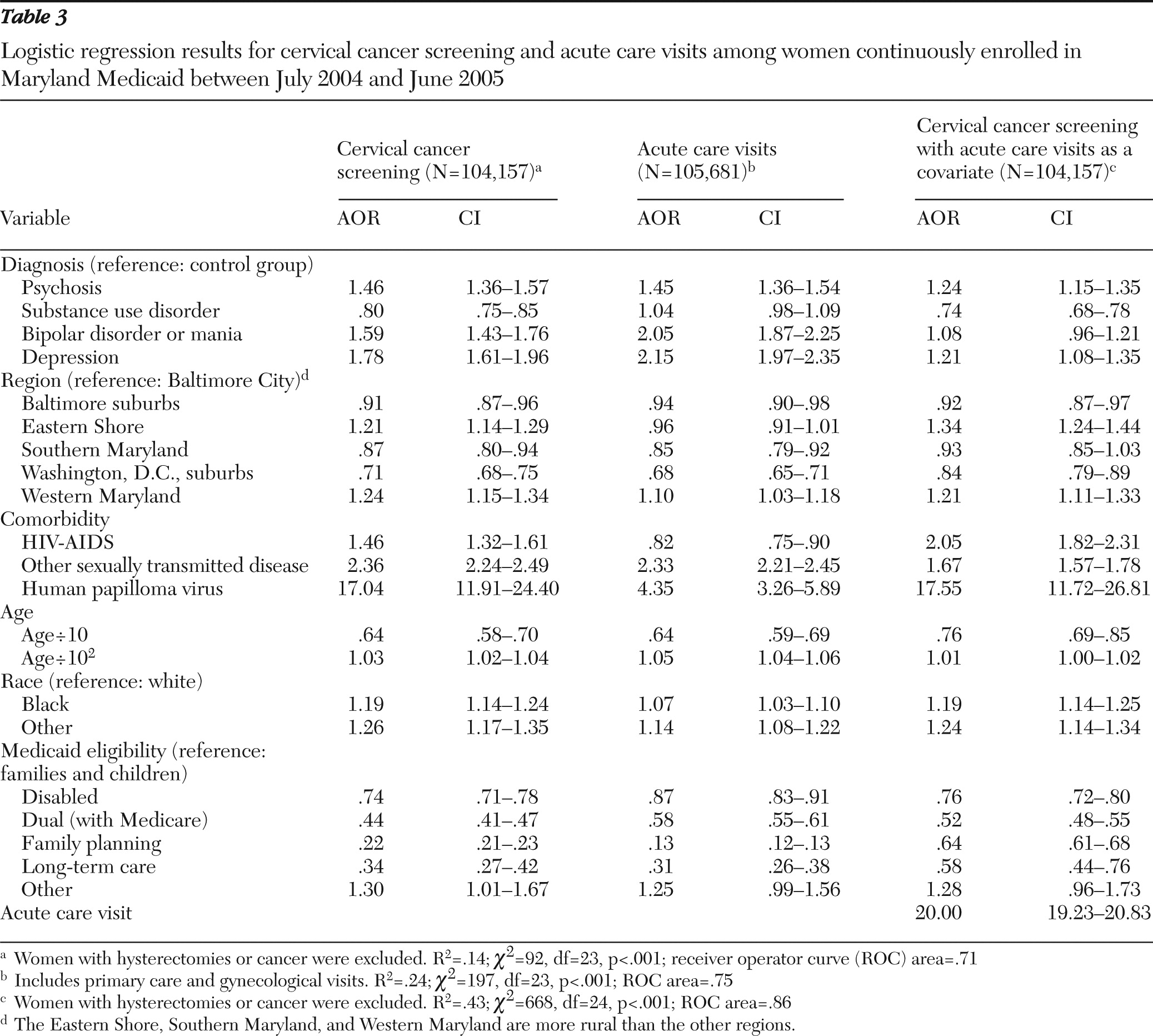
Table 3 presents logistic regression results for the three main models. Unless noted otherwise, the adjusted odds ratios (AORs) are based on contrasts with a reference group for each parameter category.
Cervical cancer screening.
The model with cancer screening as the dependent variable predicted 14% of the variance in that outcome (
Table 3). Compared with odds of screening among enrollees in the control group, the odds of screening were increased for all the diagnostic groups, with the exception of substance use disorder (psychosis, AOR=1.46; bipolar disorder or mania, AOR= 1.59; and depression, AOR=1.78). The substance use disorder group showed decreased odds of screening (AOR=.80).
Alternative-specification results were similar (data not shown). The interaction of psychosis and substance use disorder yielded a nonsignificant effect (AOR=.98, confidence interval [CI]=.74−1.28). The analyses using the six nonoverlapping diagnostic categories confirmed that the odds of screening were reduced among persons with a substance use disorder compared with persons in the control group (AOR=.81; CI=.75−.86). The odds of screening were increased among persons with psychosis compared with persons in the control group (AOR=1.49, CI=1.38−1.60), but the odds of screening among persons with psychosis and a substance use disorder and among persons in the control group did not differ (AOR=.95, CI=.82−1.1).
Sensitivity analyses of the screening findings validated our main models (data not shown). Specifically, after removing persons in remission, persons with limited Medicaid coverage, and persons in the control group with other mental illnesses (not otherwise considered in our analysis), we found that the cancer screening results were similar (N=42,680, χ2=18.1, df=21, p=.020. Screening rates were reduced for persons with a substance use disorder (AOR=.78, CI=.73–.84) and significantly elevated for persons in the other mental illness groups (AOR range 1.43–1.80).
Acute care visits.
The model with acute care (primary or gynecological) visits as the dependent variable predicted 24% of the variance surrounding that outcome (
Table 3). The adjusted odds of such visits were significantly increased for persons with psychosis (AOR=1.45), bipolar disorder or mania (AOR=2.05), or depression (AOR=2.15) versus the control group (
Table 3). The adjusted odds of such visits for persons with a substance use disorder and persons in the control group, however, were not distinct (AOR=1.04). The analyses of the mutually exclusive groupings yielded similar results and demonstrated that the odds of having an acute care visit among persons with psychosis and a substance use disorder (AOR=1.26; CI=1.12−1.43) were between the odds for each diagnostic group alone. Somewhat consistent with this intermediate result, the interaction model showed that the odds of acute care visits among persons with psychosis and a substance use disorder were increased compared with persons in the control group and that the difference approached significance (AOR=1.23; CI=.96−1.57, p<.10).
Removing persons in remission, persons with limited Medicaid benefits, and persons in the control group with other mental disorders showed similar results (N=42,680, χ2=40.4, df=21, p<.001); compared with persons in the control group, persons with substance use were 1.03 times more likely to have an acute care visit (CI=.97–.1.09), and persons in the other mental illness diagnostic groups had increased odds of having an acute care visit (AOR range 1.46–2.26).
Cancer.
None of the statistical modeling to predict genital cancers was significant (data not shown). This included all specifications and sensitivity analyses.
Covariate effects.
Table 3 presents all covariate effects of the main models. Regional effects were similar across all specifications. Compared with odds for enrollees in Baltimore City, the odds of cervical cancer screening and acute care visits were significantly decreased among enrollees in the Baltimore and Washington, D.C., suburbs and Southern Maryland and significantly increased among enrollees in Western Maryland. The enrollees on the Eastern Shore demonstrated significantly increased AORs only for cancer screening.
Comorbidities were significant covariates for both outcomes, as expected. The only unexpected result was that HIV-AIDS correlated with decreased adjusted odds for acute care visits. Estimates were extremely high for the HPV effect (AOR=17.04 and 4.35, respectively, for cancer screening and acute care).
All age and race effects were similar across models. Blacks and other nonwhites had slightly increased odds of cancer screening and acute care visits. The negative linear effect of age was offset by a positive squared effect reflecting increased odds with increasing age (
Table 3).
Cancer screening and acute care visits were similar in magnitude and direction for all Medicaid eligibility correlates except family planning; after adjustment for acute care visits, enrollees who were eligible only for family planning benefits showed higher cancer screening rates, but the rates were still well below those of the comparison group of enrollees with Medicaid eligibility for families and children. The odds of cancer screening and acute care visits were decreased among all groups compared with enrollees in the families and children eligibility category, with the exception of the small, heterogeneous, high-morbidity, “other” grouping.
Effects of acute care visits.
Table 3 shows that acute care visits were correlated with a large increase in screening odds (AOR=20). After adjustment for acute care visits, the odds of screening among the substance use disorder group and the members of the control group remained similar, but the odds of screening among the other diagnostic groups were attenuated. For example, the odds of cancer screening among persons with a bipolar disorder or mania and among persons in the control group were statistically indistinguishable (AOR=1.08).
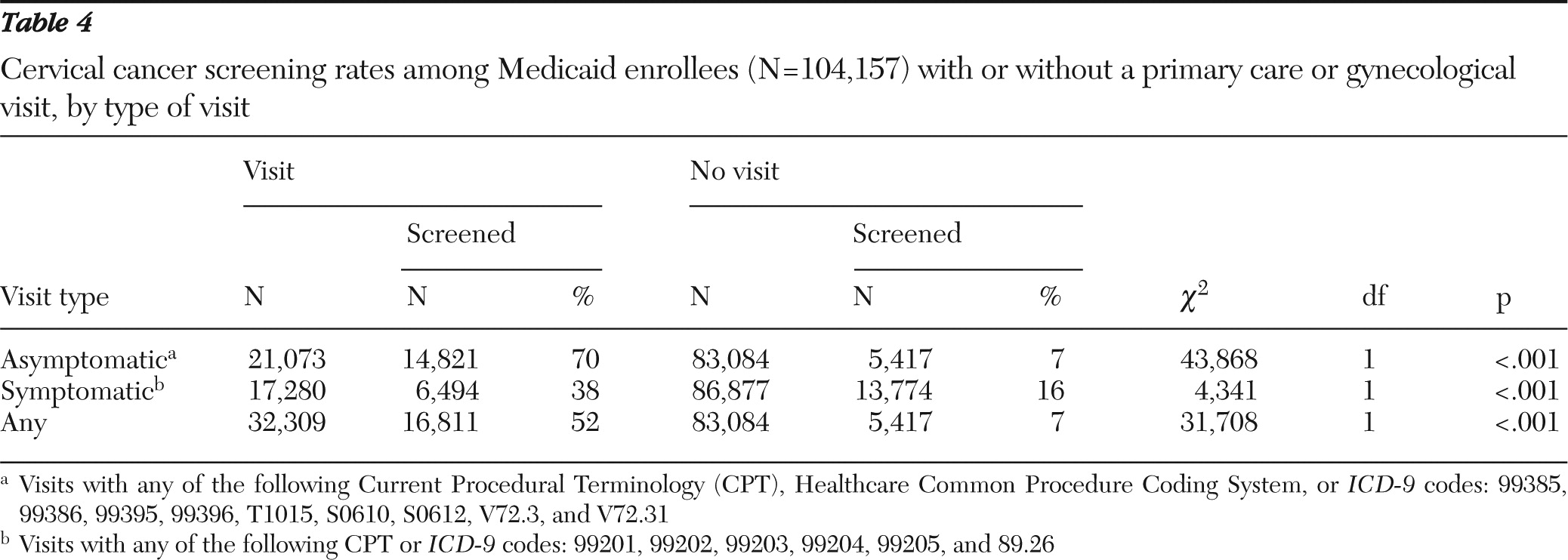
Table 4 shows that all acute care visits, especially asymptomatic visits, correlated strongly with cancer screens in the same year.
Discussion
Main effects
Among women with continuous enrollment in Maryland Medicaid, those with a diagnosis of psychosis, bipolar disorder or mania, or depression had increased adjusted odds of cervical cancer screening and associated acute care visits compared with enrollees in the control group. By contrast, women with substance use disorders had decreased odds of cancer screening and equal odds of acute care visits compared with enrollees in the control group. These results were consistent across alternative statistical specifications, including analyses that modeled interactions between substance use disorder and psychosis, removed persons with remission ICD codes, and removed persons with limited Medicaid coverage or other mental illnesses.
These findings contradicted much previous work showing that persons with mental illness, especially those with a comorbid illness, experience barriers to preventive and other medical services (
3,
17,
18,
20,
22,
39–
41). We believe that two factors explain our novel results—our inclusion of specific substance use indicators and our focus on Maryland Medicaid.
Other researchers have observed that groups with various mental disorders have different rates of preventive screening (
42), and one meta-analysis concluded that substance use disorders are tied more consistently than other forms of mental illness to somatic care disparities (
39). In addition, key studies have ignored substance use disorder as a comorbidity or conflated it with other mental illnesses (
17–
20). Accordingly, we removed the substance use disorder flag from our regressions to test whether the effects of the other diagnoses would change from positive to negative. They did not, thus failing to confirm our hypothesis that exclusion of substance use disorder flags exerted a negative bias on estimates of odds of preventive screening among persons with non-substance use mental disorders.
As such, we are left with the explanation that compared with women in the control group, women enrolled in Maryland Medicaid who had a serious mental illness (except a substance use disorder) experienced relatively higher rates of preventive screening than women with similar diagnoses living in other places or enrolled in other systems. Two studies from Canada found markedly lower rates of mammography (
17) and cervical cancer (
19) screening among women with psychosis. A third Canadian study also found markedly reduced rates of screening among women with psychosis compared with women without psychosis (
20). These studies were similar in design to ours, but because of their location and the nature of the system of universal coverage under study, they included persons across the income and wealth spectrum. Accordingly, our results may differ because we focused on low-income adults in Maryland. Income effects in Iowa, for example, may explain why research there observed reduced rates of mammography in a private insurance sample (
18).
The findings that having a substance use disorder was a key factor inhibiting preventive care were analogous to findings observed earlier about osteoporosis screening among an older subset of the same cohort (
30). However, all these effects, unexpectedly, seemed to be offset by the presence of psychosis. Such an offset is consistent with the theory that the use of any services encourages use of preventive services (
43).
The discrepancy in cancer screening among persons with a substance use disorder, combined with the strong correlation between acute care visits and screening, points to an obvious remedy: women with a substance use disorder should be encouraged to visit primary care physicians or gynecologists (
27). Moreover, including acute care visits as a predictor of cancer screening showed that such visits were a dominant correlate. At the same time, however, this additional modeling revealed that even after adjustment for acute care visits, persons with substance use disorders had decreased odds of cancer screening, suggesting that factors other than visit access are at play.
Covariate effects
Geographic effects for the two main outcomes were apparent, but there was no consistent urban or rural divide (
28).
All STDs had the anticipated impact of increasing cancer screening with or without the use of acute care visits as a covariate (
32). Surprisingly, however, HIV-AIDS correlated with decreased odds of acute care visits, indicating that general preventive care may be inhibited for persons with this chronic disease (
44).
Racial effects favored blacks and other groups over whites with regard to utilization of acute care and cancer screening. This was an unexpected result given documented disparities in health care (
33).
Medicaid eligibility by disability or family planning correlated with marked reductions in screening and acute care visits. The disability effect may be related to the system's capacity to provide preventive services to those with competing chronic illness. The correlate with family planning eligibility is likely related to limits in medical coverage or personal tendencies to seek preventive care. These results are consistent with the notion that extremes of the health spectrum (high or low morbidity) correlate with low utilization of preventive services.
Limitations
This work was specific to Maryland, a wealthy state that has achieved relatively high grades for its public mental health system (
45). It relied on cross-sectional, annual prevalence data that may cause events to be undertallied and for which the treatment events may not follow in time from the diagnoses assigned. Moreover, the study did not adjust for severity within diagnosis (
18), and it excluded partial-year enrollees (
46).
Conclusions
Our analyses suggest that women with psychosis and other serious mental disorders who were enrolled in Maryland Medicaid were more likely than persons in the control group to receive cervical cancer screening and related (primary or gynecological) acute care visits. Women with only a substance use disorder, however, appeared to be at increased risk of missing cancer screenings but not acute care visits. Routine visits were an especially strong predictor of cancer screening, and thus supporting use of acute care visits is a high-potential path toward better prevention.
Acknowledgments and disclosures
This study was supported by the Intramural Research Program, National Institute on Drug Abuse (NIDA), and NIDA Residential Research Support Services Contract HHSN271200599091CADB. The authors thank Nancy Svehla, R.N., C.P.H.Q., for her early work on their clinical definitions.
Mr. Abrams and Dr. Boddie-Willis receive substantial financial support from Maryland's Department of Health and Mental Hygiene. Dr. McMahon has served as a consultant for Amgen, Inc. Dr. Kelly receives grant support from Bristol-Myers Squibb and Janssen Pharmaceutical. The other authors report no competing interests.