Patient-Centered Mental Health Care for Female Veterans
Abstract
Objective:
Methods:
Results:
Conclusions:
Methods
Recruitment and Sample
Measures
Data Analysis
Results
| Variable | N | % |
|---|---|---|
| Age group | ||
| 18–44 | 135 | 28 |
| 45–64 | 295 | 61 |
| ≥65 | 54 | 12 |
| Racea | ||
| Caucasian | 308 | 64 |
| African American | 114 | 24 |
| Asian or other | 59 | 12 |
| Hispanic ethnicitya | 49 | 10 |
| Education | ||
| Grade 12 or GED | 38 | 8 |
| College 1–3 years | 267 | 55 |
| College ≥4 years | 108 | 22 |
| Graduate or professional school | 71 | 15 |
| Marital statusa | ||
| Married or unmarried couple | 186 | 38 |
| Divorced, separated, or widowed | 211 | 44 |
| Never married | 86 | 18 |
| Sexual orientationa | ||
| Heterosexual | 458 | 89 |
| LGB/not sureb | 51 | 11 |
| Children in the home | 103 | 21 |
| Employmenta | ||
| Employed | 187 | 39 |
| Unemployed | 47 | 8 |
| Out of labor force | 120 | 25 |
| Disabled | 127 | 26 |
| Military brancha | ||
| Army | 233 | 48 |
| Navy | 105 | 22 |
| Air Force | 94 | 19 |
| Marines | 30 | 6 |
| Coast Guard, National Guard | 16 | 3 |
| Service era | ||
| Pre-Vietnam war | 35 | 7 |
| Vietnam war | 124 | 26 |
| Post-Vietnam war | 221 | 46 |
| Persian Gulf war | 238 | 49 |
| OEF/OIF/OND servicec | 86 | 18 |
| Past-year psychiatric diagnosis | ||
| No | 202 | 42 |
| 1 diagnosis | 120 | 25 |
| >1 diagnosis (comorbidity) | 162 | 33 |
| Past-year mental health visit | 259 | 54 |
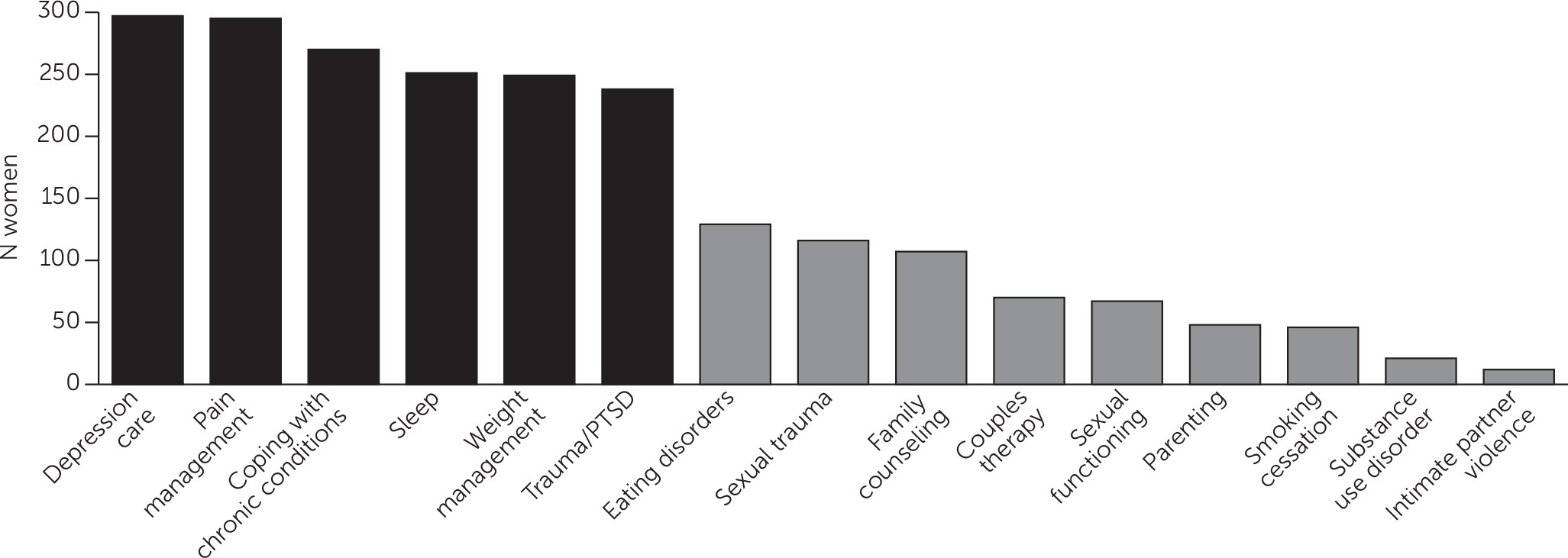
| Depression care (N=298) | Pain management (N=296) | Coping with chronic medical conditions (N=271) | Sleep (N=252) | Weight management (N=249) | Traumatic stress or PTSD (N=239) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI |
| Black (reference: white) | 2.64 | 1.50–4.62 | 2.09 | 1.23–3.57 | 1.09 | .62–1.90 | 2.33 | 1.30–4.20 | 1.16 | .62–2.16 | 2.28 | 1.17–4.47 |
| Asian or other (reference: white) | .86 | .37–1.99 | 1.18 | .51–2.77 | 1.37 | .59–3.19 | 4.17 | 1.67–10.44 | 1.16 | .51–2.68 | 1.32 | .60–2.90 |
| Hispanic ethnicity (reference: not Hispanic) | .48 | .20–1.11 | .59 | .22–1.57 | 1.09 | .41–2.87 | 4.04 | 1.33–12.34 | 1.19 | .51–2.80 | 1.39 | .61–3.17 |
| Lesbian, gay, or bisexual (reference: heterosexual) | 1.81 | .92–3.55 | 2.41 | 1.12–5.17 | 1.29 | .60–2.76 | 1.39 | .67–2.90 | 1.67 | .75–3.70 | 3.00 | 1.33–6.77 |
| Age 45–64 (reference: 18–44) | .94 | .54–1.62 | 1.41 | .80–2.46 | .96 | .54–1.70 | 2.43 | 1.27–4.64 | 2.39 | 1.21–4.73 | 1.10 | .60–2.02 |
| Age ≥65 (reference: 18–44) | .52 | .22–1.23 | 1.48 | .63–3.48 | .81 | .34–1.88 | 1.29 | .48–3.50 | 1.09 | .43–2.79 | .81 | .28–2.35 |
| Tele–mental health acceptable (reference: no) | 1.11 | .69–1.79 | 1.49 | .92–2.40 | .91 | .56–1.48 | 1.15 | .66–2.01 | .66 | .37–1.17 | 1.18 | .69–1.99 |
| Primary care colocation important (reference: no) | 5.08 | 3.19–8.10 | 5.16 | 3.21–8.31 | 6.40 | 3.75–10.92 | 4.80 | 2.84–8.11 | 5.28 | 3.15–8.85 | 4.94 | 2.83–8.63 |
| Positive PTSD screen (reference: no) | 1.90 | 1.17–3.09 | 1.37 | .82–2.31 | 1.88 | 1.06–3.34 | 2.64 | 1.49–4.67 | 1.06 | .60–1.89 | — | — |
| Military sexual trauma (reference: no) | 1.13 | .69–1.85 | .88 | .53–1.46 | .95 | .57–1.56 | 1.18 | .69–2.03 | 1.11 | .66–1.87 | 1.99 | 1.14–3.49 |
| OEF/OIF/OND deployment (reference: no)b | .67 | .36–1.22 | .69 | .35–1.37 | 1.00 | .51–1.96 | .84 | .40–1.74 | .73 | .34–1.55 | .51 | .27–.98 |
| Any mental disorder (reference: no diagnosis) | 1.20 | .67–2.14 | 1.62 | .94–2.81 | 1.39 | .77–2.51 | .66 | .35–1.23 | .88 | .49–1.58 | 1.70 | .87–3.30 |
| Psychiatric comorbidity (reference: no diagnosis) | 1.25 | .71–2.21 | 2.06 | 1.13–3.76 | 1.21 | .66–2.25 | 1.10 | .58–2.09 | 1.38 | .75–2.54 | 2.18 | 1.17–4.06 |
Discussion
Conclusions
Acknowledgments
References
Information & Authors
Information
Published In
Cover: Snowbound, by John Henry Twachtman, ca 1889. Oil on canvas; 64 × 77 cm. Art Institute, Chicago. © DeA Picture Library, Art Resource, New York City.
History
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).