The prevalence of impulse dysregulation and mental illness is high in correctional systems, with estimated rates of symptoms as high as 50% among U.S. detainees (
1–
3). In Connecticut, more than two in three newly incarcerated inmates meet criteria for at least one lifetime psychiatric illness (
3). Emotional instability and episodes of aggression by inmates raise safety and adjustment concerns, including population management issues and increased recidivism risk (
4). Personality, psychotic, and substance use disorders are prevalent among prisoners (
5); these disorders are often linked to impulsivity and institutional violence (
6–
10). The presence of co-occurring mental and substance use disorders has been linked to future violence (
11). In addition, many inmates who may not meet criteria for a psychiatric disorder may nevertheless lack adequate impulse and affect regulation and interpersonal skills requisite for adequate functioning, either in the community or in a correctional environment (
4). This suggests that efforts designed to improve behavioral outcomes may need to include inmates irrespective of diagnosis or perceived need for mental health treatment. Evidence-based mental health treatments targeting the specific needs of incarcerated populations are currently very limited (
12), and alternatives to current options could be of value to providers and custody staff alike.
Generally, there is support for cognitive-behavioral therapy (CBT) in the treatment of offenders (
13,
14). CBT has been found to reduce recidivism rates (
15). Dialectical behavior therapy is associated with positive outcomes, but it has not found broad correctional use because of its cost and care intensity (
16–
18). Other CBT approaches in correctional systems, such as Moral Reconation Therapy, Thinking for a Change, and Reasoning and Rehabilitation, have shown encouraging results (
19–
22). However, no therapy shows particular superiority over others, with clear room left for improvement (
23,
24). Here we introduce a new option.
START NOW is an evidence-informed coping skills therapy designed for incarcerated individuals (
25–
27). A group therapy format is employed to optimize cost-effectiveness and offer participants a chance to provide feedback and support. A formative evaluation of START NOW in two prisons indicated high satisfaction rates among participants and reduced psychiatric hospitalization (
25). An unpublished quasi-experimental study of an adaptation of START NOW in a residential community treatment program reported a dose-response effect for START NOW; attendance at each program session resulted in a 2% reduction in the odds of rearrest and reincarceration (
26). The study reported here further investigated START NOW’s effectiveness by examining whether greater program participation was associated with fewer disciplinary reports in a large sample of incarcerated adults.
Methods
Design and Data Sources
We conducted a retrospective cohort analysis of participants who entered the START NOW program from 2010 through 2013. Inclusion criteria were age 18 or older at program initiation and incarceration for at least one month after program participation. The number of disciplinary reports was measured up to six months after participation.
Data were collected from electronic administrative records maintained by the Connecticut Department of Correction (CDOC) and Correctional Managed Health Care at UConn Health. Data were linked by a common identifier, deidentified, and delivered to the study team. The study was approved by CDOC and by UConn Health’s Institutional Review Board Panel 2, which maintains expertise on human subject protections for corrections populations.
Intervention
START NOW consists of 32 sessions in four units (foundational, emotion management, interpersonal, and future-focused skills) in a CBT framework as detailed elsewhere (
25–
27). Motivational interviewing and collaborative therapy engagement are theorized to enhance treatment adherence and effectiveness (
26). A facilitator manual provides detailed instructions for each session. All participant material is written at a fifth-grade reading level or below. Jargon is avoided, and iconic visual imagery, along with repetition, is used throughout (
26). START NOW was implemented in seven correctional facilities (one housing only female prisoners) and facilitated by formally trained master’s- and doctorate-level clinicians with ongoing clinical supervision and fidelity monitoring. Fidelity monitoring was conducted by both the facilitator and the supervisor with structured instruments (
26).
Population
The study population was all inmates (at least 18 years of age, of either sex, and of any race or ethnicity) who participated in START NOW between 2010 and 2013. Because an inmate could participate more than once, the unit of analysis was participation events, rather than individuals. Both sentenced and unsentenced inmates participated (Connecticut is one of six states currently with an integrated jail and prison system). Participation was not limited to inmates with a recorded psychiatric diagnosis. Our analysis excluded participants with a CDOC-assigned overall security risk or mental health care need score of 5 (highest risk or highest need), because these inmates constituted a group too small to analyze as a distinct group and because they resided in inpatient psychiatric units and would not be permitted to participate in the group format. Inmates were referred by a mental health professional, case worker, or correctional officer, or they were self-referred. No restrictions on primary psychiatric diagnosis or history of infractions were placed on participation beyond exclusion of inmates in segregation. Initially, the data contained 1,112 records. After data cleaning, there were 946 participation events, representing 846 unique inmates.
Measurements
Number of disciplinary reports.
The dependent variable was the count of disciplinary reports received up to six months after program participation. The CDOC sanctions inmates who commit offenses while in custody by issuing three classes of disciplinary reports ranging from A to C; A class offenses are the most serious (
28). This study combined A and B class offenses and omitted petty offenses (C class) from analysis because petty offenses are unreliably recorded.
Time at risk after participation (that is, time during which disciplinary reports were subject to being counted) was restricted to no less than one month and up to six months. Setting boundaries in the postperiod and allowing variation in time at risk were required to first ensure that there was a reasonable minimal time span to observe disciplinary infractions after participation and because inmates varied in time in custody after participation. As described below, our multivariate analysis accommodated variation in time at risk.
Number of sessions completed.
The focal independent variable was a simple count of number of sessions completed.
Overall risk score.
At admission, CDOC assigns inmates an overall risk score ranging from 1 to 5, which is periodically updated. CDOC classification staff assign a risk level through an evaluation of seven scoring criteria: escape profile, severity or violence of the current offense, history of violence, length of sentence, pending charges or detainers, discipline history, and gang membership (
27). We tested whether the overall risk score reduced the effect of the number of sessions attended on the number of disciplinary reports and whether risk score groups varied in the effect of number of sessions attended.
Psychiatric diagnosis and comorbidity.
The treating clinician enters psychiatric diagnoses (primary and co-occurring) into an electronic database. In this study, an inmate’s primary diagnosis was classified into one of six groups: no diagnosis; personality disorder; substance use disorder; psychotic disorder; mood disorder; or anxiety, posttraumatic stress disorder, or other diagnosis. We also evaluated the effect of the number of co-occurring diagnoses, a count that included the primary diagnosis. We investigated whether diagnosis and comorbidity attenuated the relationship between sessions attended and offense reports and whether primary diagnosis groups varied in the effect of the number of sessions attended.
Control variables.
We adjusted estimates for the effects of sociodemographic factors. Race-ethnicity was a set of mutually exclusive dummy variables, including black, white, Hispanic and other, as recorded by the CDOC. Education was measured in years of school completed. Sex was a dummy variable (male=1). Age was measured in years at the time of program initiation.
Modeling variables.
Number of days after program participation was a count of time at risk of receiving a disciplinary report in the postprogram period and was used to adjust estimates in multivariate analyses. Number of CDOC admissions was a simple count of prior intakes, including the current admission. Number of admissions was used as a predictor to model excess zeros in the logistic portion of the two-part zero-inflated negative binomial (ZINB) model, with the reasoning that those with fewer admissions would have greater impulse control than those with more admissions and would thus be less likely to receive any disciplinary reports.
Data Analysis
In descriptive analyses, we calculated the range, mean, and standard deviation for age and all count variables as well as number and percentage for all categorical variables. Multivariate analysis employed ZINB models. Most observations (N=801 of 946) involved no disciplinary reports. ZINB is a two-part model that separately accounts for zero-inflation via logistic regression and main effects via a negative binomial regression. These models are appropriate for overdispersed count data. Following the methods of the UCLA Institute for Digital Research and Education (
29), we found that the ZINB model was preferred to the zero-inflated Poisson model (likelihood ratio test=17.30, p<.001) for our data. Furthermore, a Vuong test indicated that zero-inflated models were superior to standard negative binomial models (z=1.60, p<.05); however adjustments for variation in exposure time or for clustering within the individual were not possible while running the Vuong test. Multivariate analysis presents incident rate ratios from ZINB models, with standard errors adjusted for clustering within the individual. Stata’s cluster(var) option for ZINB (
30) was used. Estimates also adjusted for variation in postprogram exposure time by using Stata’s exp(var) option (
30). Our primary analysis tested whether number of sessions had a negative effect on the count of disciplinary reports and whether this effect was robust to other study variables hypothesized to also predict number of disciplinary reports. We used number of CDOC admissions in the prediction of zeros in the logistic part of the two-part model. Because interaction coefficients are difficult to interpret in nonlinear models (
31), we investigated variation in the effect of the number of sessions attended across security risk groups and primary diagnosis groups via Stata’s margins commands and plotted the results (
30).
Results
Table 1 presents descriptive statistics from 946 participation events. The unadjusted mean number of disciplinary reports in the postprogram period was .30 (range=0–8). The mean number of sessions attended was 14.34 (range=1–32). Participants were fairly equally distributed across four security risk groups, each representing about 20%−30% of the sample. Half of the sample (50%) had no recorded psychiatric diagnosis. Mood disorder was the most common primary diagnosis classification (20%), followed by psychotic disorder (10%) and substance use disorder (7%). The mean number of comorbid psychiatric disorders was 1.17 (range=0–9). The great majority of the sample was male (92%). The mean age at program initiation was 35.68 (range=18–72). The racial-ethnic breakdown of the sample was as follows: white, 43%; black or African American, 36%; Hispanic, 20%; and other race-ethnicity, 1%. The mean number of years of school completed was 11.54 (range=1–18). The mean number of days observed in the postprogram period was 165.70 (range=30–180 by study design). Finally, the mean number of CDOC admissions was 6.52±6.40 (range=1–43).
Table 2 presents incident rate ratios and robust standard errors for six ZINB models of number of postprogram disciplinary reports regressed on number of program sessions attended and combinations of other study variables to elucidate specific effects. Model 1 indicates that more program sessions attended was associated with fewer disciplinary reports received in the postprogram period (p<.001). More specifically, there was a 5% decrease in the incident rate of disciplinary reports for every additional session attended. Model 2 adds the security risk group to the number of sessions. Compared with the incident rate of disciplinary reports for the lowest security risk group (security group 1), the rates for security groups 3 and 4, respectively, were 4.64 (p<.001) and 11.23 (p<.001) times as high.
Model 3 adds psychiatric diagnosis classification to number of sessions. Compared with the incident rate for the group lacking a psychiatric diagnosis, each of the diagnostic classifications had significantly greater rates, ranging from 3.77 times (substance use disorder diagnosis, p<.001) to 8.80 times (mood disorder diagnosis, p<.001). Model 4 adds number of comorbid psychiatric diagnoses to the predictors in model 3. There was a 17% increase in the incident rate of disciplinary reports for each additional diagnosis (p<.05). Although the independent effects of psychiatric diagnosis classification remained in model 4, the sizes of these relationships were slightly reduced when comorbidity was considered in the model. Model 5 includes number of sessions, security risk group, and psychiatric considerations. All significant relationships between the variables and the number of disciplinary reports that were observed in the other models remained significant. Model 6 adds sociodemographic controls to all other study variables and serves as the full, final model. Age was independently predictive of number of disciplinary reports (p<.001). A 4% decrease was noted in the incident rate of disciplinary reports for every additional year of age. Gender and race-ethnicity were not predictive factors. Across all models, number of program sessions attended appeared to be a particularly robust independent predictor of number of disciplinary reports.
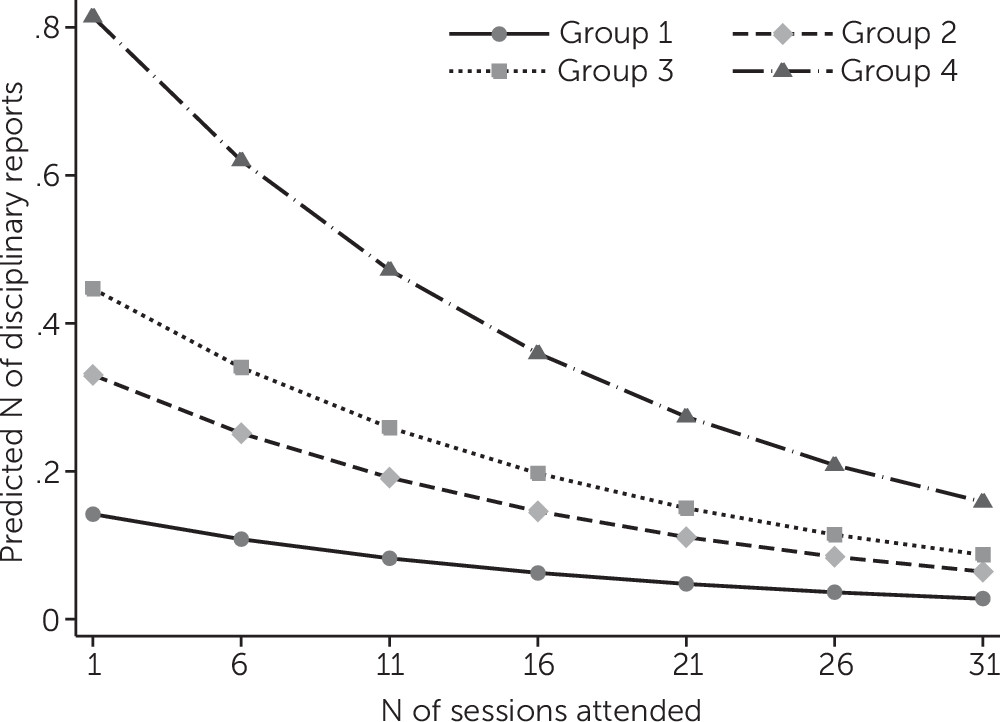
To further investigate the effect of number of program sessions attended on disciplinary reports by security risk groups and primary diagnosis groups, Stata’s margins postestimation command was utilized and plotted (
30).
Figure 1 depicts the predictive margins of security risk group predicting number of disciplinary reports by number of sessions attended. Generally speaking, all security risk groups benefited from more sessions attended. However, the higher the overall security risk score, the greater the reduction in number of disciplinary reports with more sessions attended.
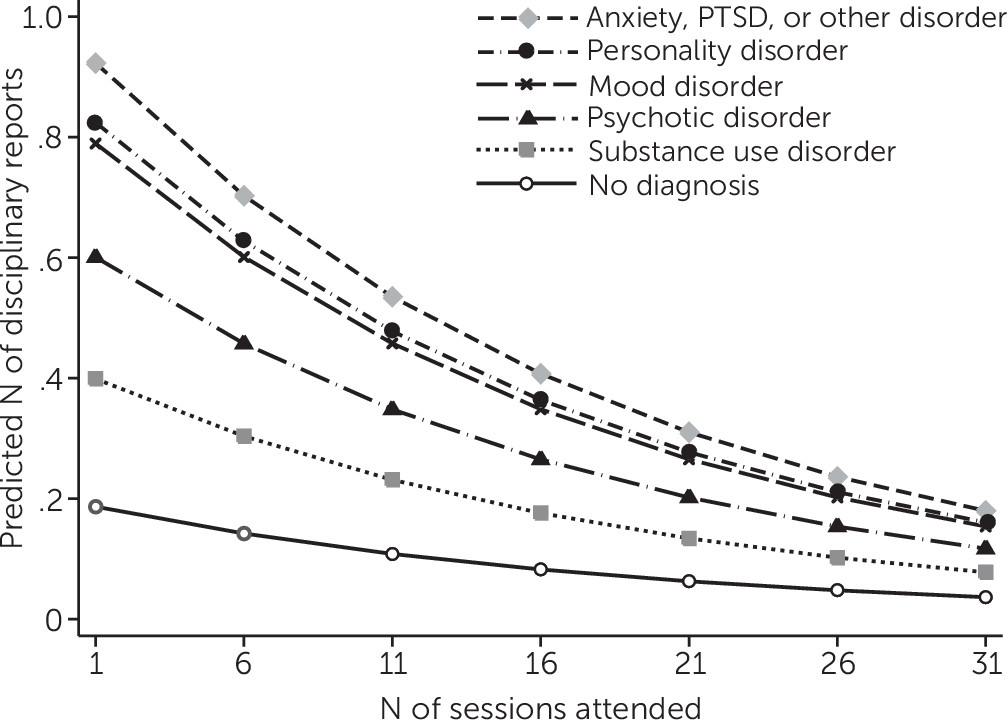
The same procedures followed for
Figure 1 were followed for
Figure 2 to plot the predicted margins of psychiatric diagnosis classifications. All diagnostic groups appear to have benefited from more sessions attended, and groups with the highest predicted number of infractions with few sessions attended benefited more with increasingly higher levels of participation.
Discussion
This study examined whether higher attendance in a group therapy program designed for inmates was associated with fewer disciplinary reports received in a state correctional system. Results indicate a significant reduction in the receipt of disciplinary reports in the postprogram period with a greater number of sessions attended. Generally, it has been found that longer treatment interventions produce more significant changes (
32,
33). A 5% decrease in the incident rate of disciplinary reports was found for every session attended. Despite the structural constraints present in correctional settings, such as frequent movement across facilities, this finding suggests that every effort should be made to retain participants in the program.
The study also examined whether security risk groups and primary psychiatric diagnosis classification groups varied in the relationship between sessions attended and disciplinary reports received. Results indicate that higher risk groups benefited most from more program participation. This suggests that when there is a waiting list of potential program participants, priority should be given to members of the groups with higher security risk. We also found that all diagnostic groups appeared to benefit from greater participation, although some groups more than others. In particular, inmates with anxiety, personality, and psychotic disorders had the steepest downward predicted number of disciplinary reports with more sessions attended. This finding may also suggest groups to target for participation and retention.
This study was not without limitations. The sample was limited to adults, and most were male offenders. Future studies should include youths and women in sufficient numbers to examine separately. Furthermore, this study did not include a control group. Future studies should seek to employ a prospective randomized comparative effectiveness design to further elucidate and compare the unique contributions of START NOW with alternative therapy options. Because of a very small sample and the distinct treatment context of offenders with the most restrictive security and care need scores, these participants were omitted from analyses. In addition, the relationship between number of sessions attended and number of reports received may not be entirely conclusive, because some inmates who engaged in behavioral infractions may have voluntarily or involuntarily discontinued participation sooner. Other inmates with high levels of impulse control may have self-selected into longer program participation. Finally, this study did not control for an inmate’s status (sentenced versus unsentenced) or participation in other (concurrent) treatment programs that may have had an impact on behavioral infractions. However, it must be acknowledged that the robust finding that number of sessions attended was associated with fewer reports strongly suggests a program effect.
Despite these limitations, this study adds evidence of the effectiveness of START NOW beyond that previously published (
27) and extends the knowledge base about the program’s effectiveness to the wider state correctional context. Future research will investigate the program’s impact on clinical outcomes in addition to behavioral outcomes. Additional outcomes to consider include the level and nature of offenses and ultimately, recidivism and hospitalization.
Conclusions
This study provides evidence that START NOW is effective in reducing the number of disciplinary reports received by inmates in correctional settings. The program is relatively inexpensive and flexible and is effective for a variety of inmate subpopulations. START NOW participation demonstrably reduced behavioral infractions and thereby eliminated the costs associated with disciplinary hearings that would have taken place. Of greater potential significance is the benefit to participants and the people with whom they interact, whether during incarceration or subsequent to release. Further work is needed to determine the extent of any such benefits.
Acknowledgments
The authors thank the Connecticut Department of Correction for providing data, making this work possible.