Suicide is a serious public health issue in the United States (
1). It is the tenth leading cause of death, after cardiovascular disease, cancer, and stroke (
1,
2). Studies suggest that prior suicidal behavior and psychiatric disorders are prominent factors that increase the likelihood of subsequent suicidal events (
3). Research also indicates that use of mental health services can help protect against suicide risk (
3). Yet, most studies on mental health service use have not considered prior suicidal behavior (
4–
6). Thus because suicide is a leading public health concern, research examining service use by adults with a history of suicidal behavior is crucial.
Previous studies on mental health service use have focused on adults with mood or anxiety disorders, without consideration of those with prior suicidal behavior (
4–
6). Current understanding of service use may therefore not reflect the unique patterns of use by adults with prior suicidal behavior and current mood or anxiety disorders. Furthermore, although suicide and suicide risk vary by major health disparity factors such as race-ethnicity, age, and gender (
7,
8), few studies have considered these differences in the examination of service use, and no study to our knowledge has investigated how these factors may work together to affect use. Thus research investigating racial-ethnic, age, and gender disparities in mental health service use by adults with a history of suicidal behavior and current mood or anxiety disorders is needed. Findings from such studies will inform understanding of use and help to identify adults in need of care.
Data from the Collaborative Psychiatric Epidemiology Surveys (CPES, 2001–2003) uniquely address these limitations. In contrast to surveys used in previous studies, the CPES provides data on clinically based measures of prior suicidal behavior and mood and anxiety disorders. The CPES is also nationally representative of the racial-ethnic, age, and gender distributions of noninstitutionalized, community-dwelling adults in the United States.
CPES data were used in this investigation to determine nationally representative prevalence estimates of current mental health service use by adults with prior suicidal behavior and current mood or anxiety disorders in the United States and to examine racial-ethnic, age, and gender differences in use.
Methods
The CPES sample consisted of 1,139 adults (≥18 years). All adults had prior nonfatal suicidal behavior (based on a lifetime assessment of suicidal ideation, plans, and attempts) and satisfied DSM-IV criteria for current mood disorders (major depressive disorder, dysthymia, and bipolar disorders types I and II) or anxiety disorders (panic disorder, agoraphobia without panic, specific phobia, social phobia, generalized anxiety disorder, and posttraumatic stress disorder) in the past 12 months, as determined by the World Mental Health Composite International Diagnostic Interview (WMH-CIDI). Only adults with prior suicidal behavior and current mood or anxiety disorders were eligible for the study. All data were from the Inter-University Consortium for Political and Social Research. Participant consent was not obtained in this investigation because the study involved the analysis of secondary data. The institutional review boards of the University of California, San Francisco, and the San Francisco Veterans Affairs Medical Center approved this study.
The WMH-CIDI assessed mental health service use. Current mental health service use was defined as specialty mental health (psychiatrist, psychologist, other mental health professional, social worker, or counselor in a mental health specialty setting; overnight hospital stay; or mental health hotline use) or general medical (primary care physician, other general practitioner or family doctor, nurse, occupational therapist, or other nonspecialty mental health professional) service use for “emotions, nerves, mental health, or use of alcohol or drugs” (
5) in the past 12 months. In this study, current mental health service use was examined across three major health disparity factors—race-ethnicity (non-Hispanic white, African American, or Hispanic or other) (
5), age (younger age, 18–34 years; middle, 35–54; or older, ≥55), and gender.
Clustering and weighting techniques that reduce systematic bias and imprecision in a complex sampling design were implemented to produce nationally representative prevalence estimates of current mental health service use that are generalizable to community-dwelling adults in the United States. Statistical differences were estimated by the Rao-Scott chi square statistic, and standard errors were determined from a recalculation of variance that used the Taylor series linear approximation method. To evaluate whether prevalence trends across the life course varied by race-ethnicity and gender, interaction terms with age modeled as continuous as well as main effects were examined in logistic regression analyses.
Reported results are based on weighted analyses unless otherwise noted. Statistical significance was defined as p<.05. All analyses were performed with SAS (PROC SURVEY, version 9.3).
Results
The unweighted sample mean±SD age was 38.6±13.7 years. The sample distribution was 41.7% younger age, 45.1% middle age, and 13.2% older age; 44.3% non-Hispanic white, 27.0% African American, and 28.7% Hispanic or other (18.4% Hispanic, 6.5% Asian, and 3.8% other); and 69.4% female, with whites being older, more educated, and more evenly located throughout the United States. Furthermore, over 70% of the sample had prior suicidal behavior within the past ten years, and nearly half had prior suicidal behavior within the past three years. The sample distribution of prior suicidal behavior was 43.6% ideation only, 13.8% plan without an attempt, 26.9% plan with an attempt, and 15.6% attempt without a plan (an impulsive attempt).
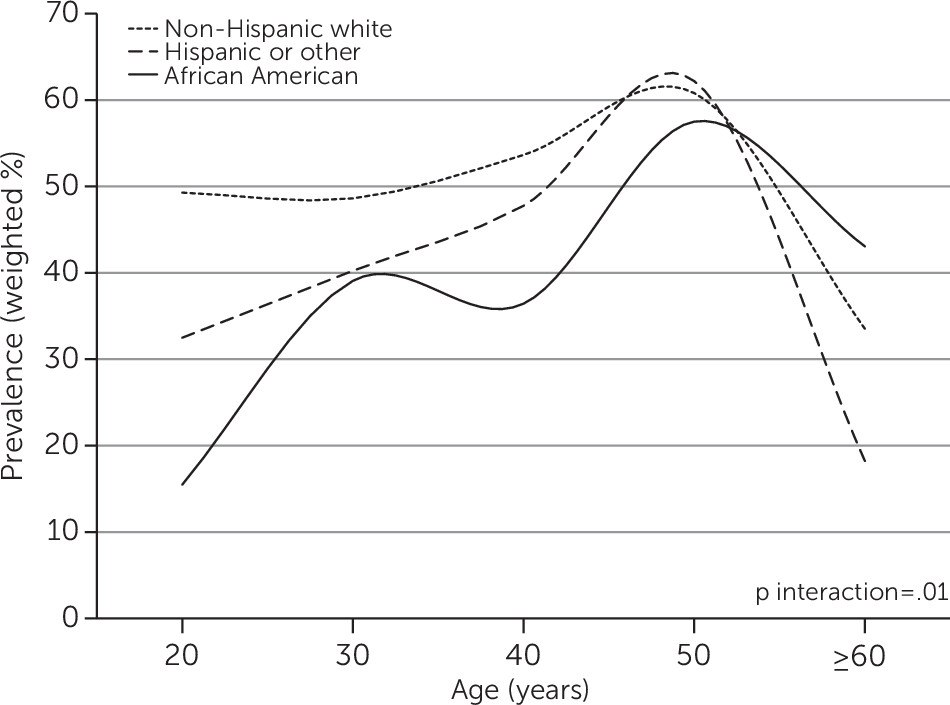
Overall, the weighted current mental health service use was 47.3%. African Americans showed the lowest use (32.2%) compared with whites (50.7%) and Hispanics or others (41.0%) (Rao-Scott χ2=17.1, df=2, p<.001), whereas adults of middle age showed the highest use (52.6%) compared with adults of younger (41.9%) and older (43.8%) ages (Rao-Scott χ2=7.2, df=2, p=.03). Service use was similar between men (48.0%) and women (46.9%).
Across the life course, African Americans showed increasing service use that was not seen among whites, Hispanics, and others, all of whose use decreased in the latter half of the life course (p interaction=.01;
Figure 1). Among those of younger age, African Americans had the lowest service use (19.2%) compared with whites (47.5%) and Hispanics and others (35.1%) (Rao-Scott χ
2=17.8, df=2, p<.001). A similar trend was seen in middle age despite overall increases in service use. However, racial-ethnic disparity was absent in older age when African Americans showed much greater service use (61.9%) that paralleled use by whites (44.0%) and Hispanics or others (35.8%) (Rao-Scott χ
2=1.8, df=2, p=.40). This rise appeared to be motivated by greater use of general medical services from younger (8.1%) to middle (17.6%) and older (54.2%) age, a pattern not seen with whites (21.0%, 34.6%, and 35.7%, respectively) and Hispanics or others (23.6%, 33.3%, and 15.8%, respectively). Such a trend was also not seen for specialty mental health service use. Similar results were obtained from sensitivity analyses involving adults with a recent history (≤3 years) of suicidal behavior and current mood or anxiety disorders, indicating that the reported findings were independent of the timing of suicidal behavior.
Finally, no gender differences in use were found across the life course and within age groups.
Discussion
This study determined nationally representative prevalence estimates of current mental health service use by adults with prior suicidal behavior and current mood or anxiety disorders. Three key findings are important to highlight.
First, overall service use was low (<50%). This finding is consistent with previous research suggesting that adults with current suicidal ideation and mood or anxiety disorders have low use (42% and 52%, respectively) (
9). Other studies have also found similar results among adults with no known prior suicidal behavior but with current mood, anxiety, or substance use disorders (
4–
6,
10). Although past research indicates that suicidal behavior motivates service use (
10,
11), our results demonstrate that even adults with a history of suicidal behavior and current psychiatric disorders likely have low use.
Second, across the life course, African Americans showed increasing service use that paralleled use by whites, Hispanics, and others. Although prior studies suggest that adults from racial-ethnic minority groups who have mood, anxiety, or substance use disorders or symptoms have lower use of services compared with whites (
5,
12,
13), few studies have considered racial-ethnic disparities in service use across the life course. Moreover, no study to our knowledge has examined whether these differences pertain to adults with prior suicidal behavior and current mood or anxiety disorders.
Third, the increase in service use across the life course by African Americans was driven by greater use of general medical services. This finding is consistent with previous research that has found that with age, African Americans show considerably higher general medical service use for mental health treatment than whites show (
14,
15). Our findings thus support that African Americans with a history of suicidal behavior and current psychiatric disorders also have rising general medical service use throughout the life course.
This study had strengths and limitations. It was the first to determine nationally representative prevalence estimates of current mental health service use by adults with prior suicidal behavior and current mood or anxiety disorders. It is also among the few to examine racial-ethnic, age, and gender differences in use and to provide results that are generalizable to community-dwelling adults in the United States. However, this study also had limitations. The CPES underrepresents homeless, institutionalized, old-old (75–84 years), and oldest-old (≥85 years) adults. Thus, given that our sample consisted of noninstitutionalized, community-dwelling adults, power for analyses of the oldest-old segment of the life course was limited. Power for analyses related to suicidal behavior severity (plans and attempts) was also limited, and potential cohort effects—although difficult to assess in this study—should be considered. Finally, stigma may have discouraged adults with psychiatric conditions from survey participation, and validation of self-reported service use was unavailable.
Conclusions
Our findings are informative yet concerning, in that even adults with prior suicidal behavior and current psychiatric disorders underutilized mental health services. Although our results revealed racial-ethnic differences in service use, they emphasize the enduring tendency of African Americans to use general medical services for their source of mental health treatment, thereby further supporting the need for psychiatric and general medical care integration. However, research is needed to explore how family, friends, community members, and technology can also provide support that can help reduce suicide and suicide risk.