Competitive Employment Outcomes Among Veterans in VHA Therapeutic and Supported Employment Services Programs
Abstract
Objective:
Methods:
Results:
Conclusions:
Methods
Data Sources and Sample Selection
Dependent and Independent Variables
Covariates
Statistical Analyses
Results
Sample Description
| All (N=38,199) | Competitively employed (N=11,928) | Not competitively employed (N=26,271) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | N | % | N | % | N | % | χ2 | df | p |
| Demographic, clinical, and social | |||||||||
| Gender | .0 | 1 | .985 | ||||||
| Male | 35,815 | 93.8 | 11,184 | 31.2 | 24,631 | 68.8 | |||
| Female | 2,384 | 6.2 | 744 | 31.2 | 1,640 | 68.8 | |||
| Age | 73.8 | 1 | <.001 | ||||||
| 18–44 | 9,140 | 23.9 | 3,186 | 34.9 | 5,954 | 65.1 | |||
| 45–64 | 29,059 | 76.1 | 8,742 | 30.1 | 20,317 | 69.9 | |||
| Race | 1.2 | 2 | .547 | ||||||
| Caucasian | 20,064 | 52.5 | 6,281 | 31.3 | 13,783 | 68.7 | |||
| Black | 17,453 | 45.7 | 5,447 | 31.2 | 12,006 | 68.8 | |||
| Other | 682 | 7.8 | 200 | 29.3 | 482 | 70.7 | |||
| Marital status | 52.3 | 2 | <.001 | ||||||
| Single or widowed | 11,718 | 30.7 | 3,407 | 29.1 | 8,311 | 70.9 | |||
| Married | 5,992 | 15.7 | 2,054 | 34.3 | 3,938 | 65.7 | |||
| Separated or divorced | 20,489 | 53.6 | 6,467 | 31.6 | 14,022 | 68.4 | |||
| Education | 34.8 | 2 | <.001 | ||||||
| Less than high school diploma | 1,823 | 4.8 | 460 | 25.2 | 1,363 | 74.8 | |||
| High school diploma or GED | 19,265 | 50.4 | 6,000 | 31.1 | 13,265 | 68.9 | |||
| More than high school diploma or GED | 17,111 | 44.8 | 5,468 | 32.0 | 11,643 | 68.0 | |||
| Military service era | 150.3 | 3 | <.001 | ||||||
| Vietnam | 12,535 | 32.8 | 3,399 | 27.1 | 9,136 | 72.9 | |||
| Post-Vietnam | 18,826 | 49.3 | 6,200 | 32.9 | 12,626 | 67.1 | |||
| Persian Gulf | 4,770 | 12.5 | 1,611 | 33.8 | 3,159 | 66.2 | |||
| OEF/OIFa | 2,068 | 5.4 | 718 | 34.7 | 1,350 | 65.3 | |||
| Anxiety disorder other than PTSD | 15.0 | 1 | <.001 | ||||||
| Yes | 6,155 | 16.1 | 1,793 | 29.1 | 4,362 | 70.8 | |||
| No | 32,044 | 83.4 | 10,135 | 31.6 | 21,909 | 68.4 | |||
| Depressive disorder | 40.0 | 1 | <.001 | ||||||
| Yes | 14,637 | 38.3 | 4,292 | 29.3 | 10,345 | 70.7 | |||
| No | 23,562 | 61.7 | 7,636 | 32.4 | 15,926 | 67.6 | |||
| PTSD | 77.8 | 1 | <.001 | ||||||
| Yes | 7,393 | 19.4 | 1,993 | 27.0 | 5,400 | 73.0 | |||
| No | 30,806 | 80.7 | 9,935 | 32.3 | 20,871 | 67.8 | |||
| Bipolar disorder | 98.0 | 1 | <.001 | ||||||
| Yes | 5,293 | 13.9 | 1,343 | 25.4 | 3,950 | 74.6 | |||
| No | 32,906 | 86.1 | 10,585 | 32.2 | 22,321 | 67.8 | |||
| Schizophrenia spectrum or other psychotic disorder | 371.9 | 1 | <.001 | ||||||
| Yes | 4,082 | 10.7 | 735 | 18.0 | 3,347 | 82.0 | |||
| No | 34,117 | 89.3 | 11,193 | 32.8 | 22,924 | 67.2 | |||
| Adjustment disorder | .0 | 1 | .962 | ||||||
| Yes | 2,821 | 7.4 | 882 | 31.3 | 1,939 | 68.7 | |||
| No | 35,378 | 92.6 | 11,046 | 31.2 | 24,332 | 68.8 | |||
| Alcohol abuse or dependence | .0 | 1 | .929 | ||||||
| Yes | 24,006 | 62.8 | 7,500 | 31.2 | 16,506 | 68.7 | |||
| No | 14,193 | 37.2 | 4,428 | 31.2 | 9,765 | 68.8 | |||
| Drug abuse or dependence | 2.04 | 1 | .153 | ||||||
| Yes | 21,209 | 55.5 | 6,687 | 31.5 | 14,552 | 68.5 | |||
| No | 16,990 | 44.5 | 5,241 | 31.0 | 11,749 | 69.2 | |||
| Personality disorder | 22.1 | 1 | <.001 | ||||||
| Yes | 2,482 | 6.5 | 670 | 27.0 | 1,812 | 73.0 | |||
| No | 35,717 | 93.5 | 11,258 | 31.5 | 24,459 | 68.5 | |||
| Other psychiatric diagnosis | 38.3 | 1 | <.001 | ||||||
| Yes | 3,024 | 7.9 | 793 | 26.2 | 2,231 | 73.8 | |||
| No | 35,175 | 92.1 | 11,135 | 31.7 | 24,040 | 68.3 | |||
| N of general medical diagnoses | 237.0 | 2 | <.001 | ||||||
| 0 | 8,395 | 22.0 | 3,161 | 37.7 | 5,234 | 62.4 | |||
| 1–5 | 29,341 | 76.8 | 8,685 | 29.6 | 20,656 | 70.4 | |||
| >5 | 463 | 1.2 | 82 | 17.7 | 381 | 82.3 | |||
| Employment pattern in prior 3 years | 1028.1 | 2 | <.001 | ||||||
| Competitive employment | 18,639 | 48.8 | 7,170 | 38.5 | 11,469 | 61.5 | |||
| Irregular employment | 6,881 | 18.0 | 2,039 | 29.6 | 4,842 | 70.4 | |||
| Unemployed, retired, disabled, student, volunteer, or other | 12,679 | 33.2 | 2,719 | 21.4 | 9,960 | 78.6 | |||
| Homeless | 9.16 | 1 | .003 | ||||||
| Yes | 20,702 | 54.2 | 6,601 | 31.9 | 14,101 | 68.1 | |||
| No | 17,497 | 45.8 | 5,327 | 30.5 | 12,170 | 69.6 | |||
| Financial assistanceb | 575.6 | <.001 | |||||||
| Yes | 18,729 | 49.0 | 4,762 | 25.4 | 13,967 | 74.6 | |||
| No | 19,470 | 51.0 | 7166 | 36.8 | 12,304 | 63.2 | |||
| Fiscal year of discharge from TSES program | 226.1 | 4 | <.001 | ||||||
| 2006 | 3,266 | 8.6 | 1,169 | 35.8 | 2,097 | 64.2 | |||
| 2007 | 6,628 | 17.4 | 2,402 | 36.2 | 4,226 | 63.8 | |||
| 2008 | 8,112 | 21.2 | 2,703 | 33.3 | 5,409 | 66.7 | |||
| 2009 | 9,418 | 24.7 | 2,687 | 28.5 | 6,731 | 71.5 | |||
| 2010 | 10,775 | 28.2 | 2,967 | 27.5 | 7,808 | 72.5 | |||
| Employment services | |||||||||
| Main type of TSES | 100.6 | 4 | <.001 | ||||||
| No main type of TSES | 2,360 | 6.2 | 682 | 28.9 | 1,678 | 71.0 | |||
| Supported employment | 8,040 | 21.0 | 2,427 | 30.2 | 5,613 | 69.8 | |||
| Transitional work in the community | 2,409 | 6.3 | 910 | 37.8 | 1,499 | 62.2 | |||
| Transitional work in a VA medical center | 21,953 | 57.5 | 7,003 | 31.9 | 14,950 | 68.1 | |||
| Incentive therapy or sheltered workshop | 3,437 | 9.0 | 906 | 26.4 | 2,531 | 73.6 | |||
| Prevocational assessment or training | 62.4 | 1 | <.001 | ||||||
| Yes | 4,680 | 12.3 | 1,696 | 36.2 | 2,984 | 63.8 | |||
| No | 33,519 | 87.8 | 10,232 | 30.5 | 23,287 | 69.5 | |||
| Job club or vocational support group | 204.6 | 1 | <.001 | ||||||
| Yes | 11,340 | 29.7 | 4,133 | 36.5 | 7,207 | 63.6 | |||
| No | 26,859 | 70.3 | 7,795 | 29.0 | 19,064 | 71.0 | |||
| Volunteer work | 30.8 | 1 | <.001 | ||||||
| Yes | 307 | .8 | 51 | 16.6 | 256 | 83.4 | |||
| No | 37,892 | 99.2 | 11,877 | 31.3 | 26,105 | 68.7 | |||
| Time in TSES program | 139.8 | 2 | <.001 | ||||||
| <6 months | 22,570 | 59.1 | 6,551 | 29.0 | 16,019 | 71.0 | |||
| 6–12 months | 10,851 | 28.4 | 3,838 | 35.4 | 7,013 | 64.6 | |||
| >12 months | 4,778 | 12.5 | 1,539 | 32.2 | 3,239 | 67.8 | |||
| Concerned about loss of financial assistance if employed | 166.2 | 1 | <.001 | ||||||
| Yes | 960 | 2.5 | 117 | 12.2 | 843 | 87.8 | |||
| No | 37,239 | 97.5 | 11,811 | 31.7 | 25,428 | 68.3 | |||
Predictors of Competitive Employment
| Variable | OR | 95% CI |
|---|---|---|
| Male (reference: female) | .98 | .89–1.08 |
| Age 45–64 (reference: 18–44) | .96 | .89–1.03 |
| Race (reference: Caucasian) | ||
| Black | .93 | .89–.98 |
| Other | .93 | .78–1.11 |
| Marital status (reference: single or widowed) | ||
| Married | 1.35*** | 1.26–1.45 |
| Separated or divorced | 1.15 | 1.09–1.22 |
| Education (reference: high school diploma or GED) | ||
| Less than high school diploma | .81*** | .72–.90 |
| More than high school diploma | 1.06*** | 1.01–1.11 |
| Military service era (reference: Vietnam) | ||
| Post-Vietnam | 1.24 | 1.18–1.31 |
| Persian Gulf | 1.30* | 1.18–1.44 |
| OEF/OIFa | 1.37** | 1.21–1.56 |
| Anxiety disorder other than PTSD (reference: no) | .96 | .93–1.06 |
| Depressive disorder (reference: no) | .89*** | .85–.94 |
| PTSD (reference: no) | .85*** | .80–.90 |
| Bipolar disorder (reference: no) | .73*** | .68–.79 |
| Schizophrenia spectrum or other psychotic disorder (reference: no) | .51*** | .46–.55 |
| Adjustment disorder (reference: no) | 1.02 | .93–1.11 |
| Alcohol abuse or dependence (reference: no) | .91*** | .87–.96 |
| Drug abuse or dependence (reference: no) | 1.06* | 1.01–1.12 |
| Personality disorder (reference: no) | .93 | .84–1.02 |
| Other psychiatric diagnosis (reference: no) | .83*** | .76–.90 |
| N of general medical diagnoses (reference: 0) | ||
| 1–5 | .81 | .77–.86 |
| >5 | .57*** | .44–.73 |
| Employment pattern in prior 3 years (reference: competitive employment) | ||
| Irregular employment | .71 | .67–.75 |
| Unemployed, retired, disabled, student, volunteer, or other | .53*** | .50–.56 |
| Homeless (reference: no) | .96 | .91–1.01 |
| Financial assistance (reference: no) | .71*** | .68–.75 |
| Fiscal year of discharge (reference: 2006) | ||
| 2007 | .97*** | .88–1.06 |
| 2008 | .83* | .76–.91 |
| 2009 | .64*** | .58–.70 |
| 2010 | .60*** | .55–.66 |
| Employment services | ||
| Main type of TSES received (reference: transitional work in a VA medical center) | ||
| Supported employment | 1.25*** | 1.17–1.34 |
| Transitional work in the community | 1.24*** | 1.14–1.36 |
| Incentive therapy or sheltered workshop | .85*** | .78–.92 |
| No main type of TSES | 1.00 | .90–1.10 |
| Prevocational assessment or training (reference: no) | 1.12** | 1.04–1.20 |
| Job club or vocational support group (reference: no) | 1.32*** | 1.25–1.40 |
| Volunteer work (reference: no) | .55*** | .40–.76 |
| Time in TSES program (reference: <6 months) | ||
| 6–12 months | 1.53*** | 1.46–1.61 |
| >12 months | 1.70*** | 1.57–1.83 |
| Concerned about loss of financial assistance if employed (reference: no) | .35*** | .29–.43 |
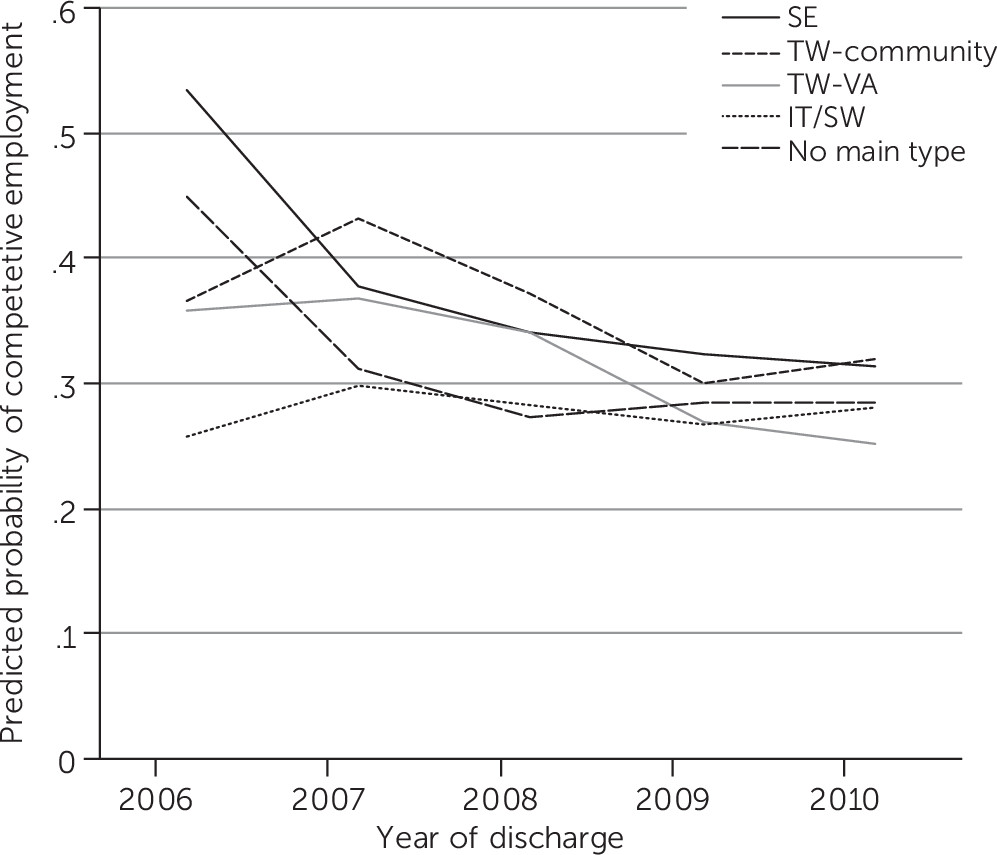
| Main type of TSES | Predicted probability |
|---|---|
| Supported employment | 34.9* |
| Transitional work in the community | 34.8* |
| Transitional work in a VA medical center | 30.3 |
| Incentive therapy or sheltered workshop | 27.2* |
| No main type of TSES | 30.3 |
Competitive Employment by Main Type of TSES Received Across Time
Discussion
Conclusions
Acknowledgments
References
Information & Authors
Information
Published In
Cover: Glowing Night, by Oscar Bluemner, 1924. Watercolor and pencil on paper. Bequest of Charles F. Ikle, 1963. © The Metropolitan Museum of Art, New York City. Image source: Art Resource, New York City.
History
Keywords
Authors
Competing Interests
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).