Parental depression is a critical public health concern, particularly among individuals involved in the child welfare system. Depression affects about 7.5 million parents in the United States and places about 20% of children at risk of adverse health outcomes (
1). Parents involved in the child welfare system are disproportionately affected, with over 33% indicating depressive symptoms and nearly 25% meeting criteria for a major depressive episode in the past year (
2), compared with 7% of adults in the general population (
3). In addition, depression does not ameliorate over time for these families (
2).
Consequences of parental depression for children have been extensively documented. Parents who experience depressive episodes are less engaged with their children (
4), less able to regulate affect or behavior during interactions with their children (
5), and both talk and read less with their children (
6). These behaviors contribute to increased child emotional and behavioral problems, as well as social and achievement deficits (
7). Maternal depression predicts higher levels of internalizing and externalizing disorders among children, general psychopathology and negative affect and behavior, and lower levels of positive affect and behavior (
8). Depressed mothers struggle to attend to health, safety, and prevention requirements, with implications for healthy child development (
9). Short- and long-term negative consequences of child maltreatment for children are well documented. Among mothers investigated for child maltreatment, depression was positively associated with neglectful parenting, emotional maltreatment, and psychological aggression (
10,
11), leading to child outcomes such as conduct disorder and poor emotional adjustment (
12).
The impact of parental depression on children cuts across race and ethnicity (
13). However, the prevalence of depression differs for various U.S. racial and ethnic populations. The prevalence of depression among Black adults is equivocal because of insufficient data (
14) and mixed findings. Compared with White adults, Black adults have reported lower rates of major depression (
15,
16), although prevalence among African Americans has also been reported as being twice as high as among White Americans (
17). Hispanic adults have reported higher rates of depression compared with White adults, although this finding is tenuous (
15,
16). Since the turn of the century, the Hispanic population has grown to represent the second-largest racial or ethnic group in the United States, behind non-Hispanic Whites, with non-Hispanic Blacks the third-largest group. Despite consistent evidence that families from racial and ethnic minority groups are disproportionately overrepresented in U.S. child welfare systems (
18), limited research has investigated how depression affects parents from these groups who are involved with child welfare systems. Better understanding of parental depression among child welfare–involved families is particularly timely, because of shifting demographic patterns nationwide and specifically within large racially and ethnically diverse urban populations.
Many child welfare–involved parents participate in home visitation programs, which are widely used, recovery-oriented, prevention and early intervention strategies for child abuse and neglect. Such programs aim to enhance parenting competence, teach problem-solving skills that promote self-efficacy, and focus on improving parent-child relationships, often a key stressor for families (
19). Home visitation programs are often delivered by home visitors employed by local community-based organizations. As adjunct service providers separate from child protective service caseworkers, home visitors frequently serve as supports for parents.
High rates of depression are notable among parents involved in home visitation programs (
20), and whether parental depression changes during home visitation participation is unclear. One study found that mothers who received home visitation experienced significantly greater reductions in depressive symptoms, compared with those who received community services (
21). Among child welfare–involved families receiving evidence-based home visitation, improvement in depressive symptoms was correlated with increased social support, reduced interpersonal conflict, and reduced parenting stress (
22). Others have found no difference in depression for parents participating in an evidence-based home visitation program (
23). Understanding parental depression over time for parents from racial and ethnic minority groups who participate in home visitation offers a great public health opportunity, because adults from minority groups tend to use traditional mental health services at significantly reduced rates (
24,
25), and community-based programs may serve as a support for families who avoid standard service delivery settings.
This study aimed to identify predominant profiles of depressive symptoms among child welfare–involved parents, describe changes in depressive symptoms for parents receiving services, and determine how profiles of depressive symptoms vary by race and ethnicity. Given the high prevalence of depression among child welfare–involved parents, this study presented a vital opportunity to understand patterns of depression among vulnerable parents by using a public-sector program aiming to improve parental self-efficacy and the health of parent-child relationships. We hypothesized that distinct depressive profiles would emerge, greater participation in services would be associated with lower levels of depressive symptoms, and depression profiles would vary by race and ethnicity. Increased understanding of depression profiles can inform priorities for service delivery, guiding prevention and intervention efforts (
26).
Methods
This study was part of the Interagency Collaborative Team project, which examined a systemwide, evidence-based practice implementation and focused on understanding outer-system and inner-organizational context factors (
27) associated with the effective implementation and sustainment of an in-home parenting intervention for child welfare–involved parents—SafeCare (
28). SafeCare is an evidence-based program demonstrated to improve parental outcomes in better management of children’s health, increased home safety, and more positive and sensitive parent-child interaction (
29–
31). In the child welfare context, SafeCare has been shown to significantly reduce maltreatment recidivism relative to standard family preservation and family reunification services (
32). SafeCare shares several features commonly found among evidence-based programs—a clear structure guiding its delivery, specific modules and topical content, and a model of change for guiding the practice patterns of home visitors working with parents. Program completion takes an average of 18 visits over 6 months. Participants in this study were parents receiving SafeCare (N=2,328) between 2012 and 2016 in a large, diverse service system. Parents eligible for the study were those referred to the SafeCare program for child neglect, who were at least 18 years old and who had at least one child in the family under age 12. Enrollment was >90%.
During study enrollment, parents provided demographic information and answered the Centers for Epidemiological Studies Depression Scale (CES-D) (
33) on a Web-based platform via a tablet device. The CES-D is a 20-item assessment of depressive symptoms, with demonstrated reliability and validity across racial and ethnic groups. Possible scores range from 0 to 60, with a “clinical” threshold of 16 indicating individuals at risk of clinical depression. Parents in this study completed the CES-D at baseline and at approximately every sixth home visit until service termination or program completion—up to a total of four times. All data collection procedures were approved by the University of California, San Diego, Institutional Review Board.
Statistical Analyses
We examined trajectories of depressive symptoms by using latent class growth analysis (LCGA) in Mplus, version 7.4. LCGA is a type of growth mixture modeling wherein sample heterogeneity is divided into a finite number of latent classes on the basis of profiles of indicator variables, and growth parameters are assumed to be invariant within classes (
34,
35). LCGA is well suited for discriminating classes defined by different developmental trajectories, because indicator variables can include measures from successive time points and the model incorporates growth parameters relating the indicator variables to time.
CES-D scores at successive time points from baseline to time 4 were used as indicator variables from which latent classes were derived. Models fitting between 1 and 5 classes were assessed multiple times by using random sets of starting values, followed by final optimizations ranging from 2 to 10. Gender, race-ethnicity, and age at the time of baseline assessment were considered as potential covariates on CES-D scores at all time points.
The optimally fitting classification model was determined through an iterative examination of fit indices (
35). The Bayesian information criterion (BIC) (
36) and sample-size–adjusted BIC (ABIC) are calculated from the log-likelihood of the model and the number of parameters in the model, and lower values suggest better model fit. The Akaike information criterion (AIC) (
37), assessed by the likelihood function accounting for estimated parameters, uses minimum AIC values to represent better model fit. The Vuong-Lo-Mendell-Rubin (LMR) test (
38) assesses the discrepancies in the likelihood between the model being tested with a model with one fewer class. Significant LMR results indicate that a K-class model fits the data better than a model with K-1 classes. Entropy for each model was also assessed, and values above 0.8 indicate that individuals are classified with confidence (
39).
Results
Sample Characteristics
Of the 2,328 participants, 219 (9%) identified their race as something other than non-Hispanic White, non-Hispanic Black, or Hispanic and were excluded because of small sample sizes. Of the remaining 2,109 persons, 1,268 (60%) completed both a baseline and time 2 CES-D assessment and were included in the LCGAs described below.
Table 1 summarizes demographic characteristics of the sample. Most participants were female and Hispanic, and most were either single or separated, divorced, or widowed. The mean age of the sample was 29 years. No demographic variables, including race and ethnicity, significantly differed between those who completed fewer than two CES-D assessments and those who completed two or more. In addition, no differences in attrition (noncompletion of a second assessment) were noted by service termination reason (i.e., moved out of the service area, lost to follow-up, or child welfare case closed). Notably, 40% of parents did not complete a second assessment. Results from chi-square and independent-samples t tests suggested that baseline CES-D scores significantly differed between individuals who completed fewer than two CES-D assessments and those who completed two or more CES-D assessments. Parents who completed only one CES-D assessment reported higher levels of depressive symptoms (t=5.33, df=2,107, p<0.001).
Depressive Profiles Over Time
Multiple LCGAs were employed to uncover classes of depressive trajectories. Iterative, unconditional latent class models with two through five classes specified were first explored (
35).
Table 2 presents fit indices associated with each LCGA. An examination of fit indices from these analyses suggested that a three-class model best fit the data (AIC=23,208.8; BIC=23,270.6; ABIC=23,232.4; LMR=418.4; p<0.001; entropy=0.84). Results suggested that a high proportion of study participants constituted class 1 (N=888), whose CES-D scores began at low to mild levels of depressive symptoms (β
0= 4.90) and improved significantly over time (β
1=–0.46, p<0.001) (
Table 3). A modest proportion of study participants constituted class 2 (N=306), whose CES-D scores began at borderline levels of depressive symptoms (β
0=12.89) and improved significantly over time (β
1=–0.81, p<0.001). A small number of participants constituted class 3 (N=74), whose CES-D scores began at high levels of depressive symptoms (β
0=23.63) and did not improve significantly over time. Following the unconditional models, separate conditional latent class models with age, gender, and race-ethnicity as covariates were explored. Results from these analyses suggested differences in class intercepts as a function of race-ethnicity (three-class model intercept on race-ethnicity=0.40, SE=0.21, p<0.05).
Depressive Profiles by Race-Ethnicity
Follow-up LCGAs with two through five classes specified were employed separately for non-Hispanic White, non-Hispanic Black, and Hispanic participants.
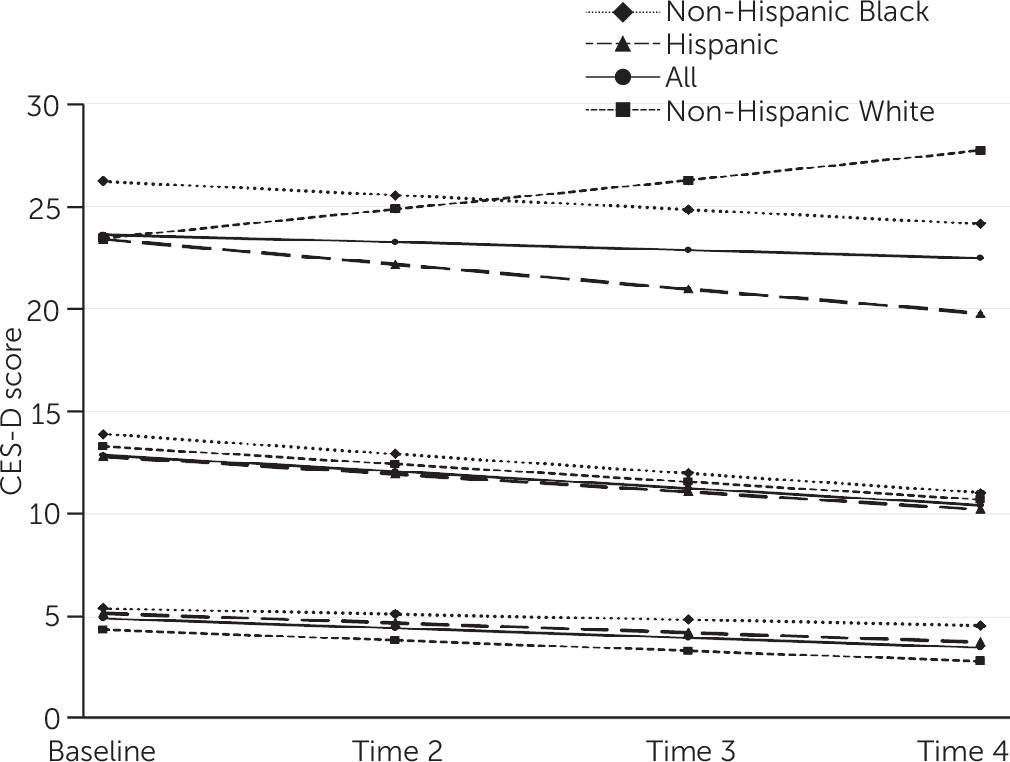
Figure 1 illustrates resulting depression trajectories for each racial-ethnic group. For all groups, a three-class model best fit the data (
Table 2).
Results for the depression profiles by race-ethnicity are presented in
Table 3. For non-Hispanic White, non-Hispanic Black, and Hispanic parents, the greatest proportion of parents formed the class with consistently low CES-D scores, with proportions of 71%, 65%, and 72% respectively. For non-Hispanic White and Hispanic parents from this class, CES-D scores were low at baseline and improved significantly over time (non-Hispanic White, β
0=4.4, β
1=–0.51, p<0.001; Hispanic, β
0=5.2, β
1=–0.47, p<0.001). In contrast, non-Hispanic Black parents from this class had low CES-D scores at baseline but showed no significant change (β
0=5.4, β
1=–0.28, p
=0.403).
The class with midlevel CES-D scores included 24%, 28%, and 22% of non-Hispanic White, non-Hispanic Black, and Hispanic parents, respectively. For Hispanic parents from this class, CES-D scores improved significantly over time (β0=12.8, β1=–0.86, p<0.01). For non-Hispanic White and non-Hispanic Black parents, CES-D scores showed no significant change.
A small proportion of parents fell into the class with clinical-level CES-D scores. Specifically, 5%, 7%, and 6% of non-Hispanic White, non-Hispanic Black, and Hispanic parents, respectively, were in this class. For all parents in this class, regardless of racial and ethnic group, CES-D scores showed no significant change.
Discussion
Parental depression is a pervasive concern, with proximal and distal impacts on children. This concern is heightened for child welfare–involved families characterized by increased levels of depression. We found that depressive symptoms were significantly higher for parents who did not fully participate in home visitation services. Among parents who did participate, a significant portion reported persistent depressive symptoms. Three distinct depressive trajectories emerged and varied by race and ethnicity. Unlike previous studies that showed lower depression for Black individuals in community samples, Black parents in this study reported elevated rates of depressive symptoms and showed no significant improvement while receiving services.
Parental engagement in services is essential for reducing child maltreatment and related outcomes for children served by the child welfare system (
40). We found that 40% of parents did not remain in home visitation services beyond a few weeks. Among those lost to follow-up, baseline depressive symptoms were significantly higher, compared with those who remained in the study. Parents who enter services with elevated levels of depressive symptoms are struggling to maintain service participation—even compulsory services, as is often the case with child welfare involvement. This finding highlights an area ripe for intervention, because addressing parents’ elevated mental health needs may facilitate increased participation in services, with downstream impact on children and families.
Most parents reported low levels of depressive symptoms, which tended to ameliorate over the course of services for White and Hispanic parents but not for Black parents—a pattern which held for Black parents across all CES-D groups. Between 22% and 28% of parents reported above average levels, but below clinical levels, of depressive symptoms. Of parents in this mid-CES-D class, Hispanic parents experienced significant reduction in symptoms during home visitation participation.
In this context, Hispanic families were often Spanish-speaking immigrants from Mexico and received a version of SafeCare culturally adapted to meet the needs of this specific community (
41). In addition to adapting the materials, content, training goals, and program structure, Hispanic families were most often paired with culturally congruent Hispanic and Spanish-speaking providers. Although findings are mixed, meta-analytic research has shown that individuals—particularly individuals of color—generally prefer a therapist of their own race-ethnicity (
42). Although treatment outcomes are mixed with regard to effectiveness, culturally relevant aspects of the service experience are salient for the responses of persons from racial and ethnic minority groups (
43).
It is particularly relevant that depressive symptoms did not improve among Black parents, whose baseline depressive symptoms were highest. While Hispanic families were often paired with culturally congruent providers—potentially contributing to the significant decline in depressive symptoms experienced by these parents—Black families were not afforded the same opportunity. Research has shown that the effects of racial-ethnic matching of therapists and clients on mental health outcomes were strongest for Black clients (
42). Additionally, correlates of race-ethnicity, such as wariness about bias in mental health services, poverty, institutional racism, and vulnerability to trauma, may contribute to seemingly high levels of depressive symptoms, but these factors are not easily amenable to individualized treatment that focuses on syndromal depression. Elevated depression rates among individuals from minority groups are largely associated with greater health burdens and inadequate access to high-quality services, factors amenable to public policy intervention (
44). Because Black families are disproportionately represented in public sector service settings, in particular child welfare services (
18), there is a specific need to address systemic, service, and discriminatory mechanisms that contribute to poorer outcomes.
None of the trajectory classes with the highest levels of depressive symptoms significantly improved over the course of services. In fact, White parents showed an increase in symptoms. Although the high-symptom group represented a small proportion of the overall child welfare–involved sample, it appears that current services are not addressing mental health needs for this group. This is important because parents with serious mental illness have been shown to have more contact with child welfare services (
45); however, the symptoms of these parents are not being mitigated in the current service context, suggesting a continued need for coordination between the child welfare and mental health care systems (
46).
This study presented longitudinal findings regarding depressive symptoms in a large, racially and ethnically diverse sample of child welfare–involved families. We capitalized on multiple time points over the course of active participation in child welfare services to reveal distinct trajectories of depressive symptoms. The study had several limitations. First, we relied on self-reports of depressive symptoms. Parents typically underreport their symptoms (
47). Even if depressive levels in this study were underreported, many families were at risk. Additionally, although the CES-D has been demonstrated to be psychometrically valid among different racial-ethnic groups, it was originally developed with a White population. Future research should continue to challenge understanding of how depressive symptoms are influenced, understood, and reported differently on the basis of cultural orientation.
Another limitation of the study was a lack of complete information regarding other services participants may have been receiving concurrently. Although we may conjecture about the array of services that families were offered or received (i.e., mental health services, housing or economic support, and family preservation services), we were unable to explore other factors that may have explained changes (or lack thereof) in depressive symptoms. Finally, we recognize the presence of within-group heterogeneity, which was unaccounted for in this study. For example, African Americans and Caribbean Black Americans have different ancestral ties, unique histories, and distinctive traditions that may result in different depression prevalence and presentations (
48,
49). Among Hispanic adults, Puerto Ricans have demonstrated higher lifetime and past-year prevalence rates of psychiatric disorders, compared with other Hispanic subgroups. Also, Hispanic individuals born in the United States have been found to be more likely to meet lifetime criteria for psychiatric disorders, compared with Hispanic individuals who immigrated (
46). Further, it is prudent and meaningful to acknowledge the limitation of this study in focusing narrowly on non-Hispanic White, non-Hispanic Black, and Hispanic child welfare–involved parents. Child welfare–involved parents comprising other racial and ethnic groups were excluded from our analyses because of small sample sizes. Future work should attend to these important populations.
Conclusions
The persistence of depression for child welfare–involved parents and the impact on children cannot be understated. Despite receipt of supportive, recovery-oriented services focused on empowering child welfare–involved parents, many experienced elevated depressive symptoms through the duration of participation in SafeCare—symptoms that have been shown to have a negative impact on children. Health and mental health service systems should consider an improved approach to addressing the mental health needs of this vulnerable population. Child welfare–involved parents with significant symptoms of depression may benefit from assistance in accessing mental health treatment. Treatment approaches such as stepped care that integrates with child welfare programming may improve both engagement and mental health among families.