The comorbidity of mental disorders and general health conditions has long been documented (
1), as has evidence suggesting that general medical and psychological symptoms increase together (
2). The COVID-19 pandemic has brought new attention to these associations because COVID-19 has been associated with psychiatric symptoms. Studies have begun to document linkages between COVID-19 diagnosis and symptoms of depression (
3) and anxiety disorder (
4). These findings are particularly concerning for patients experiencing low incomes. Previous studies have reported worse mental health outcomes among persons with lower socioeconomic status (
5); in addition, low levels of household income have been shown to increase the risk for incident mood, anxiety, and substance use disorders as well as suicide attempts (
6).
In the United States, federally funded community health centers (CHCs) work to improve access to primary health services and combat health disparities experienced by persons living in lower-income communities and served >29 million patients in 2020 (
7,
8). In recent years, CHCs have been granted additional funding to improve their behavioral health treatment capacity and to integrate mental health services into primary medical care settings (
9). However, similar to most sectors of the U.S. health care system, CHCs have faced unprecedented challenges to their care delivery caused by the COVID-19 pandemic. One key knowledge gap in the scholarly literature is that little is known about how COVID-19 disrupted the receipt of necessary mental health services among CHC patients. Although continuity of care was likely disrupted for a range of services, it is important to understand whether depression care for CHC populations was disrupted; these populations typically comprise racial-ethnic minority patients living below the poverty level (
10) who have been historically affected by disparities in access to mental health care.
The objective of this study was to examine associations between COVID-19 prevalence at CHCs and the percentage of eligible CHC patients who had ongoing depression care documented in 2020. This study builds on earlier investigations examining how COVID-19 may have disrupted care delivery in other care settings. The findings of this report yield generalizable insights about depression care for medically underserved patient populations receiving care in the CHC safety-net system.
Methods
This cross-sectional study used data from the 2020 Uniform Data System (UDS; calendar year from January 1 to December 31), obtained in August 2021 from the Health Resources and Services Administration (HRSA). HRSA collects the UDS data annually on CHCs’ patient characteristics, service utilization, and organizational features. Beginning in 2020, HRSA collected new data on testing and diagnosis of the COVID-19–causing agent, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). For purposes described below, data from the
New York Times COVID-19 data repository (
https://github.com/nytimes/covid-19-data) were also merged into the analytic file.
The CHC was the unit of analysis, and the final analytic sample included 1,113 CHCs in the 50 U.S. states and Washington, D.C., in 2020, representing about 26,865,015 total patients and 8,617,296 patients screened and potentially eligible for follow-up depression care. This study was deemed exempt from institutional review board review.
Multivariable linear regression models were estimated to examine associations between COVID-19 prevalence and the percentage of patients who screened positive for depression and who had follow-up depression care documented in 2020. To correct for heteroskedasticity in the error terms, Huber-White standard errors were used; in addition, the models were weighted by size of each CHC’s patient population diagnosed as having a mental health condition. For ease of interpreting the regression model coefficients, predicted (i.e., regression-adjusted) outcome values were calculated for different levels of COVID-19 prevalence within a CHC’s patient population by using average marginal effects. All analyses were conducted with Stata MP, version 17.1.
The main explanatory variable measured the percentage of each CHC’s patient population diagnosed as having COVID-19 infection (
ICD-10 code U07.1) by the end of 2020. As a robustness test, the regression model was reestimated by examining an alternative explanatory variable that measured the percentage of each CHC’s patient population tested for SARS-CoV-2 in 2020. The dependent variable was the National Quality Forum’s metric 0418, aggregated at the CHC level to report how many CHC patients eligible for depression care had follow-up care documented in a year. Specifically, the variable measured the percentage of CHC patients ages ≥12 years screened for depression with an age-appropriate standardized depression screening tool and, if screening was positive, who established a follow-up care plan in 2020 (
11). An example of follow-up care is additional services with a practitioner who is qualified to treat patients with depression or provide pharmacological intervention for depression treatment.
The statistical models also included a vector of covariates to absorb residual variance in the outcomes or to adjust for potential confounding factors between CHCs. UDS data were used to adjust for CHC-level patient factors, including the gender, race-ethnicity, and income characteristics of each CHC’s patient population. The percentages of patients with obesity diagnoses were included to account for health status differences among CHC patient populations. Measures of total patient population size and supplemental COVID-19 support funding (e.g., through the Coronavirus Aid, Relief, and Economic Security [CARES] Act) were included to adjust for differences in organizational size and COVID-19 testing capacity. State-level data from the New York Times database on the prevalence of COVID-19 cases by the end of 2020 were included to adjust for differences in COVID-19 severity among states.
Results
A table showing the results of the multivariable regression analysis is available in an
online supplement to this report. On average, each increase of 1 percentage point in COVID-19 prevalence within a CHC patient population was independently associated with a 0.47-percentage point decrease of eligible patients with a follow-up depression care plan documented in 2020 (p=0.039). The results of the robustness test using the alternative explanatory variable were consistent with the main model findings. A negative association was found between the percentage of each CHC’s patient population tested for SARS-CoV-2 and the outcome variable (p=0.047).
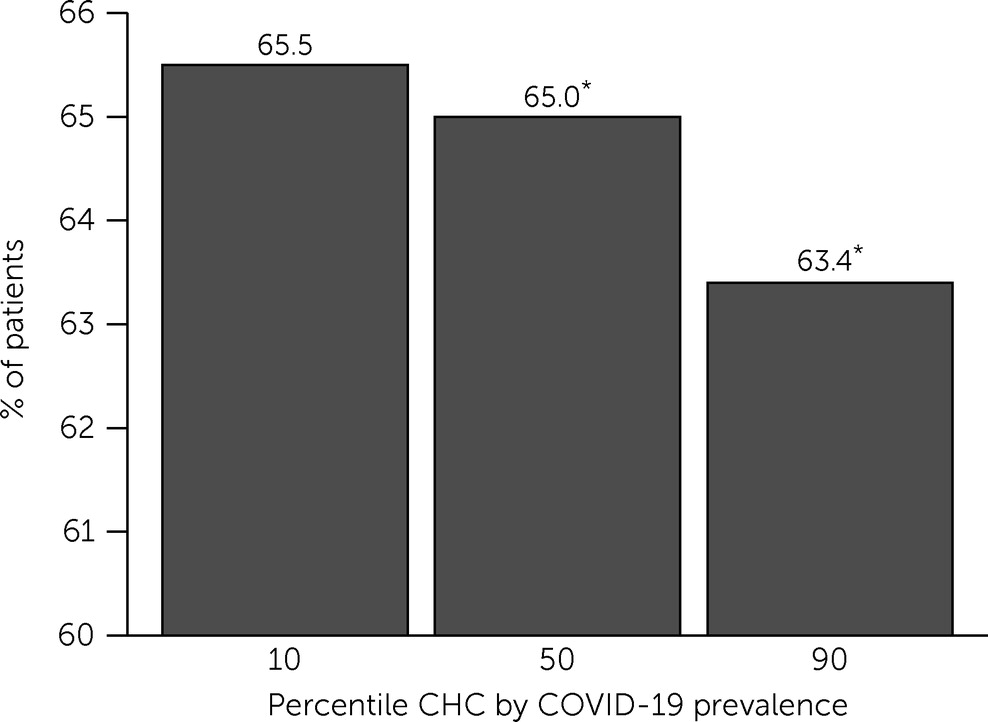
Figure 1 presents the main regression model findings. The estimated percentages given below are regression-adjusted, predicted percentages generated for an average CHC case. On average, at CHCs in the 90th percentile (based on the percentage of their patients’ diagnoses with COVID-19, i.e., many patients), 63.4% of eligible patients were predicted to have a follow-up depression care plan documented in 2020. In comparison, at CHCs in the 10th percentile (i.e., many fewer patients with COVID-19), 65.5% of eligible patients were predicted to have follow-up depression care documented in 2020 (p=0.039).
Discussion
The key finding in this report suggests that CHC patient populations experiencing greater COVID-19 prevalence in 2020 had statistically significantly less follow-up depression care documented among eligible patients, although the differences in follow-up care among populations were modest. Although not based on a causal analysis, these findings may reflect the influence of isolation policies or patient avoidance of care due to COVID-19 within local patient populations. From the patient perspective, greater rates of COVID-19 diagnosis within a CHC patient population may have caused greater hesitation to seek or return for depression care regardless of one’s risk for COVID-19 exposure. Patients exposed to COVID-19 would likely have been required to isolate or otherwise postpone care.
Another explanation for these findings could perhaps be that, at the organizational level, greater COVID-19 prevalence may have more frequently halted or delayed the availability of mental health services because of quarantine restrictions among staff and appointment cancelations. The percentage of eligible patients with a documented follow-up depression care plan was down across all CHCs on average from about 70.5% in 2019, the year preceding the pandemic (data not shown).
These findings have important implications. The results are consistent with recent studies showing that COVID-19 may have negative consequences for patients diagnosed as having depression (
3) or anxiety disorder (
4). Indications that greater COVID-19 prevalence may disrupt the ongoing delivery of mental health care for CHC patients is concerning given past evidence connecting low socioeconomic status with greater risk for depression and anxiety. Perhaps more concerning is the fact that most CHC patients belong to racial-ethnic minority groups. Racial-ethnic minority patient populations may have been predisposed to worse consequences from COVID-19 facilitated through long-standing inequalities, including greater risks of experiencing negative health outcomes resulting from COVID-19 (
12) and barriers to secondary care (
13,
14).
This study had important limitations. First, it used a cross-sectional design. The relationships explored in this study were not causal. However, this investigation is one of the first of its kind to analyze new measures created by HRSA to better understand in a generalizable way how CHCs and their patient populations experience COVID-19.
Second, UDS data were reported at the CHC grantee level. Therefore, this investigation was focused on patient populations, and individual patient outcomes and risks could not be examined. Third, this study could examine only process-of-care outcomes for depression screening and follow-up care among CHCs at the grantee level. No other mental health–related process or care measure was collected and reported by HRSA for all CHC grantees. Fourth, the pandemic disrupted care delivery in various health care settings and shifted many in-person appointments to virtual visits. The UDS does not currently report telehealth appointment data. However, given the unprecedented disruptions experienced by care providers, it is likely that some follow-up depression care appointments were delivered via telemedicine but not appropriately documented in the UDS.
Fifth, although this study analyzed the most recent UDS data, these data predated the availability of COVID-19 vaccines to the public. CHC vaccination rates may have mitigated the effect that COVID-19 had on mental health care continuity, assuming adequate vaccine availability and uptake among CHC patients. CHC vaccination rates will be available in UDS data to be released in 2022. Until then, further investigation is needed through smaller-scale studies to explore the protective effects of the COVID-19 vaccine on health care use among CHC patients. Finally, it is also important to note that UDS data are compiled and submitted to HRSA by human agents, often drawn from electronic health record (EHR) systems. Human agents working with EHR systems in high-pressure situations could make errors in data entry and reporting. There is no reason to suspect that any unobserved, systematic human error biased the estimates provided in this report. However, human data reporting necessitates mentioning this concern.
Conclusions
The findings from this study examining follow-up depression care among CHC patient populations with differing COVID-19 prevalence appear to be consistent with recent studies reporting that increased COVID-19 prevalence is associated with poorer mental health outcomes in other care settings. In response to the pandemic, the federal government legislated CARES Act funding to help CHCs address challenges associated with COVID-19 (
15) and to provide services to patient populations with low incomes. Notable provisions included $1.32 billion in supplemental funding for 2020 as well as a short-term funding fix for the Community Health Center Fund (
15). However, additional federal support will likely be needed to stem the comorbid health risks caused by the pandemic, especially given the history of mental health disparities experienced by low-income patients.
To that end, the National Association of Community Health Centers has developed resources for CHCs to more effectively respond to COVID-19 as well as advocacy tools for encouraging policy makers to maintain adequate CHC funding. Clinicians and professional associations, such as the American Psychiatric Association, wield considerable advocacy power. As a result, they can effectively communicate important public policy matters (
16) to state and federal legislators in support of CHCs receiving adequate financial support during the pandemic.