Study participants
The subjects were referred by child welfare workers to the parenting assessment team at the University of Illinois at Chicago between January 1996 and April 1999. All parents who were referred had lost custody of a child as a result of confirmed abuse, neglect, or risk of harm. They were referred for an assessment to determine their current ability to safely parent their child. They had been hospitalized at least once for a
DSM-IV (
20) psychiatric illness other than substance abuse or dependence and thus struggled with a different level of mental illness than persons who had never been hospitalized.
Of the 118 families who were evaluated by the parenting assessment team, 44 mother-child dyads met the following inclusion criteria for our study: the parent was a woman at least 20 years old, the index child was between eight months and four years of age, and there had been at least weekly contact between the mother and the index child during the one-year period preceding the study. Mothers who met DSM-IV criteria for mental retardation and those who spoke neither English nor Spanish were excluded from the study.
The inclusion criteria were selected to provide a relatively homogeneous population for study. Mothers may have somewhat different parenting issues than fathers, teenage parents may have different issues than older parents, and parenting young children calls for a different set of skills than parenting older children. The population chosen for our study reflects the current priorities of the child welfare system (
21). The requirement for at least weekly visits was included to ensure enough parent-child contact for an ongoing parental relationship to have been maintained despite the mother's loss of custody. The study was approved by the institutional review board, and all subjects gave written informed consent to participate.
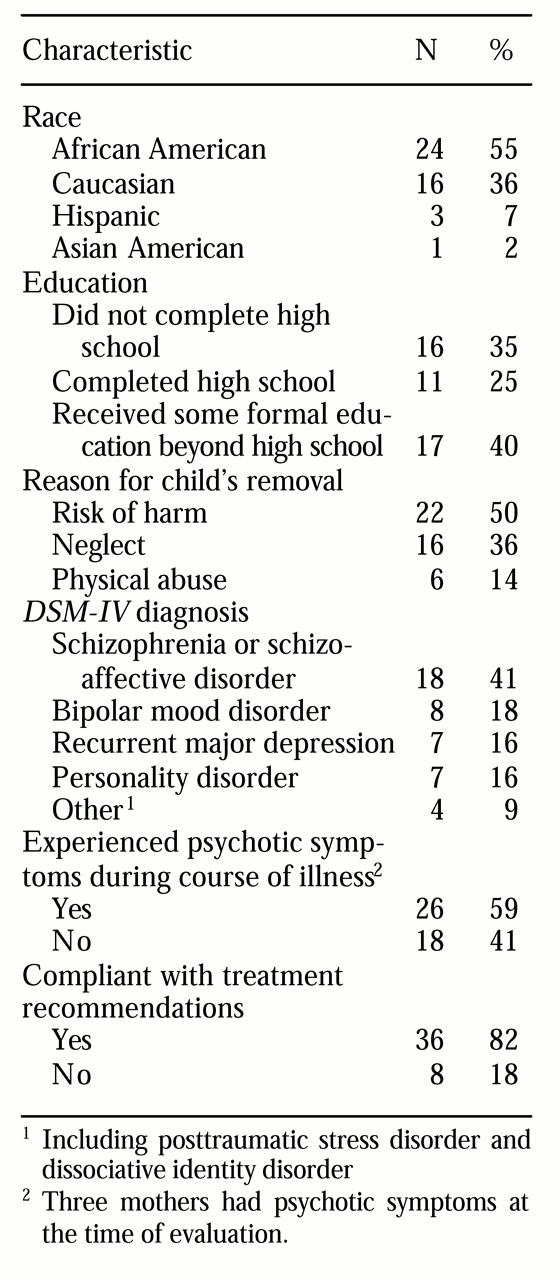
Of the 44 participating index children, half were less than two years old and half were two to four years old; half were male and half female. The mean±SD age of the 44 participating mothers was 32.4±6.3 years, with a range of 20 to 45 years. Additional information about the mothers is provided in
Table 1.
Instruments
Measure of insight. Among the tools available to assess insight, the one chosen as optimal for this study was a modified version of the Schedule for Assessment of Insight (
23). This scale approaches insight as a multidimensional phenomenon (
18). It has been used as a measure of insight in various studies (
24), and it is short enough to be practical for use as part of a battery of assessment tools. We modified the scale for use not only with patients with psychotic disorders, as was its original intent, but also for use with other persons with major mental illness. The modified instrument may be obtained from the authors.
In the study reported here, a psychiatrist with prior training in the use of the insight scale independently rated the 44 psychiatric interviews with the mothers. The psychiatrist subsequently completed a written psychiatric evaluation based on the interview and on available records of past evaluations, hospitalizations, and treatment. The written report contained no information about insight into mental illness. A second independent psychiatrist who also had prior training in using the scale rated 20 randomly selected written psychiatric evaluations. The raters had not participated in administering the study tools, and they were fully blinded with regard to each other's ratings and with regard to findings on all study variables. The intraclass correlation statistic, a measure to estimate interrater reliability, was 95.
Measures of parenting risk. The most direct way to determine whether a mother is at risk of further maltreating a child whom she has maltreated in the past would be to have her resume custody of the child and see what happens. However, this option would not be ethically justified, so researchers use less direct but still very useful measures of parenting risk. One effective measure chosen for this study was a direct, systematic observation of maternal behavior. The second measure was a comprehensive multidisciplinary clinical estimation of risk.
We used the Crittenden Care Index (
12) as a measure of mother-child interaction quality. This index was specifically developed for use with maltreating families and is appropriate for mothers with children up to four years old. It has been used with families from high-risk backgrounds and different social classes. Index ratings have been found to be highly correlated with mother-child attachment quality, child interactive behavior, and childrearing status—for example, abusing, neglecting, or adequate (
12). The index has high interrater reliability among trained raters (kappa=.83 to 90).
The index is obtained by scoring a videotape of a mother-child interaction in a standard observation. The mother and child are asked to play as they usually do at home. The two sit facing each other, with a basket of age-appropriate toys nearby. Their interaction is videotaped for three minutes. The index focuses on seven aspects of parental behavior: facial expression, vocal expression, position and body contact, expression of affection, pacing control, and choice of activity. Each aspect of maternal behavior is scored as insensitive, 0; partially sensitive, 1; or sensitive, 2. The scored items for each aspect of behavior are summed to yield an overall score ranging from 0 to14. A score of 6 or less is considered to be indicative of at-risk parenting.
In our study, the Crittenden Care Index was administered as part of a comprehensive evaluation of parenting competency. It was therefore necessary to ensure that the observational ratings were independent of the clinical estimation of maltreatment risk. To this end, two clinical psychologists who were trained in the use of the index scored all 44 tapes. The raters had not participated in administering any study tools or in making the comprehensive clinical ratings of maltreatment risk (described below). They also had no knowledge of each other's ratings or of any of the study's variables or findings. The interclass correlation between the two raters on the maternal sensitivity scale was .73.
Clinical risk for child maltreatment. A parenting assessment team—a psychiatrist, a psychologist, and a social worker—conducted standardized clinical assessments to estimate the likelihood that a particular mother would abuse or grossly neglect the index child if she were currently the child's primary caregiver. The assessment of each dyad included:
• Clinical interviews, including unstructured and semistructured interviews of the mother and child separately from one another
• Interviews with collateral historians
• Review of records, including psychiatric records, relevant medical records, child welfare agency records, and school reports
• Evaluation of the home setting using a modified Home Observation for the Measurement of the Environment inventory (
25)
• Evaluation of parental expectations of the child using the Parent Opinion Questionnaire (
11)
• Evaluation of maternal behavior and mother-child attachment quality in the home and in a standard clinical observation (
12)
• Evaluation of the effects of the mother's childhood trauma using the Childhood Trauma Interview (
26)
• Evaluation of current parenting stressors and mothers' ability to identify and acknowledge stressors using the Parental Stress Inventory (
27)
• Evaluation of the mother's current social support for parenting using a modified version of the Arizona Social Support Inventory (
29)
• An assessment of the mother's internal representation of her children (
29)
• A criminal background check
All the data were gathered and scrutinized according to guidelines described in the Parenting Assessment Team Manual (
30) and summarized in a prior publication (
31), which also discusses the rationale for the choice of assessment methodology. The assessment team reviewed the data for each case and considered risk factors in relation to protective factors and potential for change. The team then decided by consensus to assign the respondent to a higher or lower risk category for maltreatment. A higher-risk assignment meant that even if the mother was offered interventions, the prognosis for adequate parenting capability in a reasonable time frame was poor. A lower-risk assignment meant that if specific interventions were offered and accepted, there was a reasonable likelihood that the mother could successfully become an effective primary caregiver for her child. The procedure used to make a consensus decision in assigning these categories is comparable to the best-estimate technique (
32), which has been used to make
DSM-IV axis I and axis II diagnoses and has been shown to have high test-retest reliability.