With the rapid increase in the rate of incarceration among women, the psychiatric disorders and physical health problems in this population have become significant public health challenges (
1). The number of women prisoners doubled between 1986 and 1997, whereas the number of male prisoners increased by two-thirds (
2) By 1997, women prisoners accounted for more than 6 percent of the 1.8 million inmates held in U.S. prisons or jails (
2). This explosion in the number of incarcerated women has been attributed primarily to illicit drug use and drug-related crimes (
1,
3).
Rates of human immunodeficiency virus (HIV) infection are also soaring among women prisoners. In national surveys of prison inmates, the prevalence of HIV infection among incarcerated women ranged from 2.5 percent to 20 percent (
4,
5), which greatly exceeds the rate of .15 percent among women in the general population (
6). Furthermore, rates of HIV infection among women prisoners are often three times those of male prisoners (
4), whereas in community samples, HIV-infected men have nearly three times the infection rate of women (
6).
Despite the high HIV seroprevalence among women prisoners, only a few studies have examined the behaviors that place these women at high risk of HIV infection (
7,
8,
9). Major HIV risk factors for prisoners of both sexes are injection drug use and needle sharing (
4,
5,
8,
9). Although the rates of injection drug use are higher among men in the general population (
10), female prisoners are more likely than male prisoners to have been drug injectors before incarceration (
4,
9). Female prisoners are also more likely than their male counterparts to have had sex partners who were injection drug users or to have engaged in prostitution (
11).
In addition to addictive disorders, other psychiatric disorders may contribute to HIV risk behaviors. Posttraumatic stress disorder (PTSD) has received little research attention in this context, even though it has been associated with depression (
12,
13) and cocaine or opiate abuse (
13,
14), both of which have been reported to be risk factors for HIV infection (
15). Symptoms of PTSD have been associated with prostitution and injection drug use in young adults (
16). Among female drug users, violent trauma and other predisposing factors for PTSD are widespread (
17). HIV-infected adults who have a history of childhood sexual or physical abuse have reported engaging in more HIV risk behaviors such as drug abuse and sexual compulsivity than persons with no history of trauma (
18,
19).
Previous studies have usually focused on the association between HIV risk behavior and either trauma or symptoms of posttraumatic stress rather than on the full disorder, which is a more devastating response to trauma. Because PTSD has been associated with an elevated risk of HIV infection (
20), such an exploration appears especially warranted.
In previous studies, PTSD has been found to affect about one-third of incarcerated women, and it was found to be the second most prevalent psychiatric disorder—after substance abuse—in this population. Teplin and colleagues (
21) found that among 1,272 women jail detainees, 22 percent met the criteria for current PTSD, and 34 percent met the criteria for lifetime PTSD. In a study by Jordan and colleagues (
22), 30 percent of 805 convicted women prisoners reported exposure to trauma and having symptoms of PTSD in the six months before incarceration. Zlotnick (
23) has reported even higher rates of PTSD among women prisoners, although these results may be associated with differences in sample size and methodology. The association between PTSD and HIV risk behavior among women prisoners has not been explored. Establishing the prevalence of PTSD in women prisoners and its contribution to HIV risk behaviors would be important in mental health treatment planning and HIV risk reduction for this population.
Lyketsos and Federman (
15) found an association between depression and HIV risk behaviors. In nonprisoner samples, elevated rates of a lifetime history of major depression have been reported by HIV-infected and noninfected individuals who engaged in HIV risk behaviors (
24,
25,
26). The contribution of depression to HIV risk behaviors is underscored among women prisoners, in whom the prevalence of depression exceeded rates reported by men both in prison and in community samples (
22).
To our knowledge, no published study has examined the relationship between psychiatric disorders and HIV risk behaviors among women prisoners. For this study, we hypothesized that HIV risk behaviors in this population would be high, considering the high rates of HIV infection reported for women prisoners. We also hypothesized that rates of psychiatric disorders would be high and that these disorders could have contributed to high rates of HIV risk behaviors. Specifically, we predicted that PTSD, major depression, and dysthymic disorder would be linked to sex and drug risk behaviors associated with HIV transmission.
Methods
Participants
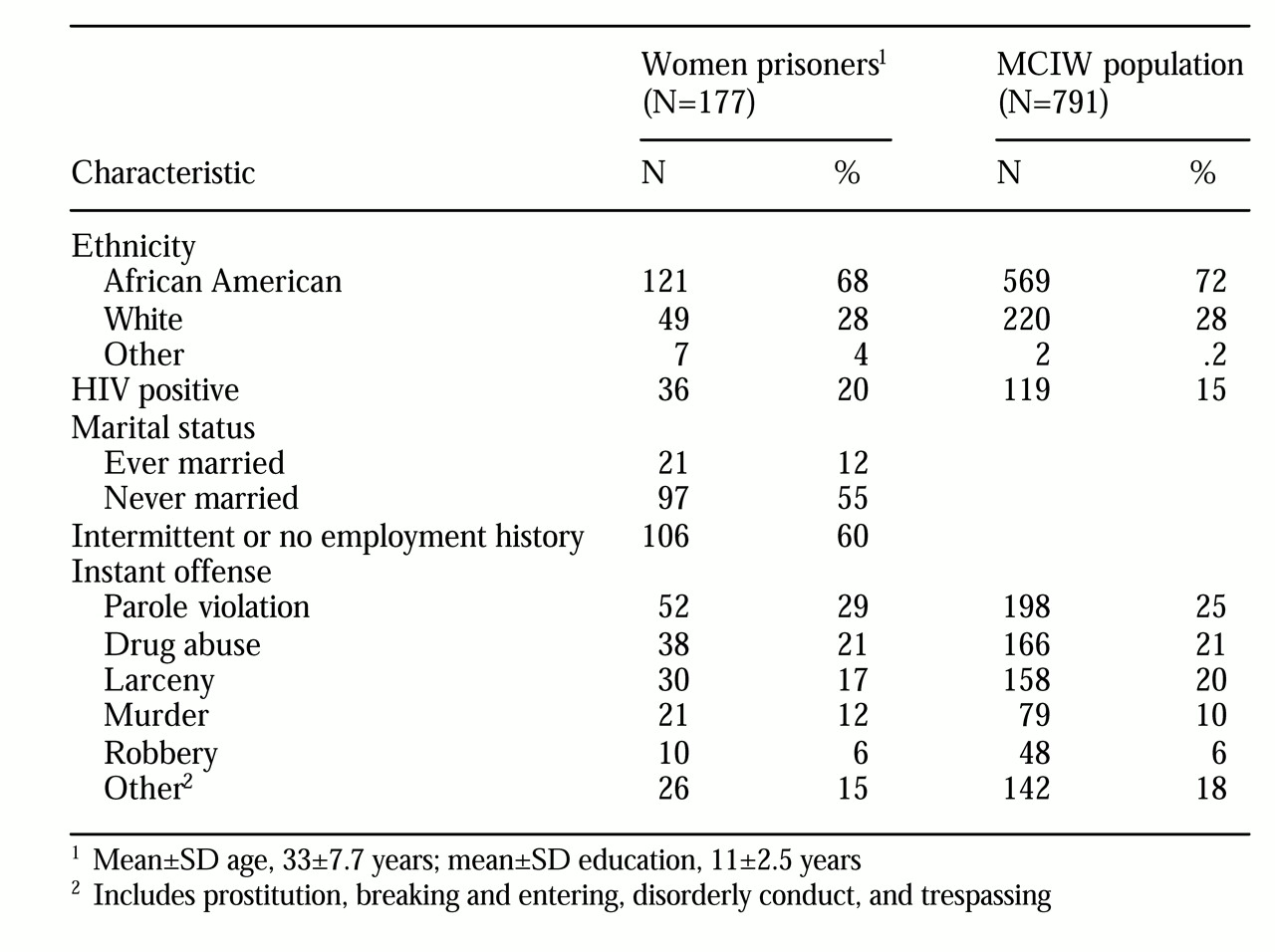
The study sample consisted of 177 women prisoners at the Maryland Correctional Institution for Women (MCIW), an 800-bed minimum- to maximum-security prison that houses the majority of female prisoners in the Maryland state correctional system. Participants were recruited through a prisonwide advertisement for volunteers to take part in a study of "issues of women in prison." To reduce selection bias, the advertisement did not mention the psychiatric or HIV nature of the study. No incentives were provided for participation. Participants were included in the study if they had been incarcerated for less than one year. An additional 15 HIV-infected women were recruited from the prison HIV clinic. Secondary analyses excluding these additional participants indicated that their absence did not have a statistically significant impact on the study findings. Participants were offered a separate feedback session on the results of their evaluation. At the conclusion of the study, participants were apprised of the purpose of the study and offered a summary of the results.
Table 1 presents the demographic characteristics of the study sample and of the entire MCIW population during the study period, from 1995 to 1997. The sample was representative of the MCIW population. The participants gave written, informed consent. The institutional review board of the Johns Hopkins University, which included a prisoner advocate, and the human subjects committee of the Maryland Department of Correction approved the study. The all-inmate advisory council at MCIW also approved the study.
Measures
We adapted scale items from the Risk Behavior Assessment (
27), a structured interview developed by the National Institute on Drug Abuse that examines drug-related and sexual HIV risk behaviors, to assess the participants' risk behaviors in the five years before their incarceration. Retrospective reporting on drug use and sexual behavior has been shown to yield reliable information (
28,
29); however, socially undesirable behavior is generally underreported (
30).
Eight dichotomous high-risk behaviors were examined: used or did not use intravenous drugs; had or did not have a sex partner who was an injection drug user; shared or did not share needles or drug paraphernalia; engaged or did not engage in anal intercourse; often or always, or never or rarely, had sexual intercourse when intoxicated or high on drugs; never or rarely, or often or always, used condoms; engaged or did not engage in prostitution; and had 100 or more, or fewer than 100, sex partners. The absolute number of sex partners participants had, a continuous variable, was also examined.
The Structured Clinical Interview for DSM-IV, Non-patient Edition (SCID) (
31), was used to assess participants for axis I psychiatric disorders, including substance use. Lifetime—that is, ever meeting diagnostic criteria—and current psychiatric diagnoses were determined for major depression, dysthymic disorder, heroin or cocaine dependence, and PTSD. After the PTSD module had been administered, participants who indicated that they had experienced a traumatic event were asked to identify the event. Traumatic events were subsequently categorized as sexual assault before age 16, excluding rape; adult sexual assault, excluding rape; rape before age 16; rape after age 16; physical assault before age 16; physical assault after age 16; witness to physical or sexual assault; fire; and other events—for example, motor vehicle accident. This approach is consistent with that used in published studies (
32,
33).
Two psychologists and a social worker reviewed the SCIDs. All three had received prescribed training (
34), which included reviewing and scoring videotaped SCID interviews as well as observing or scoring interviews by SCID-trained psychiatrists or other mental health professionals to verify adequate interrater reliability. The reviewers were blind to the participant's HIV status and HIV risk behaviors.
HIV testing
HIV serologic testing was performed for all participants, and, in accordance with prison policy, all participants received pre- and posttest counseling.
Statistical analysis
Data were analyzed with SPSS software (
35). Chi square tests were used to compare distributions of categorical variables, such as risk behaviors, and t tests were used to compare distributions of continuous data. Logistic regression was used to investigate the association between psychiatric diagnosis—the independent variable—and each high-risk behavior category—the dependent variable. The resultant odds ratios were adjusted for age, race (white or not white), HIV status, and years of education. Given the association of addiction with HIV risk behaviors (
8,
9,
10,
11), odds ratios were also adjusted for a SCID-derived psychiatric disorder of heroin or cocaine dependence. Linear regression was used to investigate the association of psychiatric diagnoses with number of sex partners.
Results
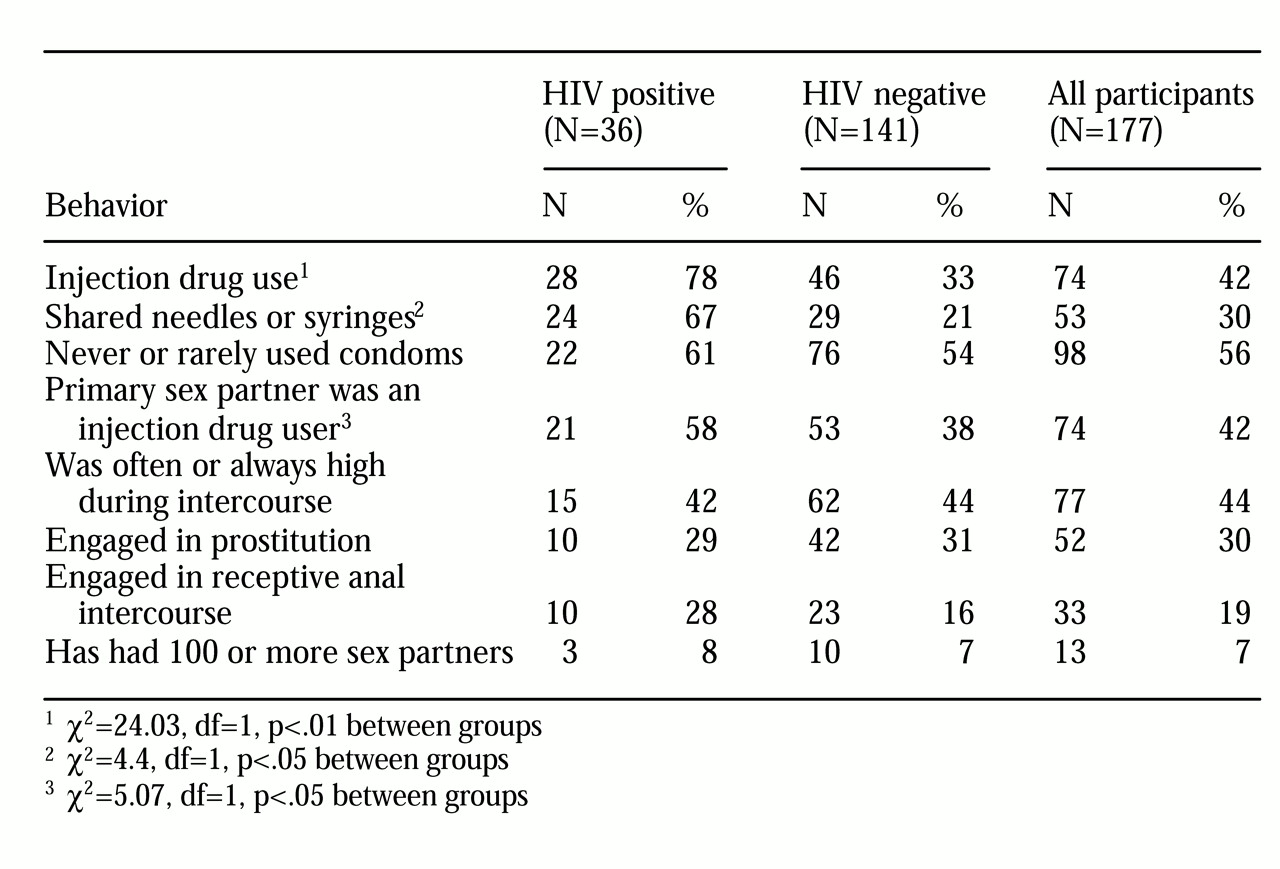
Specific HIV risk behaviors are summarized in
Table 2. Both HIV-positive and HIV-negative participants reported several types of sexual behavior that would have placed them at risk of HIV infection—for example, never or rarely using condoms, engaging in anal intercourse, or engaging in prostitution. Crack cocaine was the drug most frequently exchanged for sex. The women's drug use behavior, such as use of injection drugs or sharing of needles and syringes, also placed them at significant risk of HIV infection.
HIV-positive and HIV-negative participants differed significantly in having a history of having injected drugs (χ2=24.03, df=1, p<.001), having a sex partner who was an injection drug user (χ2=5.07, df=1, p<.03), exclusively having sex partners who were injection drug users (χ2=9.6, df=1, p<.002), and sharing of drug paraphernalia (χ2=4.40, df=1, p<.04). These behaviors are those most likely to transmit the HIV virus. The total number of HIV risk behaviors was high among all participants, but it was significantly higher among HIV-infected participants than among noninfected participants (mean±SD= 4.69±1.43 and 3.48±1.52; F=17.99, df=1,175, p<.001).
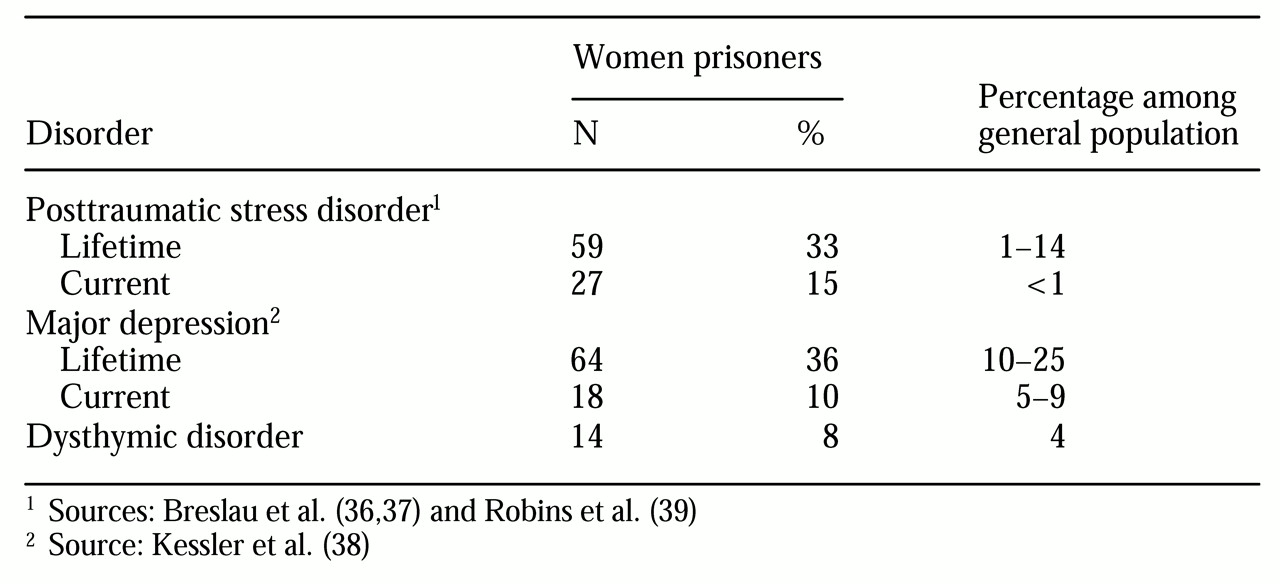
The participants' psychiatric diagnoses are summarized in
Table 3. Their frequencies of current and lifetime diagnoses were well above general population estimates for women for PTSD (
36,
37,
38), major depression, and dysthymic disorder (
39).
The association between the diagnosis of a psychiatric disorder and specific high-risk behaviors was examined in logistic regression models. Compared with participants who did not have PTSD, participants who met criteria for a lifetime diagnosis of this disorder were 71 percent more likely than those who were not diagnosed with PTSD to have engaged in anal sex and 56 percent more likely to have engaged in prostitution (Wald statistic=5.75, df=1, p<.02; and Wald statistic=4.5, df=1, p<.04). The association between lifetime PTSD and other HIV risk behaviors was not significant.
After the analysis adjusted for age, race, HIV status, education, and heroin or cocaine dependence, the association between lifetime PTSD and the practice of anal sex or prostitution remained significant (for anal sex, odds ratio=1.7, 95 percent confidence interval=1.26 to 2.16; Wald statistic=5.5, df=1, p<.02; and for prostitution, OR=1.56; 95% CI=1.17 to 1.95; Wald statistic=4.8, df=1, p<.03). HIV risk behaviors were associated with a current diagnosis of PTSD, but the association was not significant.
In logistic regression models, no significant associations were found between traumatic life events and HIV risk behaviors, either when considered alone or when adjusted for the presence of PTSD. No significant associations were found between any of the reported high-risk behaviors and major depression or dysthymic disorder.
Discussion
The prevalence of HIV infection among women prisoners has been found to be as high as three times the rate among male prisoners (
4). The participants in our study reported high rates of risky sex and drug use behaviors during the five years before incarceration. Rates of PTSD, depression, and dysthymic disorder among these women were also high. Furthermore, participants with a lifetime diagnosis of PTSD were more likely than others to have engaged in prostitution and receptive anal sex.
Nearly half of the women in our study used injection drugs during the five years before incarceration, and most of them shared needles or syringes, primarily with their significant other. The majority of women never or rarely used condoms, and nearly half reported having sexual intercourse with partners who used injection drugs. Prostitution for money or drugs, primarily cocaine, was a frequently reported behavior. Not surprisingly, prior high-risk behaviors were more prevalent among the participants who tested positive for HIV infection. As other studies have shown (
8,
9), we found that injection drug use, needle sharing, and sexual intercourse with partners who used injection drugs were associated with HIV infection. These similar findings support the validity of the methods we used to ascertain risk behavior.
The rate of PTSD among the women in our study was also high, significantly exceeding the rate in the general population. Fifty-eight participants (33 percent) met
DSM-IV criteria for a lifetime PTSD diagnosis, and 27 (15 percent) met criteria for a current PTSD diagnosis. These rates correspond with those reported by two large-scale studies of incarcerated women that indicated that PTSD was the most prevalent psychiatric disorder among women prisoners, excluding substance abuse (
21,
22).
Our study also indicates that PTSD is associated with HIV sexual risk behavior. Participants who had a lifetime history of PTSD were more likely to have engaged in prostitution and receptive anal sex in the five years before incarceration than those who did not have PTSD. A causal relationship between PTSD and HIV risk behavior cannot be identified by the methods used in this study; however, prostitution may increase exposure to trauma and thus the likelihood of developing PTSD (
17,
40). Alternatively, PTSD that stems from early sexual abuse may predispose a woman to engage in sexual behaviors that can be destructive, such as prostitution or receptive anal sex (
41). Clarification of the contribution of trauma and PTSD to HIV risk will facilitate prevention and treatment efforts.
Our results indicate that the trauma of being raped before age 16 was the most frequently reported antecedent to PTSD among the women prisoners. Rape has been cited as the event most likely to produce PTSD in the general population (
39,
42), particularly if it occurs before or during adolescence (
42).
Interestingly, exposure to trauma alone was not found to be associated with HIV risk behavior in our study. Other studies have found an association between trauma or posttraumatic stress symptoms and HIV risk behavior (
16,
17,
18,
19); however, none examined PTSD and trauma, so it is not known whether PTSD would have been a better predictor of HIV risk behavior in those studies.
Identification of PTSD among women prisoners is crucial because of its high prevalence. Effective psychological and pharmacological interventions are available to treat the disorder (
43). Treatment planning will be facilitated by more accurate estimates of PTSD, such as diagnostic evaluations of consecutive prison admissions, as opposed to the random sampling used in this study and elsewhere (
23).
Women who engage in drug-related and sexual HIV risk behaviors should be routinely evaluated for PTSD. Instruments such as the Trauma History Questionnaire and the PTSD Checklist (
44,
45) have improved detection rates of the disorder. Undetected, PTSD may present a barrier to reducing HIV risk. Comorbid PTSD and substance abuse have been associated with poorer compliance with drug treatment (
46) and quicker relapse (
47) than substance abuse alone. Untreated PTSD may present a similar obstacle to reduction of sexual risk behaviors (
16).
The failure to detect a relationship between major depression or dysthymic disorder and high-risk behaviors was unexpected. Possibly, the high rates of these disorders in this prison sample attenuated the ability to detect a small association with HIV risk behaviors. Alternatively, the relationship between mood disorders and HIV risk behaviors reported elsewhere (
15) may be mediated in women by PTSD (
37). There is also evidence that rates of depression among HIV-infected women may not be as high as rates reported for HIV-infected men (
48).
The findings of this study have two potential limitations. First, participants were volunteers from the general prison population. Because the population was not systematically sampled, the reported frequencies of HIV risk behaviors and of associated psychiatric disorders may not reflect actual prevalence.
The second potential limitation is that our estimates of HIV risk behaviors relied on retrospective self-report, although participation in the study had no positive or negative effect on incarceration time, so the women had no motivation for responding untruthfully. The high prevalence of drug use, particularly during risk behaviors, may have resulted in inaccurate reporting (
49). Bias in self-reports appears to be in the direction of underreporting past occurrences of behavior and psychopathology (
30,
50), suggesting that our findings may underestimate the actual frequency of HIV risk behaviors. The prison setting necessarily limits sources of information to retrospective self-report, although prisons can provide a unique opportunity to examine an otherwise elusive group.
Conclusions
This study demonstrated that HIV risk behaviors were highly prevalent among women prisoners before incarceration. Rates of current and lifetime PTSD, major depression, and dysthymic disorder were also high. A lifetime history of PTSD was associated with prostitution and receptive anal sex and may have contributed to the high rates of risky sexual behaviors. Targeted HIV risk reduction efforts among women should include evaluation for PTSD; furthermore, women diagnosed with PTSD should be evaluated for HIV sexual risk behaviors.
Acknowledgments
This study was supported by grant MCRR-OPD-GCRC-5MO1RROO722 to Dr. Lyketsos from the Johns Hopkins General Clinical Research Center, National Institutes of Health. The authors thank Joseph Coresh, M.D., Ph.D., for his statistical consultation and Gail Bendit, B.A., Robert B. Harrison, M.S., and Pamela Norbeck, L.C.S.W., for their technical assistance.