Substance abuse is a potent risk factor for poor outcomes in schizophrenia and other serious mental illnesses (
1,
2,
3,
4,
5). Some surveys and drug treatment outcome studies continue to rely solely on self-report measures of illicit drug use, despite problems with reliability and validity (
6). In one epidemiologic survey, lifetime self-reported illicit substance abuse was estimated at 44.8 percent among persons with schizophrenia spectrum disorders (
7). In a recent clinical sample of involuntarily committed severely mentally ill patients, illicit drug use was found to be 34 percent in the four months before hospital admission (
8). Measurement of drug use can be much improved by multi-informant reporting and concurrent use of biological measures of detection, such as urine drug analysis and a relatively new measure, radioimmunoassay of hair (
6,
9,
10,
11,
12,
13). Urine drug testing, although it is reliable and valid and is a more sensitive indication of recent use, has a narrow window of detection, usually about 24 hours. In contrast, radioimmunoassay of hair can be used to detect exposure from two to three days after the most recent use to an indefinite period after use, depending on length of the hair sample. Given typical hair growth of .5 inch a month, 90-day detection (1.5 inches) has been shown to be a reliable and valid method of detecting the use of amphetamines, cocaine, marijuana, opiates, and phencyclidine (PCP)—drug categories of key concern to the National Institute of Drug Abuse and the Department of Health and Human Services (
9,
10). Radioimmunoassay of hair is also thought to be less intrusive than urinalysis and less vulnerable to measures to avoid detection, because hair sampling is conducted directly by the individual obtaining the sample (
11).
After numerous studies of drug detection by hair analysis (
6), the U.S. General Accounting Office in 1993 endorsed the use of the technique in drug outcome studies (
12). Radioimmunoassay of hair has also been successfully used to detect substance use not found by urinalysis and self-report in populations of adult arrestees (
13), juvenile arrestees (
14), addicts (
15), pregnant women (
16), and, in a small study, persons with schizophrenia in London (
17); the technique has continued to be of interest (
18,
19,
20,
21,
22). Despite this interest, however, radioimmunoassay of hair has not come into general clinical use, perhaps because of concerns about patient acceptance.
To determine more definitively whether the measurement of illicit drug use among persons with schizophrenia can be improved through radioimmunoassay of hair, we compared the self-reported substance use of 203 persons with schizophrenia and related disorders with the results of their laboratory tests for substance use. We also sought to assess the acceptability of the radioimmunoassay of hair in this population.
Methods
The participants were drawn from the North Carolina site of the schizophrenia care and assessment program (SCAP) (
23), a multicenter, prospective observational study focused on the cost-effectiveness of new treatments for psychotic disorders in five geographic regions of the United States. A sample of 403 persons with schizophrenia-related disorders was recruited from several treatment facilities in a nine-county mixed urban and rural area in the north central region of the state. These individuals were originally recruited by means of two simultaneous strategies: sequential inpatient admissions at a regional public psychiatric hospital, an acute psychiatric unit of a private university hospital, and a Veterans Affairs hospital; and random selection of outpatients from four area mental health programs' case rosters and one Veterans Affairs medical center outpatient clinic. The SCAP research design involves no intervention or interference with usual patterns of treatment. Inclusion diagnoses were based on review of clinical records and included recently documented
DSM-IV diagnoses of schizophrenia, schizoaffective disorder, and schizophreniform disorder.
In 1997, participants still enrolled at the 18- or 24-month period of the SCAP study were consecutively approached for inclusion in this substudy of detection of illicit drug use. Few significant differences in demographic characteristics were noted between the original SCAP sample and the 203 participants enrolled in our study, as described below.
Following institutional review board approval, 241 SCAP participants were approached to participate in this study. Participants were informed of the confidentiality of the study, asked to provide informed consent, and offered $25 on completion of the study. Of those approached, 203 (84 percent) consented to participate. Reasons given for nonparticipation, which were not mutually exclusive, were lack of ability or willingness to give a hair sample by 20 persons (10 percent), lack of ability or willingness to give a urine sample by 10 persons (5 percent), and lack of willingness or ability to complete the accompanying interview by 21 persons (10 percent). Men were more likely than women to consent to participate (χ2=6.43, df=1, p=.011). Recruitment varied significantly by original recruitment site; SCAP participants from the state hospital and rural sites were more likely to refuse to participate in the substance abuse study than were those contacted from other sites (χ2=22.07, df=4, p<.001). There were no other significant differences in consent to participate.
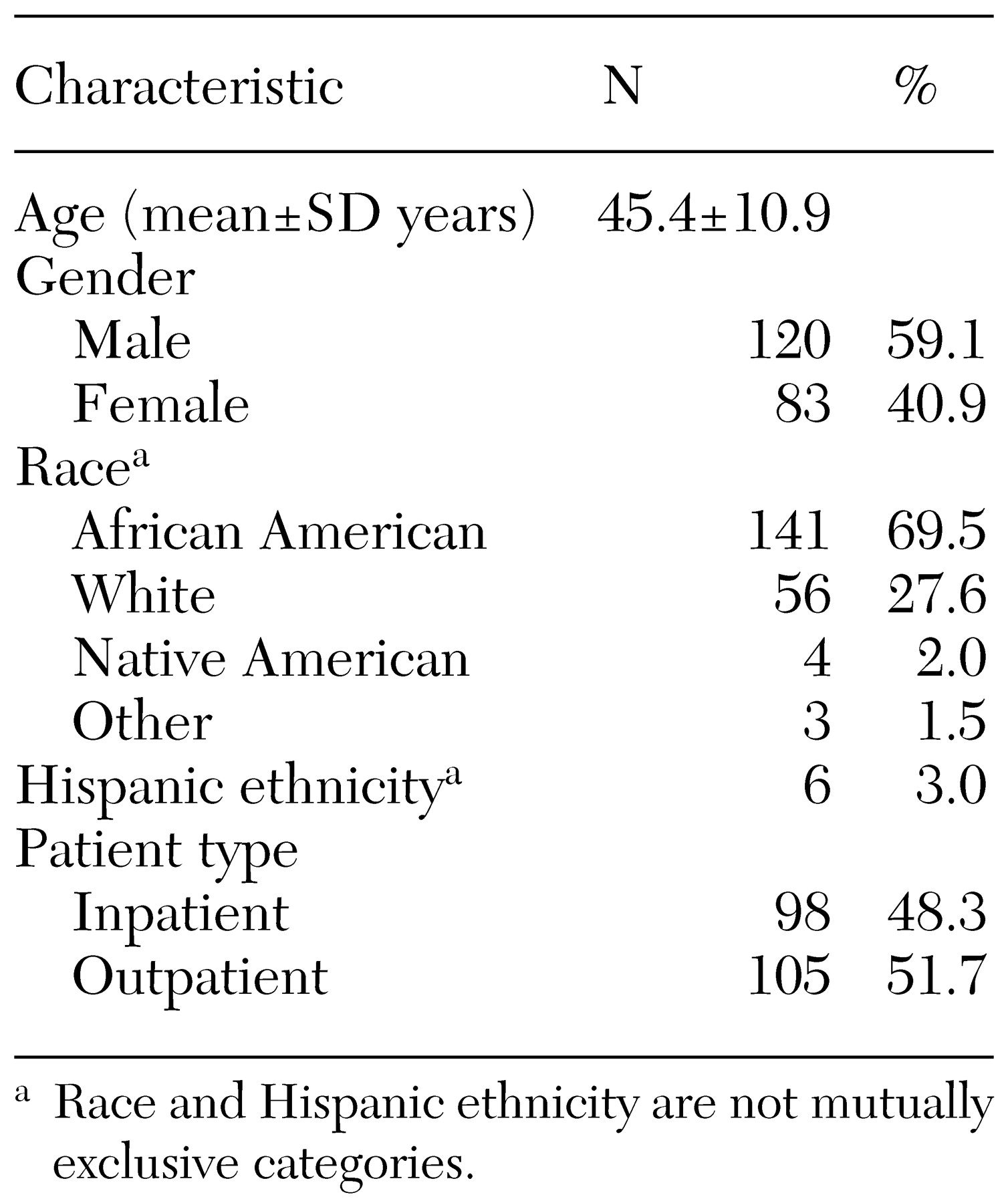
As shown in
Table 1, the majority of participants were male and African American, with a few participants reporting Hispanic ethnicity (race and Hispanic ethnicity were not mutually exclusive). The mean age of the sample was 45.4 years, and the median age was 44.5 years. The numbers of inpatients and outpatients were roughly equal.
Participants were asked how often in the past three months they had used illegal drugs or abused prescription drugs. Abuse of prescription drugs was defined as taking more of a prescription drug than was prescribed or taking someone else's prescription drug in order "to get high or change the way you feel." Those reporting any use of illegal drugs or abuse of prescription drugs were also asked detailed questions about their type and patterns of use. Participants were further queried about alcohol use, but these results are not reported, and confirmatory laboratory tests were not performed.
Participants submitted hair and urine samples for analysis. Hair specimens were tested for signs of substance use by the Psychemedics Corporation by means of radioimmunoassay of hair (
9). This technique assays drugs and their metabolites transferred from capillary circulation through the hair follicle to the internal hair structure. A tuft of hair about the diameter of pencil lead is cut from the scalp on the back of the head. Samples 1.5 inches long were taken from each participant. For participants with short hair, a larger volume of hair was removed. If no hair was present on the head, hair was taken from the chest, arm, or leg. With a hair specimen 1.5 inches long, drug use in the preceding three months can be assessed. Testing was performed for five substances: amphetamines, cocaine, marijuana, opiates, and PCP. A positive test is defined as a test value for a specific drug that is more than three standard deviations from the mean of a comparison sample of drug-free individuals. These tests were not used to quantify the extent of substance use. The hair tests were invalid for two participants, leaving 201 valid tests. In addition, for nine participants the test for marijuana was inconclusive. Inconclusive tests were counted as negative for the subsequent analysis.
Drug urinalysis was performed with a commercially available rapid multiple immunoassay urine drug test, Triage by Biosite, which was used to screen for seven substances: barbiturates, benzodiazepines, cocaine, marijuana, methamphetamines, opiates, phencyclidine. (Note that radioimmunoassay of hair does not assess the presence of benzodiazepines and barbiturates.)
Because several of the substances detected by the hair or urine tests also have legitimate prescription indications, participants were asked which drugs, including nonpsychotropics, had been prescribed for them in the past three months. Data from chart reviews were also available to evaluate prescribed medication for nearly all participants. Participants who tested positive for a prescribed medication detected in hair or urine were considered not to be abusing, and their tests were recorded as negative.
Results
Self-reported drug use
A total of 26 participants (12.8 percent) reported using illegal drugs and 12 (5.9 percent) reported abusing prescription medication in the past three months. These totals were not mutually exclusive. Self-reported use of illegal drugs and abuse of prescription medications were combined to create a measure of self-reported substance abuse. Of the 203 participants, 33 (16 percent) reported abusing drugs in the past three months, 17 (8 percent) reported using drugs one to several times a month, 12 (6 percent) reported using drugs one to several times a week, and four (2 percent) reported daily use. On the basis of all sources of information (self-report, hair, or urine), 78 participants (38 percent) were determined to be abusing substances.
Laboratory tests
All 203 participants submitted hair and urine samples for laboratory analysis. For two participants, the hair sample submitted was inadequate in volume to perform radioimmunoassay. In comparisons of hair test results with self-report and urinalysis findings, when sources of data were missing, the missing test results were assumed to be negative, resulting in a total sample of 201 for the hair test. Additionally, for nine participants the hair test for marijuana was inconclusive; in these cases the results were assumed to be negative.
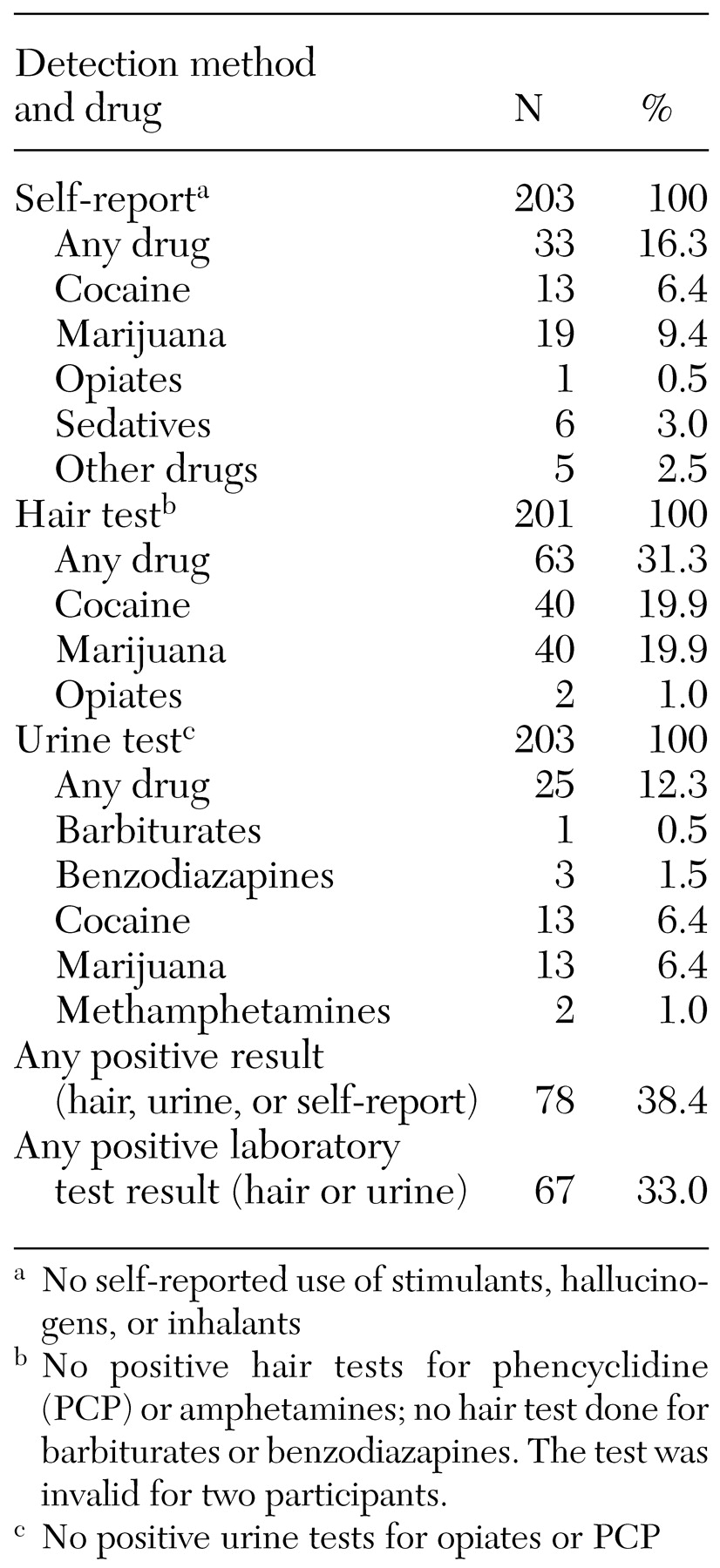
As shown in
Table 2, according to the urine test, 25 participants were using an illegal drug. Three participants tested positive for benzodiazepines, 13 for cocaine, two for methamphetamines, 13 for marijuana, and one for barbiturates. No one tested positive for opiates or PCP.
Also as shown in
Table 2, according to the hair test, 63 participants had used an illegal drug during the period covered by the hair test. A total of 40 of the 201 participants tested positive for cocaine, 40 for marijuana, and two for opiates. No participants had positive hair test results for PCP or amphetamines, and hair tests were not conducted for barbiturates or benzodiazepines.
Laboratory tests compared with self-reports
For all substances tested, 67 participants tested positive for substance use on either laboratory test, and 78 tested positive for substance use by laboratory test or self-report, as shown in
Table 2. Only 16 participants (8 percent) had positive results by all three measures. Of the 78 participants shown to be positive for substance use by any result, only 27 (35 percent) were found positive by more than one result.
Because of the shorter period of detection covered by the urine test, some positive cases of drug use would not have been detected by this method. The 42 participants who had a positive hair test but a negative urine test largely demonstrated the longer window of detection possible with radioimmunoassay. Conversely, four participants had a positive urine test but a negative hair test, indicating use that was too recent to be detected in hair or a lower level of drug than is detectable in hair.
If it can be assumed that false positives for substance use by self-report are unlikely, the 11 participants with self-reported substance use but no positive laboratory tests were of interest. Of these 11 participants, four reported abusing a sedative, two reported marijuana use, one reported cocaine use, two reported using other drugs, and one reported abusing marijuana, cocaine, and one other drug. None of the 11 participants had a hair test that was inconclusive for marijuana, and only one had an invalid hair test.
In these cases of self-report of substance use undetected by laboratory measures, the substance use may have been undetectable by the calibration of these assays, or the participants may have incorrectly reported their use in the three-month time frame or misidentified the substance they had used. These results also challenged the validity of the hair tests, although no other data were available to serve as an external validator of use.
The agreement between the combined laboratory tests and self-reported substance use was low by conventional tests of concordance (Cohen's kappa=.26, p<.001). It would be misleading to compare the sensitivity and specificity of these laboratory measures, given the differences between tests in period of detection. The urine test showed greater agreement with self-report (Cohen's kappa=.52, p<.001), and the hair test agreed only weakly with self-report (Cohen's kappa=.29, p<.001). The urine test, with its shorter period of detection, may have been more strongly associated with self-report than the hair test because participants, even when asked about the past three months, tended to recall only recent behavior, and therefore the shorter detection period may have better matched the participants' shorter recall period.
Hair test compared with urine test
For all drugs, the agreement between the hair test and the urine test was low (Cohen's kappa=.36, p<.001). Because radioimmunoassay of hair does not assess the presence of benzodiazepines and barbiturates, we removed these positive tests from the analysis, and we still found that the concordance rate did not change. The concordance rate for marijuana was even lower (Cohen's kappa=.31, p<.001). For cocaine, the concordance between the two laboratory tests was higher than the overall concordance (Cohen's kappa=.44, p<.001) but still not strong.
Bivariate relationships to drug use
Self-report of substance use was significantly associated with being male, being recruited from the inpatient group, and being younger, as shown in
Table 3. However, when positive results from the two laboratory tests combined were considered, none of these differences remained significant, suggesting that lower self-report of substance use in these groups might have been misleading. For example, the women were less likely to acknowledge substance abuse, but they appeared to have patterns of use similar to those of the men.
Also as shown in
Table 3, race and ethnicity, analyzed as African American compared with all others, including Hispanic, was not related to substance use by any assessment.
Discussion and conclusions
This study demonstrated that the use of laboratory measures combined with self-report can markedly improve the detection of substance use among persons with schizophrenia. Because any illicit drug use is likely to be problematic in this population, we focused on actual use rather than a formal diagnosis of drug abuse (
24,
25). When results from radioimmunoassay of hair and urinalysis were combined with self-report in a composite index, illicit drug use was identified for 38 percent of participants, compared with only 16 percent by self-report alone. The higher rates of detection with radioimmunoassay of hair are comparable to general estimates of problematic drug use in clinical samples (
24,
25). Moreover, compared with urine testing alone, radioimmunoassay of hair roughly doubled the detection of substance use, from 12 percent to 31 percent. It should also be noted that levels of self-report may be somewhat higher in clinical settings, where clinicians have ongoing relationships with their patients.
Participants in this study seemed to find radioimmunoassay of hair to be an acceptable procedure, although 10 percent refused to provide a hair sample—twice the refusal rate for a urine sample. Because we did not explicitly ask participants about the acceptability of the test, further studies should evaluate that. Because these research participants were compensated, the rates of acceptance of radioimmunoassay of hair may be higher than those in general clinical populations. Nonetheless, radioimmunoassay of hair appeared to be acceptable and nonintrusive.
The question remains as to how useful the three-month period of detection offered by radioimmunoassay of hair is as a time frame for assessment of illicit drug use among persons with schizophrenia. Given the growing awareness of the role of substance abuse in severe mental illness, this long period of detection may be of some value, especially when patients are seen relatively infrequently. A three-month window of detection does not provide an indicator of very recent use or of immediate need for detoxification or substance abuse intervention. However, this period could be likened to the use of a glycosylated hemoglobin test to detect poor glucose control in diabetes. The radioimmunoassay of hair gives a picture of substance abuse over a prolonged period. Clinically, this assay may be a very useful ancillary measure, because patients often abstain from using drugs before treatment contacts or may use drugs too sporadically for urine detection. Among patients with schizophrenia, for whom a low threshold of substance use is likely to be clinically significant and problematic, such a measure has added importance and may be especially valuable when combined with a urine test.
Generally, charges for radioimmunoassay of hair range between $35 and $75 per sample; the cost of a screening drug urinalysis is generally $25 to $35. Results for hair analyses can usually be obtained in several days if adequate numbers of samples are generated to justify the cost of conducting the assay.
Whether these higher rates of detection over a three-month period correlate with poor clinical outcomes is an open question for empirical research. In future research, we will examine rates of use of specific substances by method of detection, and we will evaluate the associations of these indicators with longitudinal treatment outcome measures to assess the value of radioimmunoassay of hair as a clinical tool and for research studies.