Chronic physical health problems
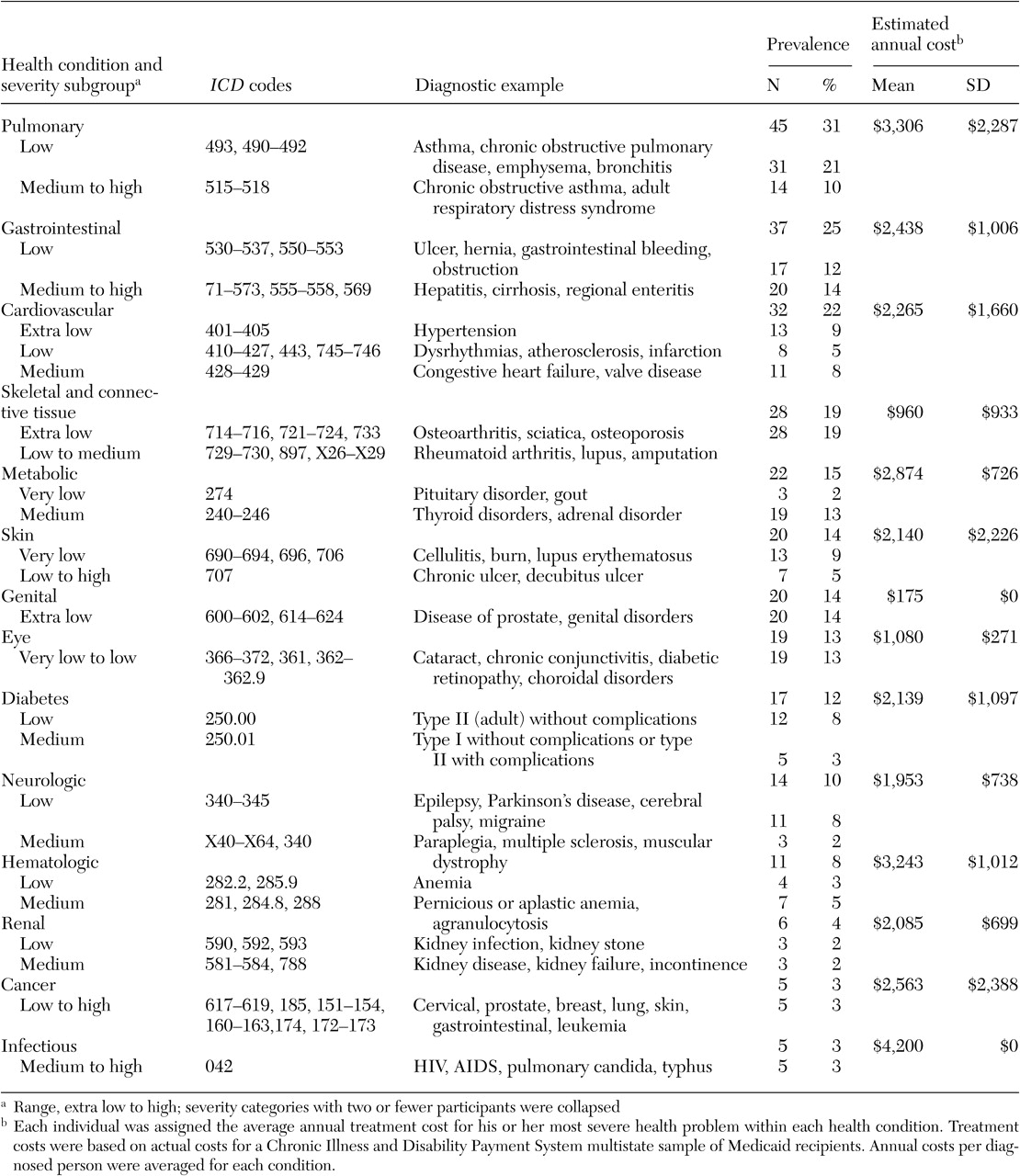
Prevalence and cost of treatment. Seventy-four percent (N=109) of our study sample was treated for one or more of the chronic health conditions listed in
Table 2. Chronic pulmonary disease was the most prevalent health condition, and it was second in cost only to infectious diseases. Overall, there was wide variation in average annual costs (range, $175 to $4,200), which were measured as the average of estimated annual costs per person receiving a diagnosis. Average cost and prevalence of health conditions were uncorrelated, substantiating the independence of these two health measures.
Comorbid physical conditions. Fifty percent (N=73) of our sample was treated for two or more of the 14 conditions listed in
Table 2. More than a third (N=46) were treated for three or more conditions, and a fifth (N=29) were treated for four or more conditions. Pulmonary disease was the most comorbid condition in our sample: 50 percent or more of participants with eight other health conditions were also treated for respiratory problems. Except for the pervasive co-occurrence of pulmonary disease and another disease, dual diagnoses of health conditions were diverse. Less than 50 percent of participants with gastrointestinal diseases, metabolic diseases, or diabetes had a co-occurring physical condition.
Health condition severity. A high correlation was found between each individual's estimated annual total cost of treatment (overall health problem severity) and total number of health conditions (r=.85, p<.001). Estimated average annual cost of treatment for individuals with chronic pulmonary disease (45 persons, or 31 percent) was four times that of a person without chronic pulmonary illness (102 persons, or 69 percent; mean of $8,277±$5,632 compared with a mean of $2,270±$2,713; t= 6.75, df=144, p<.001), even with an outlier of $40,000 omitted. Otherwise, estimated total cost per person across the 14 health categories was highly variable (mean of $4,315± $5,491).
Mortality. Eleven participants (6 percent) from the Massachusetts Employment Intervention Demonstration Project sample (N=176) died during the study period, seven of whom were in our Medicaid subsample (N=147). Dual diagnoses were very evident: five of the 11 deaths were due to pulmonary illness (lung cancer, chronic obstructive pulmonary disease, or pneumonia), and all five of these deaths were associated with a severe substance use disorder. Except for a single death that was caused by diabetes, the other six deaths were directly related to a substance use disorder (overdoses and drug-related murder), often with a co-occurring severe illness, such as AIDS. Ten of the 11 participants who died during the study were Caucasian and older than 35 years, and there was an even split in gender (five females and six males). Seven of the deceased had psychiatric diagnoses of bipolar disorder or major depression.
Correlations with background characteristics. By using estimated annual costs per condition as a measure of severity, we compared participants on eight background characteristics across the 14 CDPS diagnostic categories, with a moderately stringent threshold for statistical significance (p=.02). As
Table 3 shows, participants who were treated for pulmonary disease were more likely to have been given a diagnosis of major depression or bipolar disorder than a diagnosis of schizophrenia, and they were more likely to have an active substance use problem. Infectious disease was also associated with a substance use disorder and with homelessness. Because 84 percent of persons who were homeless at any time during the project (16 of 19 participants) were treated for a substance use disorder, but only 40 percent of those with an active substance use disorder (16 of 40 participants) were homeless at any time during the project, substance use disorder may account for the greater incidence of infectious disease among participants who were homeless, but homelessness cannot account for the greater incidence of infectious disease among participants who had a substance use disorder.
Gender, obesity, and age were also predictive of health problems. Women had more metabolic (thyroid), skeletal and connective (arthritis), eye, and genital disorders than men. Also, obesity was associated with a higher incidence of both metabolic and gastrointestinal disorders. Age differences were also evident: only one participant younger than 33 years had a serious pulmonary disease, and no one older than 45 years had an infectious disease. One medical condition, cardiovascular disorders, showed a clear progressive increase across age groups for both hypertension and heart problems. Participants aged 45 through 75 years at baseline had higher rates of hypertension (11 participants, or 30 percent) than those aged 34 through 44 years (seven participants, or 11 percent) or those aged 18 through 33 years (three participants, or 6 percent) (p=.006). Likewise, participants aged 45 through 75 years at baseline also had more heart problems (ten participants, or 27 percent) than those aged 34 through 44 (six participants, or 10 percent) or those aged 18 through 33 (three participants, or 6 percent) (p=.011). No racial or ethnic differences were found in the prevalence of any health condition.
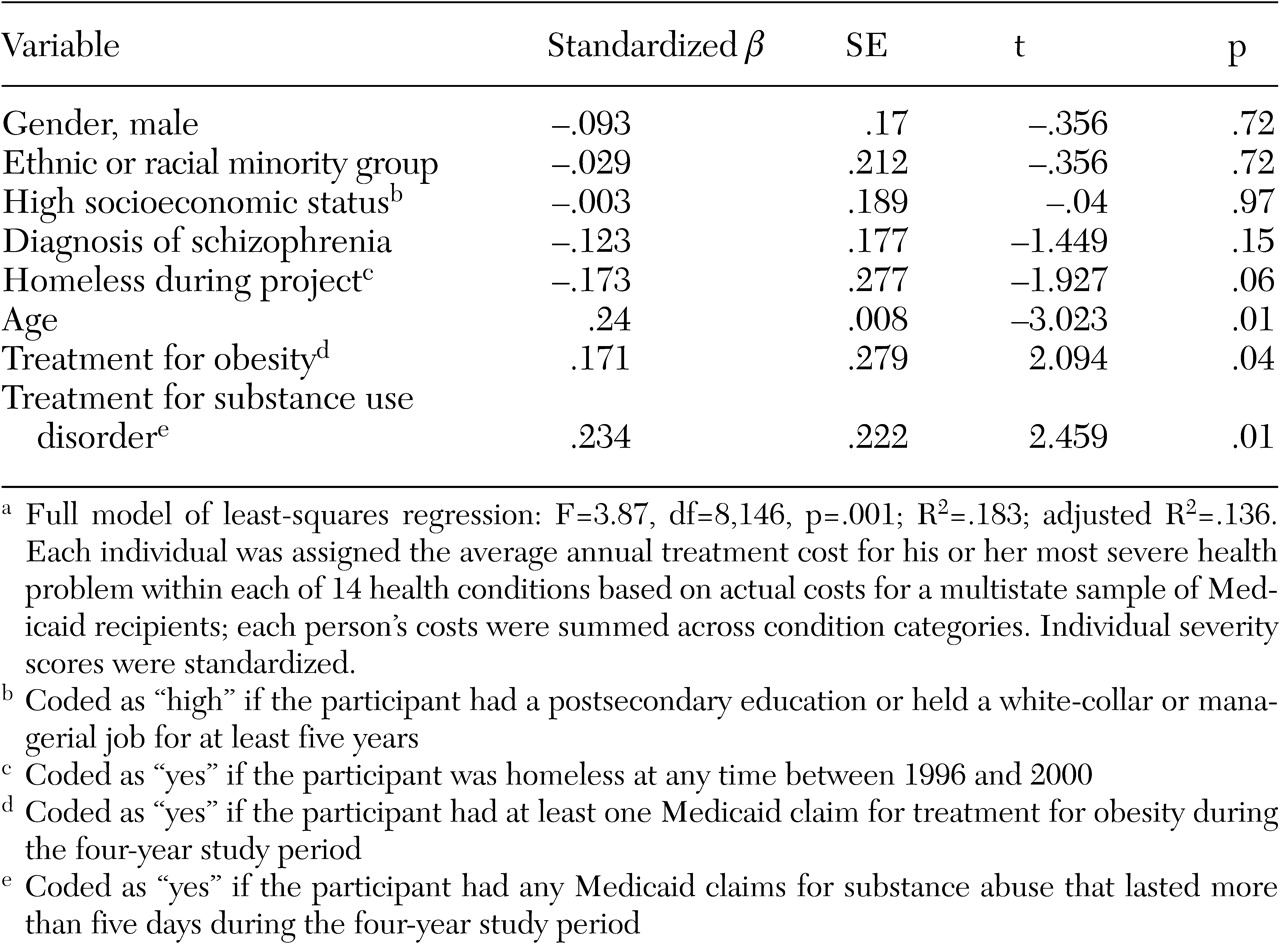
Predictors of health problem severity. As shown in
Table 4, a regression analysis was conducted to identify personal characteristics that were predictive of health problem severity (standardized estimated annual treatment costs per person). The overall model was statistically significant, with age, substance use disorders, and obesity as significant predictors; the .05 level of significance (two-tailed test) was used. To test the robustness of these findings, the analysis was repeated with the inclusion of participants in the Massachusetts Employment Intervention Demonstration Project who were not Medicaid recipients (N=30). We used interview data to identify health problems, obesity, and substance use disorders for these additional participants. The new model was statistically significant (F=3.73, df=8, 164, p=.001; R
2=.181; adjusted R
2=.139), with the same significant covariates: age (B=.239; p=.002), obesity (B=.174, p=.024), and substance use disorder (B=.246, p=.006). Although substance use disorder, age, and obesity were not collinear, 30 percent of persons aged 45 or older at baseline in the Medicaid subsample (11 of 37 participants) and the total Massachusetts Employment Intervention Demonstration Project sample (12 of 42 participants) were both obese and had a substance use disorder.