Estimates of the prevalence of depression range from 2.5 percent among children to 8.3 percent among adolescents (
1). The onset of depression appears to be occurring earlier in life (
2). Early-onset depression, if left untreated, can persist, recur, and continue into adulthood and may lead to more severe depression (
3). Depression among children and adolescents is associated with an increased risk of suicidal behavior and suicide (
3).
A limited number of antidepressant medications have been approved by the U.S. Food and Drug Administration (FDA) for treatment of pediatric obsessive-compulsive disorder (
4). Before 2003, no antidepressant had FDA approval for the treatment of depression in the pediatric age group (
5). Although psychotherapy is considered the first-line therapy for mild to moderate depressive disorders in this patient population (
6,
7), off-label use of antidepressants for depression appears to be widespread (
8,
9) and gaining in acceptance. Studies have reported three- to tenfold increases in the prevalence of antidepressant use among children and adolescents from 1987 to 1996 (
10,
11).
The use of antidepressants to treat depression among pediatric patients remains controversial (
12). Off-label drug use in this age group has been described as "an experiment with every use (
13)." Published studies of antidepressant treatment of depression among youths have shown these agents to be only modestly effective; many treated patients continue to experience symptoms (
14,
15,
16). Tricyclic antidepressants have not been found to be effective for treating depression among prepubescent children (
17) and have been implicated in pediatric sudden death (
18). Recently, the FDA, the United Kingdom's Medicines and Healthcare Products Regulatory Authority, and Health Canada recommended that paroxetine, a selective serotonin reuptake inhibitor (SSRI), not be used among children and adolescents, because its efficacy has not been established for depression among youths and its use is associated with increased risk of suicidal thinking and suicide attempts (
19). This issue is currently the subject of great debate. The evidence of increased risk of suicide with use of the other SSRIs in pediatric populations currently is being reviewed.
Recent data on trends in the ambulatory use of antidepressants overall and by class in nationwide samples of young patients are limited. Given this fact along with the dearth of data on the safety and efficacy of antidepressants for the pediatric age group and the fact that approximately 65 percent of all children were commercially insured beneficiaries in 2000 (
20), a contemporary description of the patterns of use of antidepressants in this population is warranted. The objectives of the population-based, retrospective study reported here were to estimate the prevalence of use of the different classes of prescription antidepressant medications among commercially insured children and adolescents in ambulatory care by using national pharmacy claims data to examine trends in antidepressant use from 1998 to 2002.
Results
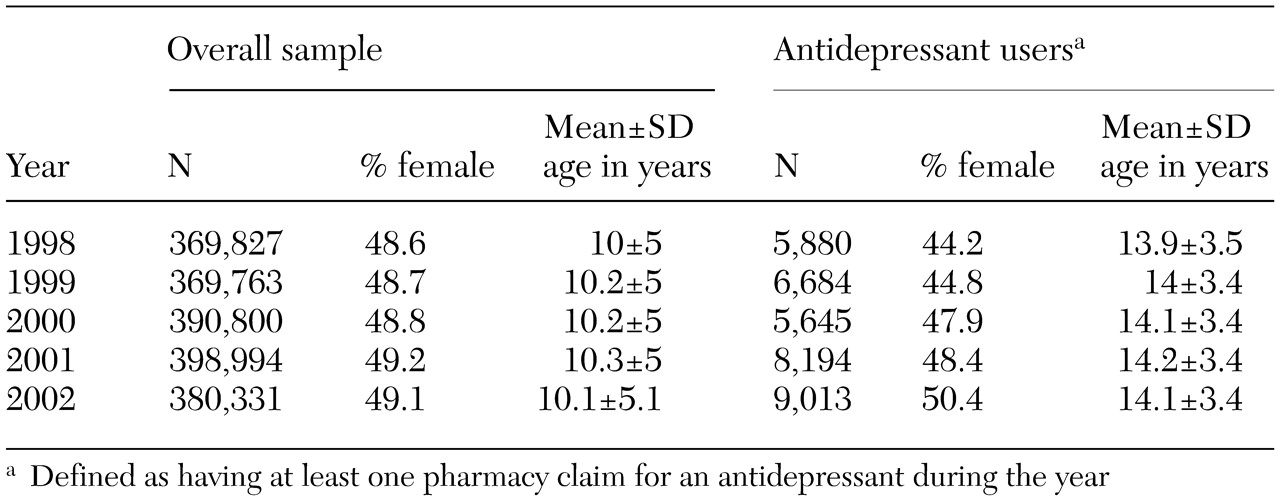
The overall sample of commercially insured children and adolescents increased from approximately 370,000 in 1998 to more than 380,000 in 2002, as can be seen from
Table 1. Over the study period, the proportion of girls increased, but the mean age of children in the sample remained relatively constant in both the overall sample and the subsample of antidepressant users. This resulted in a sample of child and adolescent antidepressant users in 2002 that was older and had a slightly higher proportion of girls relative to the overall sample.
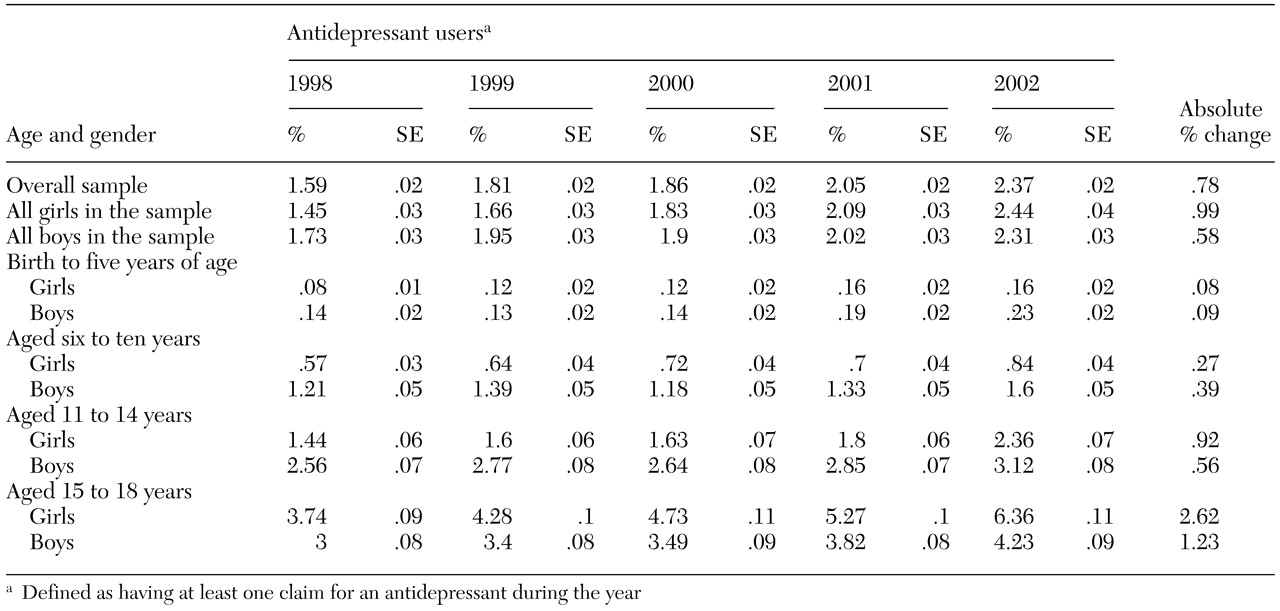
From 1998 to 2002, the overall prevalence of antidepressant use increased by 49 percent, as can be seen from
Table 2. Log-rate modeling indicated that the overall prevalence of antidepressant use increased significantly (p<.001) at an adjusted rate of 9.2 percent per year over the study period (model goodness of fit p=.180 with a deviance of 37.9, df=31). The largest year-to-year proportional increase in overall prevalence occurred between 2001 and 2002 (16 percent).
The prevalence of antidepressant use increased in all strata of age and gender in 2002 compared with 1998. However, prevalence increased more markedly among girls (68 percent) than among boys (34 percent). The prevalence was higher for boys at younger ages, but girls had a higher prevalence by the time they reached high school age. When 2003 was compared with 1998, girls and boys aged 15 to 18 years showed the largest absolute changes in prevalence (2.6 and 1.2 percentage point increases, respectively). However, the youngest age group (aged zero to five years) showed the largest proportional increase in prevalence within the respective gender categories (100 and 62 percent for girls and boys, respectively).
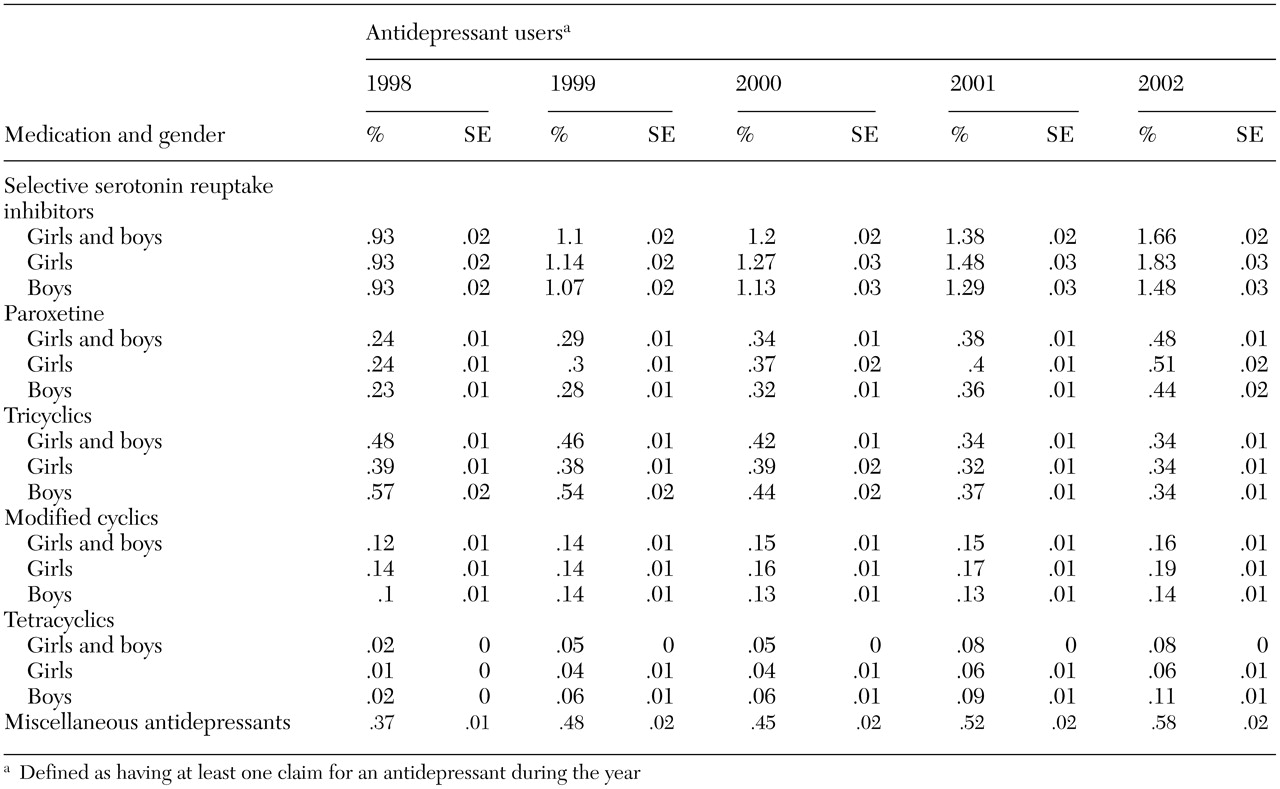
The overall prevalence of use for all antidepressant classes increased during the study period except in the case of tricyclics (a decrease of 29 percent), as can be seen from
Table 3. In all five years of the study, SSRIs were the most commonly prescribed antidepressants, and tetracyclics were the least prescribed. Although tetracyclics (mirtazapine) had the lowest prevalence of use of all antidepressant classes, this class had the largest proportional increase in prevalence over the study period—400 percent overall. The largest absolute increase in overall prevalence over the five years was for SSRIs (.7 percentage points). The prevalence of use among girls increased by 97 percent for SSRIs and 114 percent for miscellaneous antidepressants—including the serotonin and norepinephrine reuptake inhibitor venlafaxine—over the study period. The prevalence of use of the SSRI paroxetine increased by 113 percent and 91 percent among girls and boys, respectively, from 1998 to 2002.
Discussion
Our results suggest a continuing growth in the use of antidepressants among patients aged 18 years or younger. The adjusted trend in the prevalence of use of antidepressants among children and adolescents increased at an annual rate of 9.2 percent. The proportional increase in overall prevalence of use that we observed during the study period (about 50 percent over five years) was less than the three- to tenfold (
10,
11) increases over ten years that were reported in studies performed in earlier periods in a variety of study populations. However, the rates of increase observed in these other studies (
10,
11) reflect increases from lower base prevalences. These findings suggest that rates of growth, in terms of absolute prevalence increases observed from the late 1980s to mid-1990s, are continuing.
The prevalence of overall use of antidepressants in our pediatric population (160 per 10,000 in 1998) was similar to rates reported for 1996 by Olfson and associates (
11) (100 per 10,000) in a national survey and by Zito and associates (
10) (160 per 10,000) in a health maintenance organization. The 1999 prevalence of use of SSRIs (110 per 10,000) and paroxetine (30 per 10,000) in our pediatric population was similar to that estimated by Shatin and Drinkard (
24) for the same year (130 per 10,000 and 38 per 10,000, respectively) in a nationwide sample of employer-insured patients less than 20 years of age.
A number of factors acting together or independently may have led to the escalated use of antidepressants among children and adolescents, including increasing rates of depression in successive age cohorts (
2), a growing awareness of and screening for depression by pediatricians (
25), emergent extrapolation of the safety and efficacy of antidepressant pharmacotherapy seen by clinicians among adults to the needs of pediatric patients (
11), and greater reliance on pharmacotherapy by general practitioners as coverage for mental health services, such as psychotherapy, becomes more limited (
26). The increasing trend we observed in overall antidepressant use appears to have been driven primarily by greater use of SSRIs.
As in other studies, we found that the use of antidepressants was higher among younger male and older female pediatric patients (
8,
24). We also found substantial proportional increases in the prevalence of overall antidepressant use among female and male preschoolers (
10), increasing prevalence with each successive age group (
27), and a marked increase in the prevalence of SSRI use (
9,
24) and decrease in tricyclic use (
24). The prevalence of paroxetine use in our sample increased by approximately 100 percent from 1998 to 2002, a finding that is similar to that reported by Shatin and Drinkard (
24) (a 102 percent increase from 1995 to 1999), which suggests a continued growth in use of paroxetine through the late 1990s and into the 21st century. This finding is of note given FDA's recent recommendation that paroxetine not be prescribed for depression among pediatric patients (
19).
Several factors should be considered in interpreting our findings. Our data did not enable us to document whether youths who received antidepressants had a diagnosis of depression. However, available data suggest that antidepressants are prescribed for children and adolescents for depression more than for anxiety disorders (
28), and prescription claims have been shown to be a reliable and valid source of data for documenting treatment for depression among adults (
29). As with any analysis involving the use of administrative claims data, a claim does not indicate whether the patient actually took the medication. In addition, although this study did exclude publicly insured pediatric patients, the generalizability of the results is likely to be robust given that previous investigations have documented similar if not higher rates of growth in antidepressant use among Medicaid beneficiaries than among commercially insured pediatric beneficiaries (
10,
30).
Although we were unable to assess the community prevalence of depression in our sample, the proportions of youths we observed receiving any antidepressants (.2 percent to 1.6 percent of children and 2.4 percent to 6.4 percent of adolescents in 2002) are substantially lower than the estimated U.S. national prevalence of depression in these age groups (2.5 percent of children and 8.3 percent of adolescents) (
1). Even if all the children and adolescents with an antidepressant claim in our study were being treated for depression, these findings suggest that the use of prescription antidepressants among pediatric patients will continue to grow as more children and adolescents with depression have their illness diagnosed and treated. This potential growth highlights two differing but not mutually exclusive beliefs: first, the concern that antidepressants are being prescribed for children and adolescents in the face of insufficient information about their safety and efficacy in this population (
31) and, second, the inference that advocacy work to identify and treat depression among children and adolescents has begun to pay off (
32). We were unable to assess the merit of these two views in our study.