Sample
Researchers at the National Health Research Institute used identification cards and birth dates to verify unique persons in the Bureau of NHI population database and gave each person a series number to construct a sampling frame. The National Health Research Institute then compiled a database of 200,432 randomly selected persons, about 1 percent of the population, for use in a related health insurance study (
16). No statistically significant differences in age or sex were found between the group that was selected and all enrollees. The data consisted of ambulatory care and inpatient records as well as the registration files of NHI enrollees.
Enrollees were excluded from our study if they had not been eligible for NHI during 2000. As a result of this criterion, 14,542 persons were excluded. An additional 47,976 persons under the age of 18 years were excluded from our study. The final sample consisted of 137,914 persons. Data for persons who had at least one service claim in 2000 for either ambulatory or inpatient care, with the principal diagnosis of a psychiatric disorder, were categorized into one of the psychiatric disorder classifications according to
International Classification of Diseases, 9th Revision, Clinical Modification (
ICD-9-CM) diagnostic criteria (
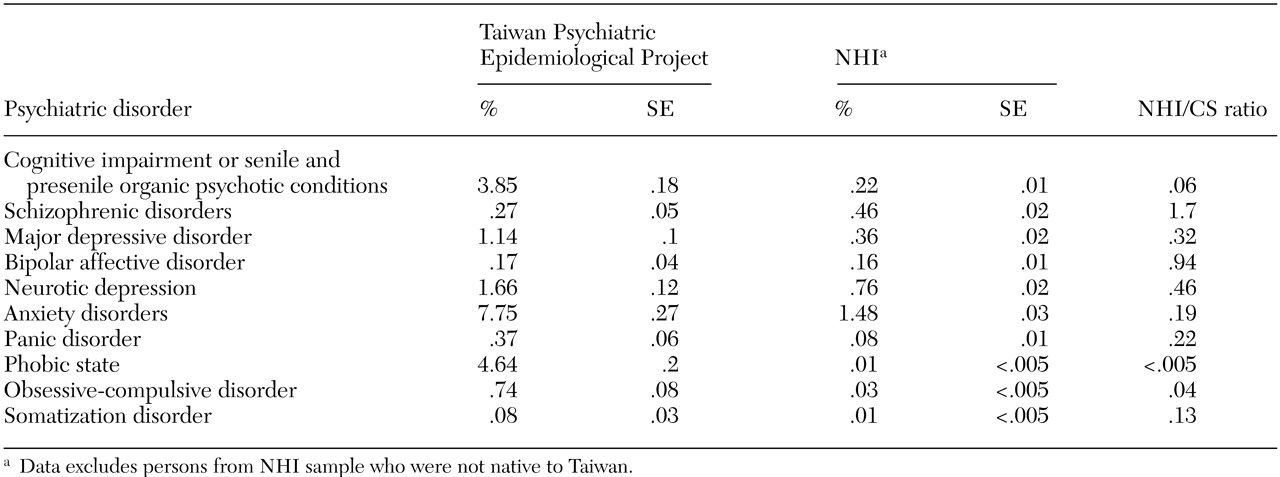
17). We divided psychiatric disorders into any major psychiatric disorder and any minor psychiatric disorder. Major psychiatric disorders included
ICD-9-CM codes 290 through 298. Minor psychiatric disorders included
ICD-9-CM codes 300 through 316, excluding 303 through 305 and 312 through 315. Major depressive disorder is grouped with affective psychoses; in
DSM-III-R it is called major depression. In our study it was classified as a mood disorder and was coded as 296.x. Neurotic depression in
ICD-9-CM—called dysthymia in
DSM-III-R—was coded as 300.4. The "any psychiatric disorder category" consisted of both major and minor psychiatric disorders.
When claims data showed that a person had two or more types of psychiatric disorders, we established a method to decide which diagnosis should be considered the primary diagnosis to be used in the study. In Taiwan, patients who have one or more major psychiatric disorders, including ICD-9-CM codes, can apply for catastrophic illness registration (CIR) cards, which are provided by the Bureau of NHI. These enrollees do not make copayments for mental health care. For persons who had two or more major psychiatric disorders listed in the claims data, the diagnosis listed on the CIR card was used. For persons without CIR cards, we chose the diagnosis associated with inpatient treatment (by frequency), and for persons with no inpatient stays, we chose the diagnosis associated with outpatient care (by frequency), followed by the diagnosis that was assigned by a psychiatrist. For persons with two or more minor psychiatric disorders, we followed a similar algorithm, except these persons did not have CIR cards.
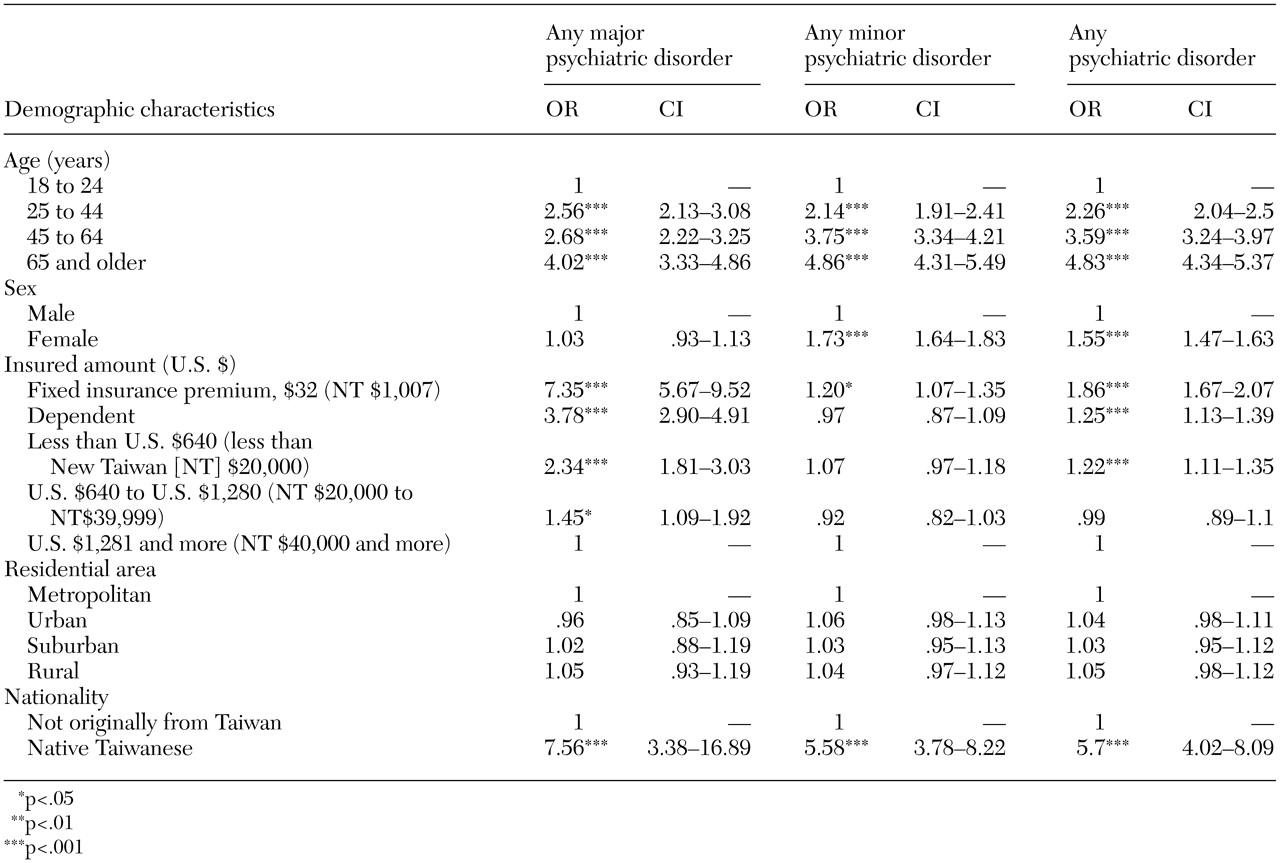
Data for demographic variables—including age, sex, insured amount, residential area, and nationality—were obtained directly from the National Health Research Institute files. Four age groups were used: 18 to 24 years (22,436 enrollees, or 16.3 percent), 25 to 44 years (63,256 enrollees, 45.9 percent), 45 to 64 years (35,731 enrollees, 25.9 percent), and 65 years or older (16,491 enrollees, 12 percent). Data for 68,709 males (49.8 percent) and 69,202 females (50.2 percent) were obtained for our study. The insured amount was classified into one of five categories: fixed insurance premium (which indicated the lowest socioeconomic status, U.S. $32 (New Taiwan [NT] $1,007; 15,086 enrollees, or 10.9 percent), dependent (no premium information was available for dependents; 32,189 enrollees, or 23.3 percent), less than U.S. $640 (NT $20,000; 50,569 enrollees, or 36.7 percent), U.S. $640 to $1,280 (NT $20,000 to $39,999; 26,480 enrollees, or 19.2 percent), and U.S. $1,281 or more (NT $40,000 or more; 13,590 enrollees, or 9.9 percent). Residential area was divided into four areas: metropolitan (36,756 enrollees, or 26.6 percent), urban (45,405 enrollees, or 32.9 percent), suburban (18,422 enrollees, or 13.4 percent), and rural (37,331 enrollees, or 27.1 percent). Nationality was divided into persons who were native Taiwanese (133,636 enrollees, or 96.9 percent) and persons who were not native Taiwanese (4,278 enrollees, or 3.1 percent).
Insured amount is based on and approximate to the monthly wage of the insured and ranges from NT $15,840 to NT $87,600. For the insured group of wage earners, the total monthly premium of an insured family is the insured amount times the premium rate (4.55 percent in 2000) times the employee contribution rate (30 percent) times the (1+number of dependents). For example, for an insured family who has an insured amount of NT $42,000 and two dependents, the total monthly premium of the insured family is NT $1,720 (U.S. $55.1) [NT $42,000 × 4.55 percent × 30 percent × (1+2)=NT $1,720 (U.S. $55.1)]. For the insured group without salaried income, the average premium remained at NT $1,007 (U.S. $32) in 2000.