Data sources
Data on Medicaid eligibility, medical encounters, and medication use were used for our study. Eligibility files included information on the individual's age, gender, race and ethnicity, enrollment dates, and state-assigned eligibility category, which related to disability, foster care, and low-income status. Data on disabling conditions were not available from Medicaid claims, but disability eligibility was determined by federal standards.
Medical encounter files produced service use variables, including service date, provider type, medical diagnosis, medical procedures, and service setting. Provider categories were mental health (psychiatrists, psychologists, mental health and substance abuse clinics, and psychiatric clinics), primary care (physicians, pediatricians, managed care, nurse practitioners, Early and Periodic Screening, Detection, and Treatment providers, and general health clinics), or other specialty (home or personal care providers, outpatient hospital clinics, neurology, and rehabilitation).
International Classification of Disease, 9th Edition (ICD-9) codes represented clinician-reported diagnoses. Claims-based diagnostic information has been found to be fairly complete, with 54 to 100 percent corresponding with the medical record data (
45,
46,
47,
48). The three-digit major category code has been found to be more reliable than specific five-digit codes (
49). Organized by major group, diagnoses found in our study included ADHD, adjustment disorder, anxiety, autism, bipolar disorder, conduct disorder, depression, developmental disability, learning disability, mental retardation, oppositional defiant disorder, personality disorders, psychoses, substance use disorders, and tic disorders. All other codes were categorized as "other psychiatric disorders."
Procedures, recorded as Current Procedural Terminology 1998, Standard Edition (CPT), were classified as mental health, developmental, and general medical. Mental health-related procedures included CPT codes 90801 to 90899, methadone drug level testing, psychological testing, and several state-specific codes, including individual and group mental health treatments, substance abuse counseling and services, psychiatric rehabilitation, residential treatment-based behavioral therapy, and day treatment services. These codes were classified further as psychopharmacologic management, psychotherapy, school-based services, substance abuse and mental health treatment, and "all other" (for example, psychiatric evaluations). Developmental procedures included speech and language as well as physical and occupational therapy. General procedures were all other evaluation and management visits.
Psychopharmacologic medications were identified from the pharmacy claims. The major therapeutic classifications were stimulants, antidepressants, antipsychotics, antiparkinsonian medications, sedatives and hypnotics, anxiolytics, anticonvulsants, and lithium. Antidepressants were also identified as selective serotonin reuptake inhibitors (SSRI) and tricyclic antidepressants, given the more frequent use of SSRIs for ADHD (
50). Because carbamazepine and valproic acid are used in treating patients with psychiatric disorders, these medications were subgrouped as mood-stabilizing anticonvulsants.
Analytic plan
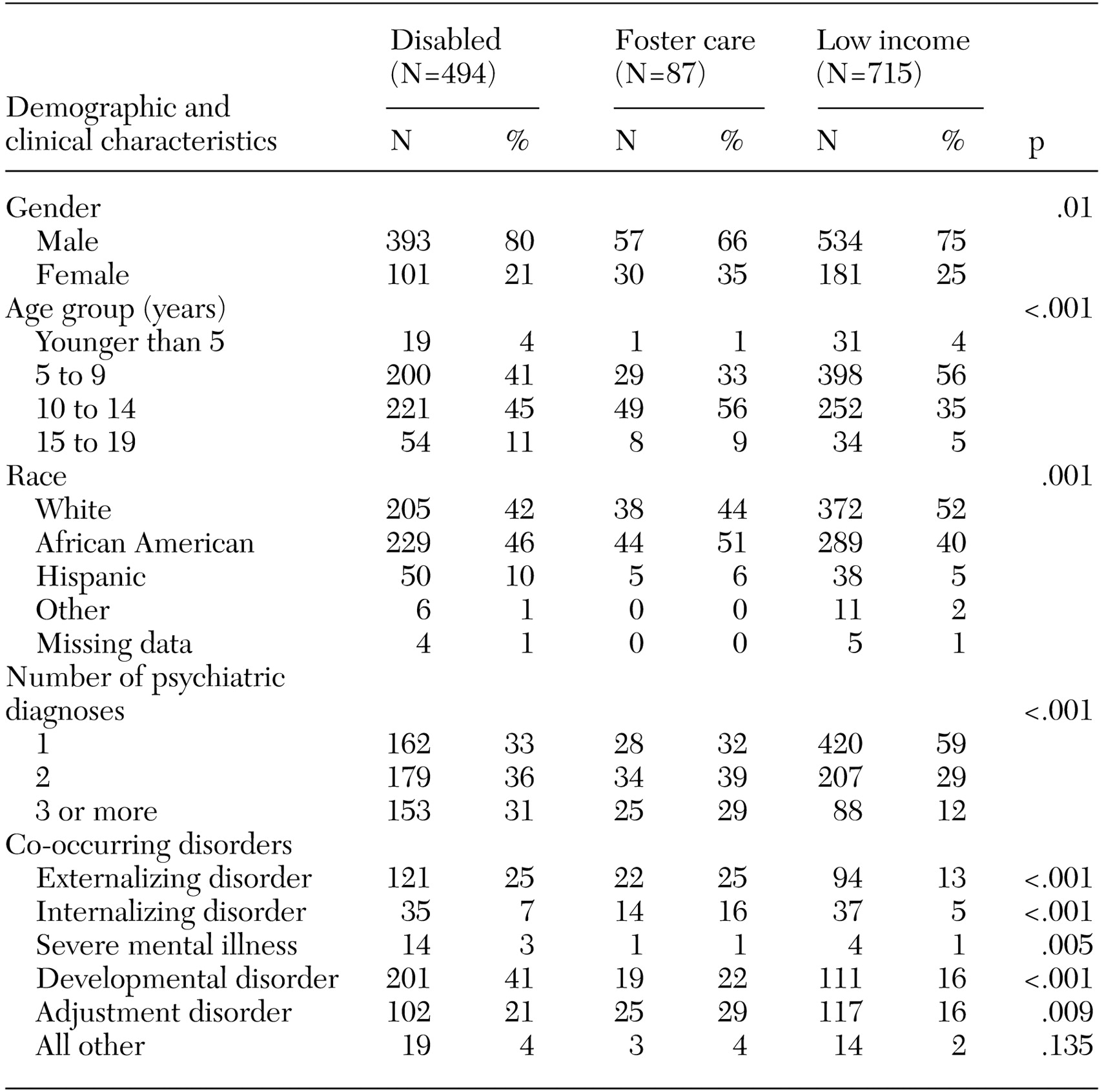
Descriptive statistics were used to characterize the population, and bivariate chi square analyses were used to test associations between demographic characteristics, mental health services, and psychopharmacologic treatments by Medicaid subgroup. Three polytomous logistic regression models were used to test the associations between Medicaid subgroup and each dependent variable: number of different classes of psychopharmacologic medications (model 1), psychopharmacologic regimen (model 2), and single versus combined pharmacotherapy and psychotherapy treatment (model 3). Use of medications from different classes was the basis for identifying receipt of none, one, two, or three or more psychopharmacologic medications. Psychopharmacologic regimen was stimulant only, stimulant with at least one other medication, or nonstimulant only. Psychopharmacologic medication only, psychotherapy only, or both was used to define single versus multimodal treatment. No psychopharmacologic treatments (model 1 and 2) and multimodal treatments (model 3) were the reference groups. The independent variable was Medicaid subgroup, as defined by disability (referent), foster care, and low-income. Models adjusted for age, gender, race and ethnicity, psychiatric diagnoses, and provider specialty. To avoid small cell sizes, diagnostic categories were collapsed as externalizing disorder (conduct and oppositional defiant disorders), internalizing disorder (depression and anxiety), severe mental illness (psychoses and bipolar disorder), developmental disorder (mental retardation, autism, developmental delays, and tics), adjustment disorder, and all other disorders.
Variables were added sequentially to the model on the basis of original hypotheses and significant bivariate associations. Model fit was ascertained by using log-likelihood tests. Medicaid subgroup was entered first, followed by demographic variables (age, gender, and race and ethnicity), mental health service use indicators, provider specialty, and co-occurring diagnoses, retaining only variables that improved the model fit. A two-tailed, 5 percent significance level with a Bonferroni correction (p<.002) for multiple comparisons was used. All analyses were performed by using SAS version 8.2.