There is growing concern about increasing rates of diagnosis of autism and attention-deficit hyperactivity disorder (ADHD) and about whether this observed increase is associated with environmental agents (
1,
2,
3), improved ascertainment (
4,
5), or overdiagnosis (
6,
7,
8,
9). Although recent cross-sectional studies have examined the prevalence of ADHD (
10,
11) and autism (
12,
13,
14), few studies have examined trends in the prevalence of these disorders. Some studies have examined trends in treated prevalence. For example, Kelleher and colleagues (
5) found that pediatricians identified attention problems such as ADHD among 1.4 percent of children in 1979 and 9.2 percent of children in 1996, an increase of 657 percent. Data from the U.S. National Ambulatory Medical Care Survey suggest a 250 percent increase between 1990 and 1998 in the number of children receiving a diagnosis of ADHD (
15). Zito and colleagues (
16) found that children's ambulatory care discharges for ADHD increased from 1.9 percent to 3.6 percent.
Similar studies have indicated as much as a 373 percent increase in the number of reported cases of autism spectrum disorders from 1980 to 1994 (
17). California's Department of Developmental Services reported an additional 100 percent increase in rates of autism from 1992 to 1997 (
18). It is unclear whether this observed change represents a true increase in the community prevalence or is a function of improved recognition and diagnosis (
4,
19,
20,
21).
Other studies have shown concurrent increases in rates of diagnosis of other psychiatric disorders among children and adolescents. In their comprehensive reviews, Rutter and Smith (
22) and Fombonne (
23) provided evidence of increases in rates of diagnosis of depressive disorders, suicide, and substance use disorders. Similarly, Achenbach and Howell (
24) found slight increases in parents' reports of children's problems. These general increases in pathology parallel physicians' increased recognition of psychosocial problems (
5) and children's increased use of health care services for behavioral and emotional disorders (
25,
26).
It is possible that the community prevalence of all these disorders is increasing simultaneously. However, it is also possible that changes in parental and social expectations, methods of ascertainment, awareness of the signs and symptoms of psychiatric disorders, and changes in diagnostic thresholds are responsible for the observed increase in rates of diagnosis of these disorders. In any case, it is critical that these changes be examined in the context of other—presumably unrelated—disorders, so that patterns can be compared. To our knowledge, no study has examined the changing rates of these disorders over time in the same data set. The goal of the study reported here was to examine trends by age and calendar year in the diagnosis of autism spectrum disorders and ADHD at hospital discharge in the context of hospital discharges for other psychiatric disorders.
Methods
Data from the Healthcare Cost and Utilization Project (HCUP) were used to examine secular trends in diagnosed psychiatric disorders between 1989 and 2000. The HCUP Nationwide Inpatient Sample (NIS) approximates a 20 percent sample of U.S. community hospitals. The American Hospital Association defines community hospitals as "all nonfederal, short-term, general, and other specialty hospitals, excluding hospital units of hospital institutions." Specialty hospitals, such as obstetric-gynecology, ear-nose-throat, short-term rehabilitation, orthopedic, and pediatric hospitals, were included, and long-term hospitals, psychiatric hospitals, and chemical dependency treatment facilities were not included in the survey.
The NIS includes data from selected states that agreed to provide data for all payers for inpatient hospital discharges. The NIS used a stratified probability sampling of community hospitals intended to select 20 percent of each stratum. Sampling strata were defined by five hospital characteristics: region (Northeast, Midwest, West, or South), control (government nonfederal, private not-for-profit, or owned by a private investor), urbanicity (urban or rural), teaching status (teaching or nonteaching), and bed size (small, medium, or large). Each year of the NIS contains data for between 800 and 1,000 hospitals and approximately five to seven million records. The NIS includes sample weights that provide both state- and national-level estimates.
Sample
This study included all hospital discharges from calendar years 1989 to 2000 in the HCUP NIS for individuals from birth to age 21 years. Individuals could be included in the sample more than once if they had multiple discharges.
Measures
Psychiatric disorders were coded by using the
International Classification of Diseases, 9th Edition (
ICD-9) (
27). Disorders were associated with a hospital discharge if they were coded in any position for that discharge. Comorbid conditions were double-counted for all analyses. Autism spectrum disorders were coded for any discharge with a 299.0 diagnostic code, ADHD for any discharge with codes 314.00 to 314.99, major affective disorders for any discharge with codes 296.00 to 296.99, and substance use disorder for any discharge with codes 303.00 to 305.99.
Analyses
For each set of disorders, three rates were calculated. First, the rate of hospital discharges associated with each disorder was calculated for each calendar year as a function of the total number of hospital discharges for that year. Second, average rates were calculated across all years of the study period by age. Finally, the sample was divided into four periods: 1989 to 1991, 1992 to 1994, 1995 to 1997, and 1998 to 2000. Differences in trends were examined for each period.
Results
A total of 339,560 hospital discharges were recorded for persons from birth to age 21 years that were associated with any psychiatric diagnosis (data not shown). The psychiatric disorder was the primary diagnosis in 58 percent of cases. Thirty-three percent of psychiatric diagnoses were for drug-related disorders; 22 percent of these were primary diagnoses. Of the 85,103 discharges (25 percent) associated with a diagnosis of an affective disorder, 76 percent were primary diagnoses. Of the 30,317 discharges (9 percent) associated with a diagnosis of ADHD, 24 percent were primary diagnoses. Of the 3,736 discharges (1 percent) associated with an autism diagnosis, 23 percent were primary diagnoses.
An overall increase was noted in the hospital discharge rate for each diagnosis. Diagnoses of alcohol and other drug use disorders were most common, increasing from 125 per 100,000 discharges (95 percent confidence interval [CI]=114 to 136 per 100,000) in 1989 to 174 per 100,000 (CI=160 to 189 per 100,000) in 2000, followed by major affective disorders, which increased from 65 per 100,000 (CI=60 to 71 per 100,000) to 155 per 100,000 (CI=134 to 177 per 100,000); ADHD, which increased from 11 per 100,000 (CI=9 to 14 per 100,000) to 53 per 100,000 (CI=45 to 61 per 100,000); and autism, which increased from 1.2 per 100,000 (CI=1 to 1.4 per 100,000) to 5.5 per 100,000 (CI=4.4 to 6.5 per 100,000). Although the discharge rates associated with diagnoses of alcohol and other drug use disorders dipped in the early 1990s, the trend for these and affective disorders were relatively parallel over the study period. Discharge rates for autism and ADHD evidenced a greater relative increase over the study period.
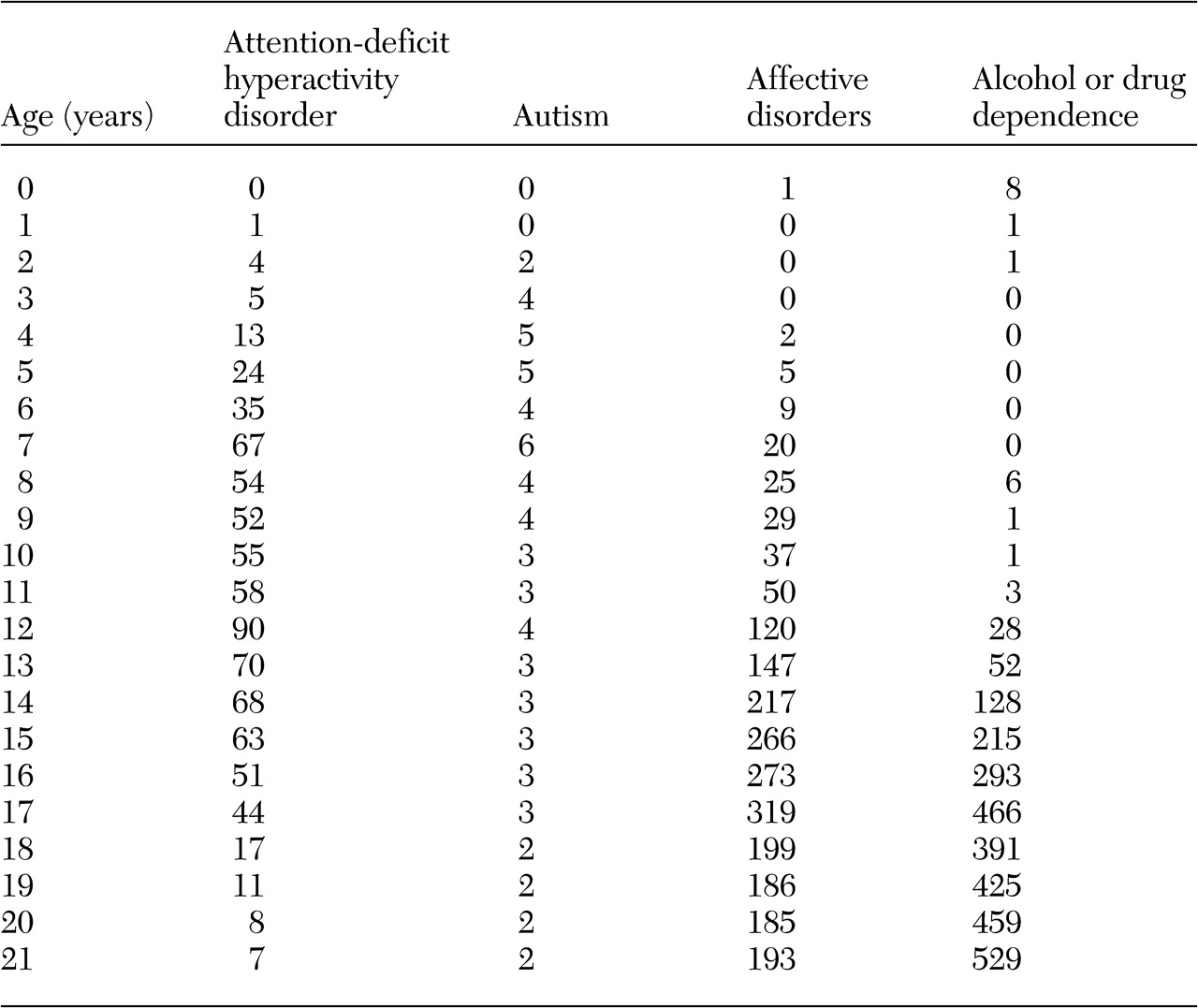
Hospital discharge rates for each diagnosis as a function of age are shown in
Table 1. Rates of diagnosis of alcohol and drug use disorder were close to zero among children up to the age of 12 years, reaching a peak of 466 per 100,000 for 17-year-olds and then peaking again at 529 per 100,000 for 21-year-olds. Rates of diagnosis of affective disorders began to increase among younger children and to increase more gradually to a peak for 17-year-olds (319 per 100,000) and decrease for 18-year-olds. Diagnoses of ADHD appeared among children around four years of age and increased gradually, peaking among seven-year-olds (67 per 100,000) and 12-year-olds (90 per 100,000) and decreasing for older individuals. Diagnoses of autism increased more sharply among young children, reaching a rate of 4.2 per 100,000 among three-year-olds and peaking at 5.9 per 100,000 among seven-year-olds. A secondary peak was observed among 12-year-olds (4.2 per 100,000).
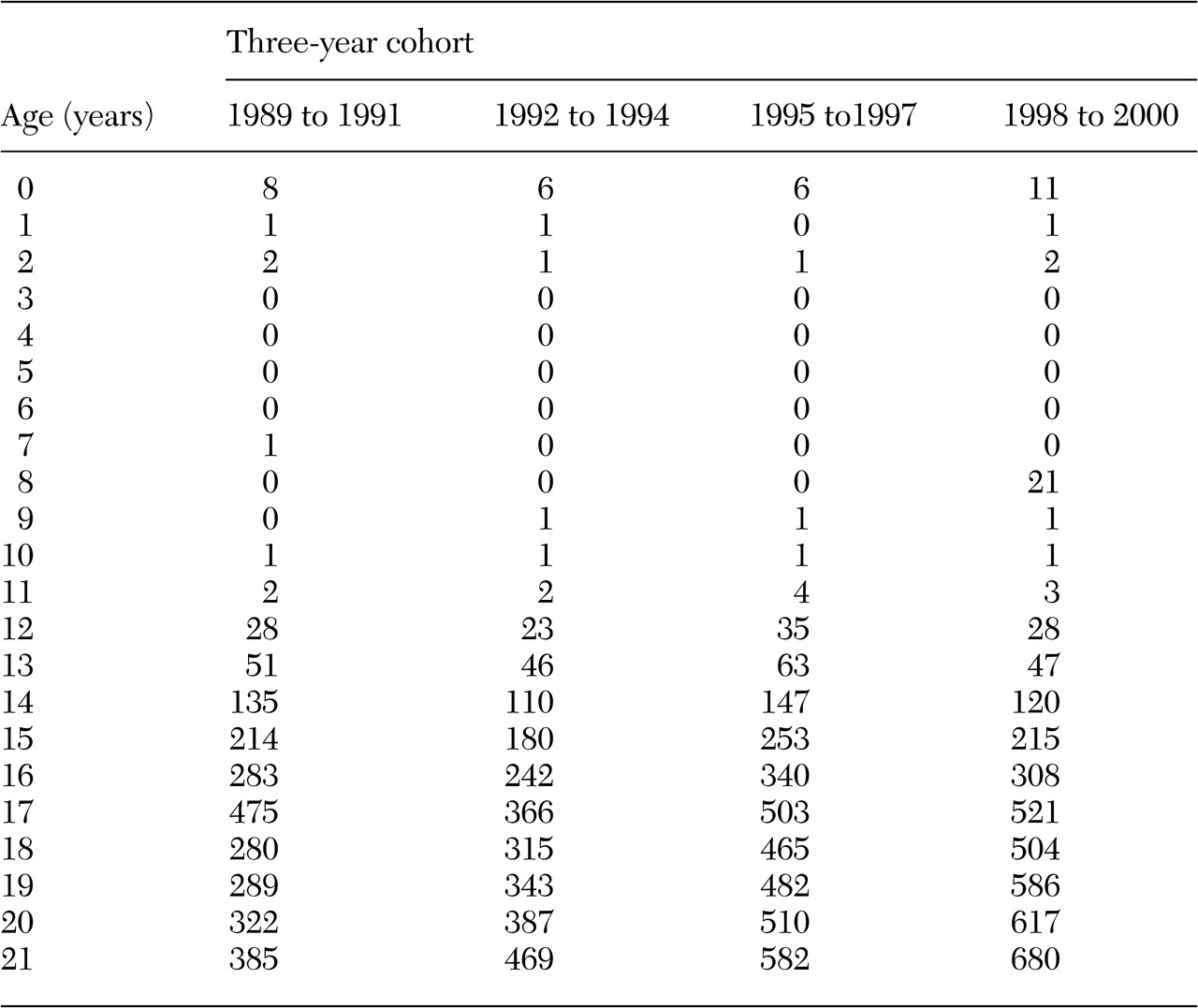
Average annual discharge rates associated with diagnoses of alcohol and other substance use disorders are shown in
Table 2. The trends for all four periods follow a relatively similar pattern, with diagnoses beginning among 12-year-olds and increasing steadily until age 21. A secondary peak was noted among 17-year-olds. The relatively small differences across each period for children and adolescents suggest that the changes observed in
Table 1 are a function of increasing discharge rates among young adults. For example, among 21-year-olds, there were 680 per 100,000 diagnoses in the period 1998 to 2000, compared with 385 per 100,000 in 1989 to 1991.
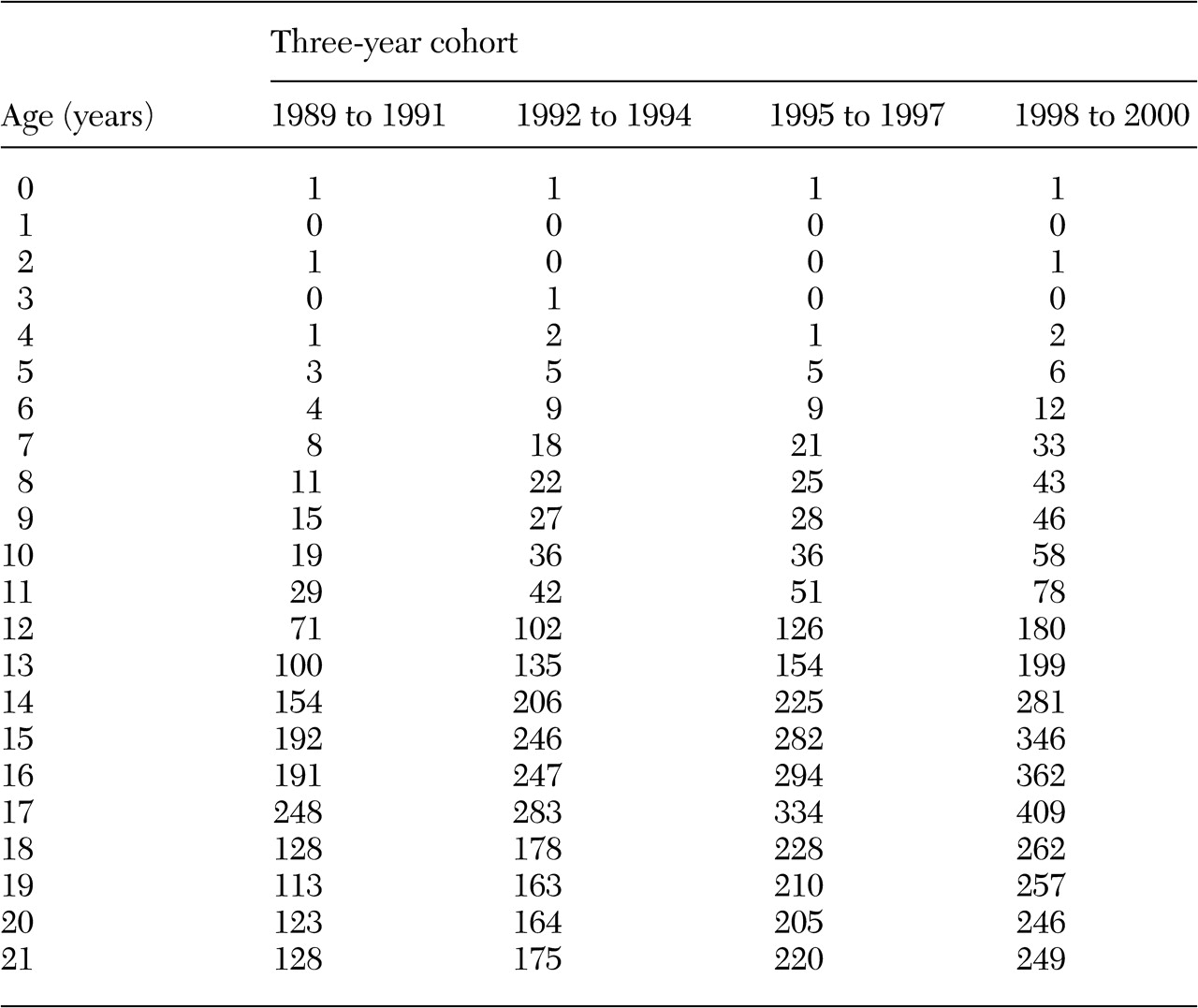
Average annual discharge rates for major affective disorders are shown in
Table 3. Children begin to have hospital discharges with an associated diagnosis of major affective disorder around the age of five years. Although all four groups followed a similar pattern across the age spectrum, increased differentiation was noted over time, with greater increases in more recent periods. Discharge rates associated with affective disorders peaked at age 17, at 409 per 100,000 in the period 1998 to 2000 and at 248 per 100,000 in the period 1989 to 1991. In all four periods, a decrease after age 17 was noted.
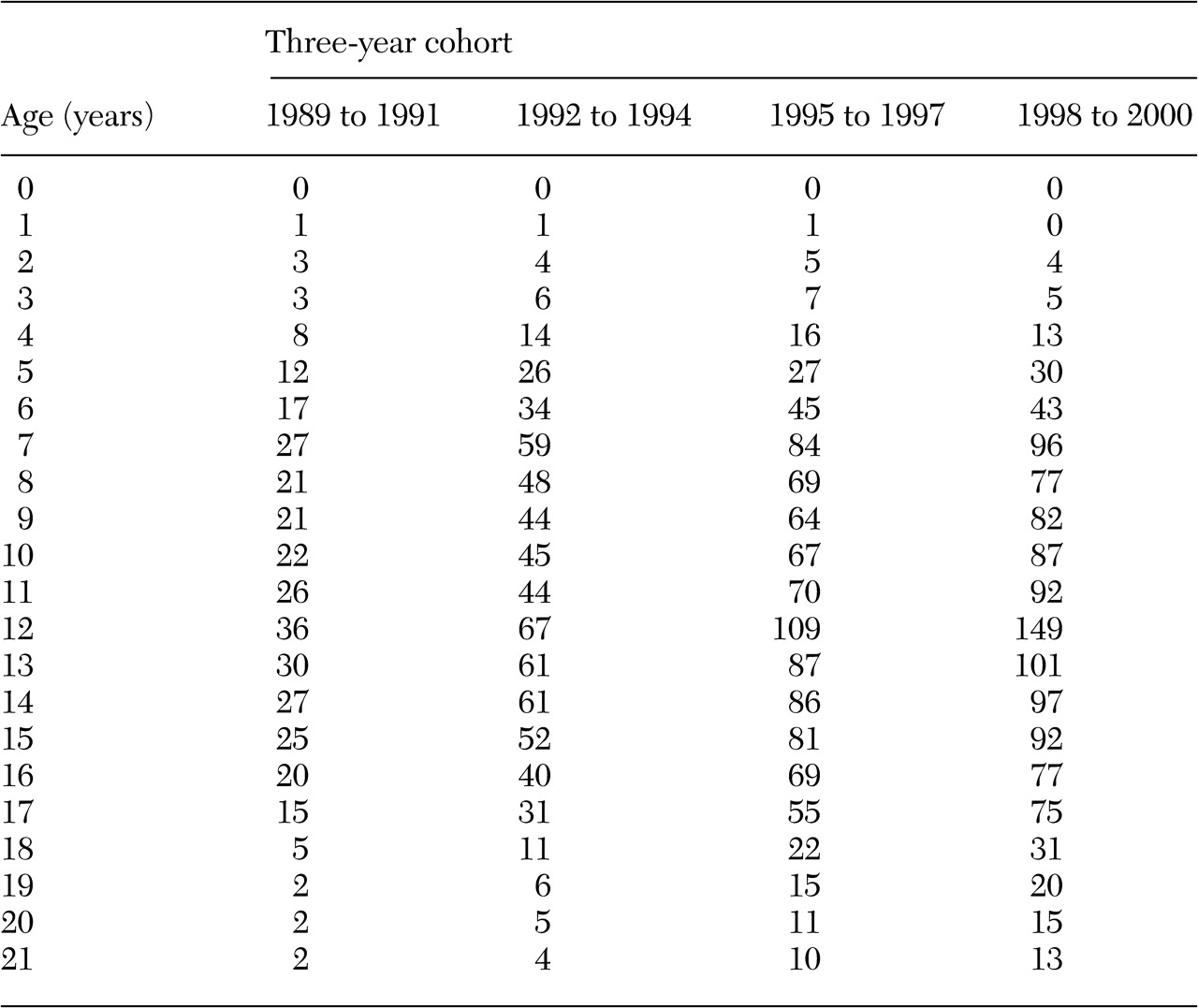
Average annual discharge rates associated with a diagnosis of ADHD are shown in
Table 4. Discharges associated with this diagnosis can be observed among children as young as two years of age, with a sharp rise until age seven; more recent periods showed a greater increase. The discharge rate for seven-year-olds was 27 per 100,000 discharges in the period 1989 to 1991 and 96 per 100,000 in the period 1998 to 2000. Rates declined among children aged seven to eight years, increased again among children aged 11 to 12, dropped again among children aged 12 to 13, and then fell more gradually to a low among 21-year-olds. This pattern was more pronounced in recent periods.
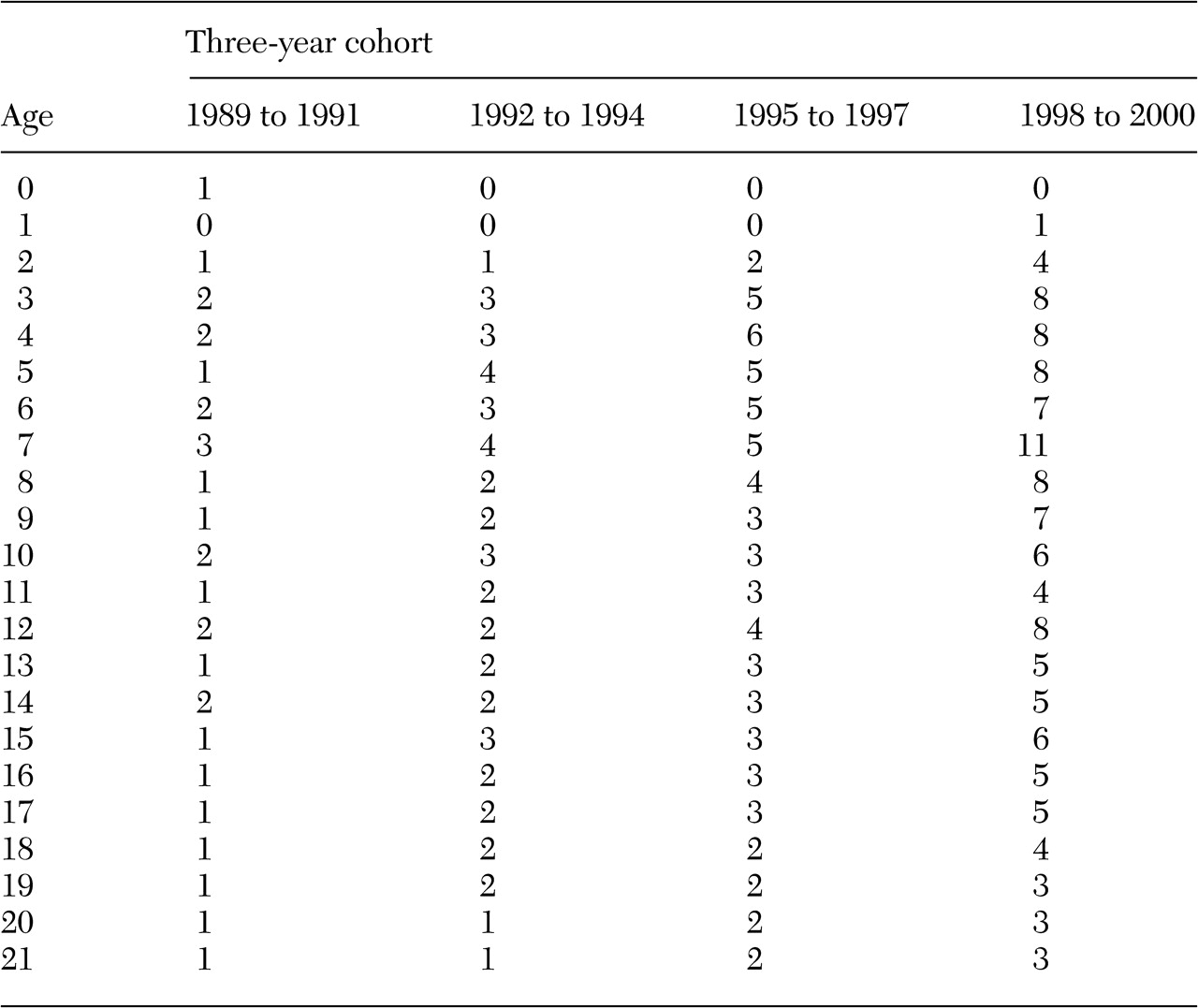
Average annual discharge rates associated with autism are shown in
Table 5. The trends by calendar year as well as by age suggest a similar pattern to that of ADHD. Discharge rates associated with autism increased sharply among children aged one to three years and again among children aged six to seven years, with greater increases in more recent periods. Among seven-year-olds, 11 per 100,000 children received a diagnosis of an autism spectrum disorder in the period 1998 to 2000, compared with three per 100,000 in 1989 to 1991. Rates then dropped among children aged seven to 11, with greater decreases in more recent years. Another increase was seen among children aged 11 to 12 years, with another drop from age 12 to 13. Among 12-year-olds, eight per 100,000 children were given a diagnosis in the period 1998 to 2000, compared with two per 100,000 in the period 1989 to 1991. By young adulthood, there was less differentiation by period in the proportion of hospital discharges.
Discussion
This study provided evidence of increasing hospital discharge rates for several psychiatric disorders between 1989 and 2000. Although substance-related and affective disorders were more common, the increase was more pronounced for ADHD, which evidenced a 381 percent increase over the study period, and autism, which evidenced a 358 percent increase. Increases were observed in successive periods for all disorders. Diagnoses of ADHD and autism showed peaks among seven- and 12-year-olds. In contrast, substance-related and affective disorders showed gradual increases in discharge rates, peaking among 17-year-olds.
As expected, the rates of diagnoses among individuals being discharged from a hospital were lower than community prevalence rates. Survey data suggest that between 20 and 40 percent of adolescents have been drunk in the past 30 days, and between 4 and 12 percent have used hallucinogens, narcotics, or cocaine in the past 30 days (
28). Although these percentages are overestimations of the proportion of youths who would qualify for a diagnosis of substance abuse or dependence, the numbers suggest that the maximum rate of .5 percent found in this study is an underestimation. Likewise, the highest estimate of affective disorders in this population was .4 percent, whereas estimates of affective disorders among children have been between 3 and 8 percent (
29,
30). The prevalence of ADHD is between 3 and 5 percent (
10,
11) and of autism is between .2 and .4 percent (
14). These data provide underestimations of community prevalence, but it appears that the underestimation is not dissimilar across disorders.
One might expect that hospitalization rates would be higher among older children, especially in the case of chronic conditions. This was the general pattern for affective and substance-related disorders. However, rates of diagnosis of autism and ADHD were highest among seven- and 12-year-olds, with rates dropping between ages seven and 12 and again after age 12. It is unlikely that related symptoms decreased between these ages. Rather, it is likely that certain events precipitate the association of a diagnosis of autism or ADHD and a hospital discharge. For example, the peaks among seven- and 12-year-olds suggest that transitions into elementary school or into middle school are associated with increased rates of diagnosis.
The finding that hospital diagnoses of mental disorders are increasing across the age span in more recent years has several possible interpretations. Increased rates of diagnosis of all disorders over time suggest increased ascertainment, perhaps due to increased awareness of disorders or changing practice patterns. The fact that a greater increase in diagnoses of developmental disorders among younger children was observed in the more recent periods suggests the possibility of increased community prevalence. A third possibility is that children with developmental disorders are more likely to be hospitalized than are other children.
Increased ascertainment
A MEDLINE search using the term "attention deficit disorder" returned 185 articles in 1989 and 541 in 2000. A search that used the term "autistic disorder" returned 216 articles in 1989 and 359 in 2000. Increased awareness was not limited to the medical literature. A NEXIS search of all U.S. news outlets found 25 articles on ADHD and autism in 1988 and 838 articles in 2000. Popular awareness may have consequently increased, fueling parental concern and, in turn, changing physicians' behavior (
31). Concurrently, treatments for developmental disorders have become more widely accepted and used. More children with a diagnosis of ADHD (
32) as well as younger children with this diagnosis (
33) are treated with stimulants. Likewise, children with autism are increasingly treated with stimulants and neuroleptics (
34). The increasing popularity of these treatment options may increase the likelihood that providers will assign a related diagnosis.
Another possible reason for changing ascertainment is the expansion of Supplemental Security Income (SSI) and the Individuals With Disabilities Education Act (IDEA), which may have provided incentive for physicians to diagnose ADHD and autism. The number of children insured through SSI increased by more than 400 percent between 1988 and 1997 (
35), in large part because of the Social Security Administration's broadened definition of disability to include mild mental retardation and mental illness.
Concurrently, the number of children served by IDEA grew from 4.5 to 6.3 million between 1988 and 2000 (
36). The categories of both autism and "other health impairment," which includes ADHD, grew by more than 1,000 percent during this time. In 1990, IDEA was expanded to include early intervention services for children aged three to five years (
36). School systems were required to implement new systems for screening and diagnosis, which may have increased the number of children receiving a diagnosis.
Increase in community prevalence
Byrd and colleagues (
18) suggest that changes in diagnostic practices cannot explain the rise in diagnosis of autism. Several etiologic pathways for this increase have been posited. One hypothesis is an increase in exposure to environmental toxins, such as mercury (
3,
37,
38). A second is an increase in viral loads associated with measles, mumps, and rubella (MMR) vaccines. The association between increasing rates of both MMR vaccination and autism has been noted (
17), but evidence of causality is limited (
4,
39). Recent studies indicated no association between MMR vaccination and autism (
40,
41,
42), and limited data are available on the risk of neurodevelopmental disorders associated with thimerosal exposure (
41). A second possibility relates to the increasing survival rate of low-birth-weight and otherwise compromised babies, who are at increased risk of developmental disorders (
43). From 1989 to 1997, rates of mortality among preterm infants decreased by more than 30 percent (
44). However, it is unlikely that the increase in the number of low-birth-weight babies alone could account for a large change in rates of developmental disorders.
Increase in prevalence of hospitalization
A number of studies have shown that children with developmental disorders use more health care services than other children (
45,
46). Although hospitalization rates for the general population remained constant from 1983 to 1991, rates of hospitalizations for persons with developmental disabilities increased by 56 percent (
47). This change could not be accounted for by an increase in the number of persons with developmental disabilities and occurred at the same time as a reduction in hospital admissions for pediatric injury (
48,
49) and stable rates of admission for asthma (
50) and influenza (
51).
Gallaher and colleagues (
52) found that having a developmental delay was independently associated with hospitalization, even after other health conditions had been controlled for. They also found that children with developmental delays were twice as likely as other children to have other chronic health conditions. Children with both developmental delay and another chronic health condition were much more likely to be hospitalized than other children, and, unlike the effect of having a chronic health condition only, this difference persisted over the first five years of life. Increased probability of hospitalization among children with developmental disabilities may partially account for trends observed in this study.
Limitations
Some limitations of this study should be mentioned. As with any administrative data source, the HCUP is subject to coding errors (
53). If these errors were differentially biased by disorder, or error rates changed over time, it would bias comparisons within or among diagnoses. Second, it is possible that although individuals with psychiatric disorders presented at hospitals in the data set, psychiatric diagnoses were not assigned. It may be that when presenting problems are more directly related to the mental disorder—for example, intoxication and substance use or self-injury and depression—the disorder is more likely to be coded. This dynamic might lead to underreporting of rates of diagnosis of ADHD and autism relative to other disorders. A related limitation is that for approximately three-quarters of individuals with a diagnosis of an affective disorder, ADHD, or an autism spectrum disorder, the diagnosis was secondary to some other morbidity. Primary diagnoses were not examined in these cases and may have been differentially associated with the assigned secondary diagnosis. Third, because this study used only inpatient hospital data from specific types of hospitals, the results may not be generalizable to other health care settings. Fourth, the hospitalization data do not include long-term psychiatric and drug treatment facilities, so individuals with alcohol and drug dependence are probably underrepresented. The number of such specialty hospital facilities have also been declining in recent years, and few children are admitted to these types of facilities, so it is difficult to ascertain exactly what bias the exclusion of the facilities may have on our results.
Conclusions
Regardless of the reason for the observed increase, the results of this study suggest that increasing rates of diagnosis of autism and ADHD at hospital discharge are not occurring in isolation but, rather, in the context of increasing rates of diagnosis of a number of disorders. Although it is possible that the community prevalence of various psychiatric and developmental disorders is increasing, it is important to consider variables such as changes in relevant policies, increased awareness, and changes in practice patterns that may also be causally related to these increases.