Insurance cost-sharing requirements raise special concern when the enrollee has schizophrenia. Persons with schizophrenia are disproportionately poor, have limited opportunities for employment, and are dependent on public programs for access to specialty mental health services (
1,
2,
3,
4). In low-income patient populations, greater cost-sharing can lead to substantially less use of preventive services (
5,
6) and prescription medications (
7,
8) and can adversely affect patients' clinical outcomes (
9,
10,
11). In addition, patients with schizophrenia often have limited or inconsistent contact with the treatment system; thus any financial barrier may discourage them from remaining in regular contact with providers.
For these reasons, Medicare enrollees with schizophrenia are particularly vulnerable. Medicare requires up to 50 percent patient cost-sharing for most outpatient mental health services, provides little or no coverage for case management and community-based psychosocial rehabilitation services, and will not provide prescription drug coverage until 2006 (
12). Although approximately 56 percent of Medicare enrollees with schizophrenia have additional insurance coverage through Medicaid (
13), which requires relatively little cost-sharing and covers case management, rehabilitation, and medication, many do not. These patients must rely on other sources—private or other public coverage, public subsidies, or personal assets—to cover the cost of mental health services.
The effects of cost-sharing requirements on access to mental health services among Medicare enrollees with severe mental illness are not well documented. The two previous studies that provided information on this issue had significant limitations (
13,
14). First, they did not include use of case management, rehabilitation services, or second-generation antipsychotic medications, which are more expensive than first-generation antipsychotics (
15). Medicaid coverage may substantially increase access to these treatments, which are not covered by Medicare. Second, previous studies' results were based on patient self-report or Medicare claims. Self-reports for persons with schizophrenia are subject to underreporting of utilization (
16), and Medicare claims may omit utilization when reimbursements come from other insurers or when services are subsidized through sources other than insurance. Third, previous studies could not control for differences in clinical symptoms and other personal characteristics that may have been related to the probability of using services.
In particular, Medicaid administratively limits eligibility with a cap on total household income and assets, whereby the income of spouses and other relatives living in a consumer's household count against the cap. In contrast, eligibility for Medicare before age 65 implies enrollment in the federal Social Security Disability Insurance (SSDI) program. Similar to Medicaid, SSDI eligibility requires being work disabled and maintaining monthly earnings below a level of approximately $750, but SSDI does not place a cap on household income or assets. Thus the incomes of many nonelderly Medicare enrollees with schizophrenia are too high for them to qualify for Medicaid coverage despite being chronically disabled and despite having substantial medical need.
Methods
The data used here were from the U.S. Schizophrenia Care and Assessment Program (SCAP), a large-scale naturalistic observational study of adults in treatment for schizophrenia in six states.
SCAP patient recruitment
Using administrative records provided by the six participating regional treatment sites, we identified patients who were aged 18 years or older and had a current diagnosis of schizophrenia, schizoaffective disorder, or schizophreniform disorder on the basis of DSM-IV for possible recruitment into the study. From these lists, approximately 400 patients at each site were randomly selected and enrolled. Patients also had to be able to provide informed consent, to not have participated in a clinical trial in the 30 days before enrollment, to have sufficient ability to communicate in English, to agree to participate in all tests and examinations required by the study protocol, to be accessible by telephone or mail, and to anticipate remaining available for follow-up. Informed consent was obtained from patients, and approval was obtained from an institutional review board at each treatment site.
SCAP treatment sites
Organizations in the following cities and states participated in the study: West Haven, Connecticut; Orlando, Florida; North Carolina (encompassing the Durham-Chapel Hill area as well as several rural counties in the north-central region of the state); Baltimore, Maryland; San Diego, California; and Colorado (encompassing four counties in the Denver area). All sites included public providers of mental health services or private providers who had contracted with state or local government agencies to provide "open access" to public services. Patients were recruited from various treatment organizations located within these sites, including psychiatric outpatient clinics and inpatient facilities located at teaching hospitals, Department of Veterans Affairs medical centers, community mental health centers, private outpatient mental health service organizations, day treatment programs, homeless shelters, psychosocial rehabilitation programs, and a state psychiatric hospital. Service use data were collected from the recruitment organization as well as from other provider organizations in the community.
Sites had to meet certain requirements: the capacity to provide electronic patient service use information by using site management information systems, the regular provision of an array of mental health services, a relatively large patient population (to facilitate recruitment), an open formulary or administratively unrestricted patient access to first- and second-generation antipsychotic medications, involvement of a multidisciplinary staff in SCAP data collection and management, and the presence of a site principal investigator with a national reputation in schizophrenia research. Among sites that met these requirements, sites were ultimately selected with the purpose of obtaining diversity in racial or ethnic composition, geographic location (both rural and urban), and system features (for example, acceptable types of insurance coverage, managed care involvement, and number and size of participating mental health service organizations).
Sample selection
Baseline data for all 2,328 SCAP participants were collected between July 1997 and January 2001. Data collection continued until March 2003. After a baseline interview, participants were followed up at six-month intervals for up to 36 months. Of the 2,328 participants, 91.5 percent completed at least one six-month follow-up. Because of late recruitment into the SCAP, 30-month follow-ups were not attempted for 96 consumers, and 36-month follow-ups were not attempted for 260 consumers.
Of the 2,328 participants, 1,259 nonelderly (younger than 65 years) consumers who had Medicare coverage were selected. Elderly consumers were excluded, because for them work disability is not a requirement for Medicare eligibility. Of the remainder, 53 consumers were excluded because they did not complete at least one follow-up assessment after baseline. Also, 98 consumers known to have incomplete medical record information were excluded. In these cases, administrative barriers—for example, as a result of a consumers' switching to a new provider or becoming incarcerated—prevented full access to records. Finally, 17 consumers with missing values for other covariates were excluded, leaving a sample of 1,088 consumers who had a combined 3,808 assessments, including the baseline interview and follow-up assessments, or approximately 3.5 assessments per person.
Measures
Service use. Data on service use were collected through a review of medical records obtained from organizations that provide mental health services. Possible service locations were identified by site managers and consumers. Locations included specialty mental health care providers as well as medical service providers (such as emergency departments) and community organizations (such as homeless shelters). Possible service locations were visited at six-month intervals to obtain medical records. All consumers provided their informed consent for record collection.
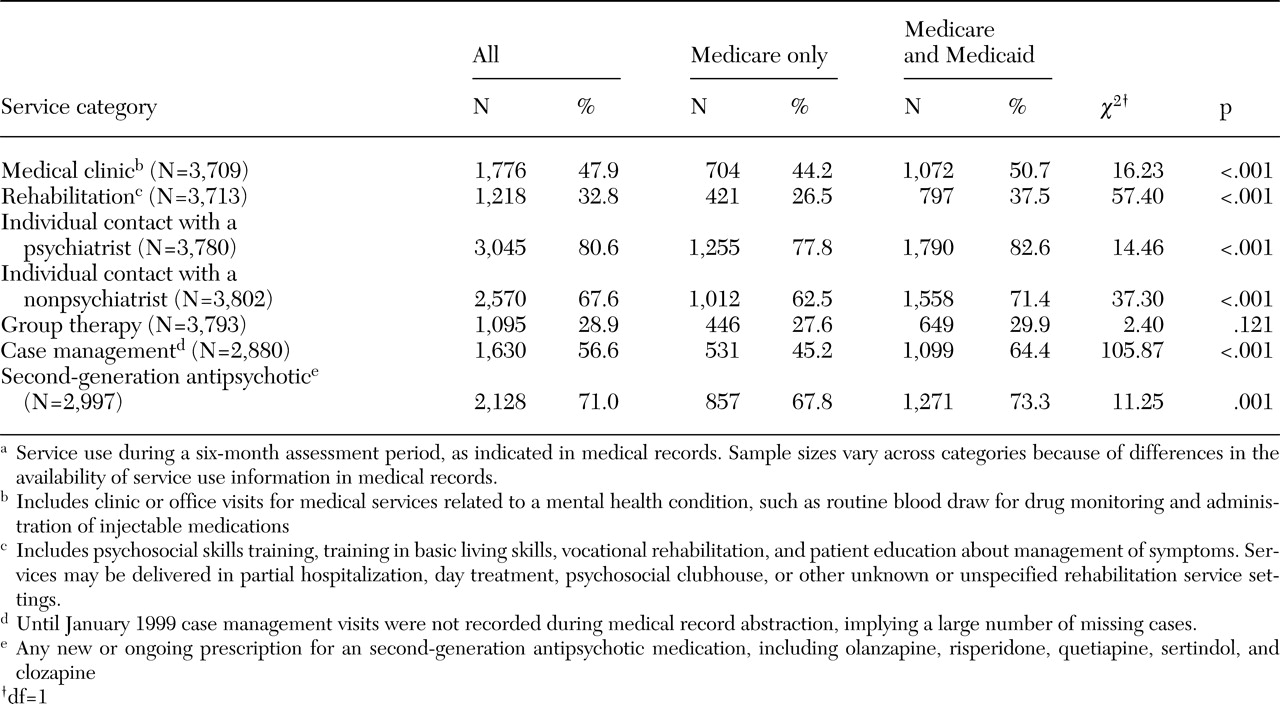
A dichotomous indicator was created for any service use in a six-month period for each of seven outpatient treatment categories: medical clinic visits for a mental health problem, rehabilitation services, group therapy, individual contact with a psychiatrist, individual contact with a nonpsychiatrist therapist, case management, and use of a second-generation antipsychotic medication. The medical clinic category included clinic or office visits for medical services related to a mental health condition, such as routine blood draw for drug monitoring and administration of injectable medications. The rehabilitation services category included psychosocial skills training, training in basic living skills, vocational rehabilitation, and patient education programs. Rehabilitation services obtained during day treatment, partial hospitalization, residential care, and other service settings were included. Individual contact with a psychiatrist included both individual psychotherapy as well as medication management. Use of a second-generation antipsychotic was indicated by the presence of a new or ongoing prescription for olanzapine, risperidone, quetiapine, sertindol, or clozapine. Assessments involving the use of first-generation antipsychotic medications only were grouped with 64 cases involving no use of an antipsychotic medication. Exclusion or inclusion of the latter cases from analyses did not influence results.
Insurance coverage. Insurance status was self-reported at each six-month assessment. It was assumed that persons who reported the same insurance status at both the beginning and the end of the period maintained that insurance status throughout the period. Because of missing information and changes in insurance status from the beginning to the end of the assessment period, insurance status was imputed in 869 of the 3,808 assessments on the basis of insurance status reported at either a previous or a subsequent interview. The purpose of imputation was to minimize sample exclusions in cases in which insurance status was missing or changed during the period. In cases in which insurance status changed, imputation was a random selection of insurance status at either the beginning or the end of assessment. All results reported below were checked for sensitivity to exclusion of the cases with imputed insurance status. Exclusion of these cases did not qualitatively influence the results and had at most a small influence on the estimated magnitudes of the effects of insurance status.
Analyses
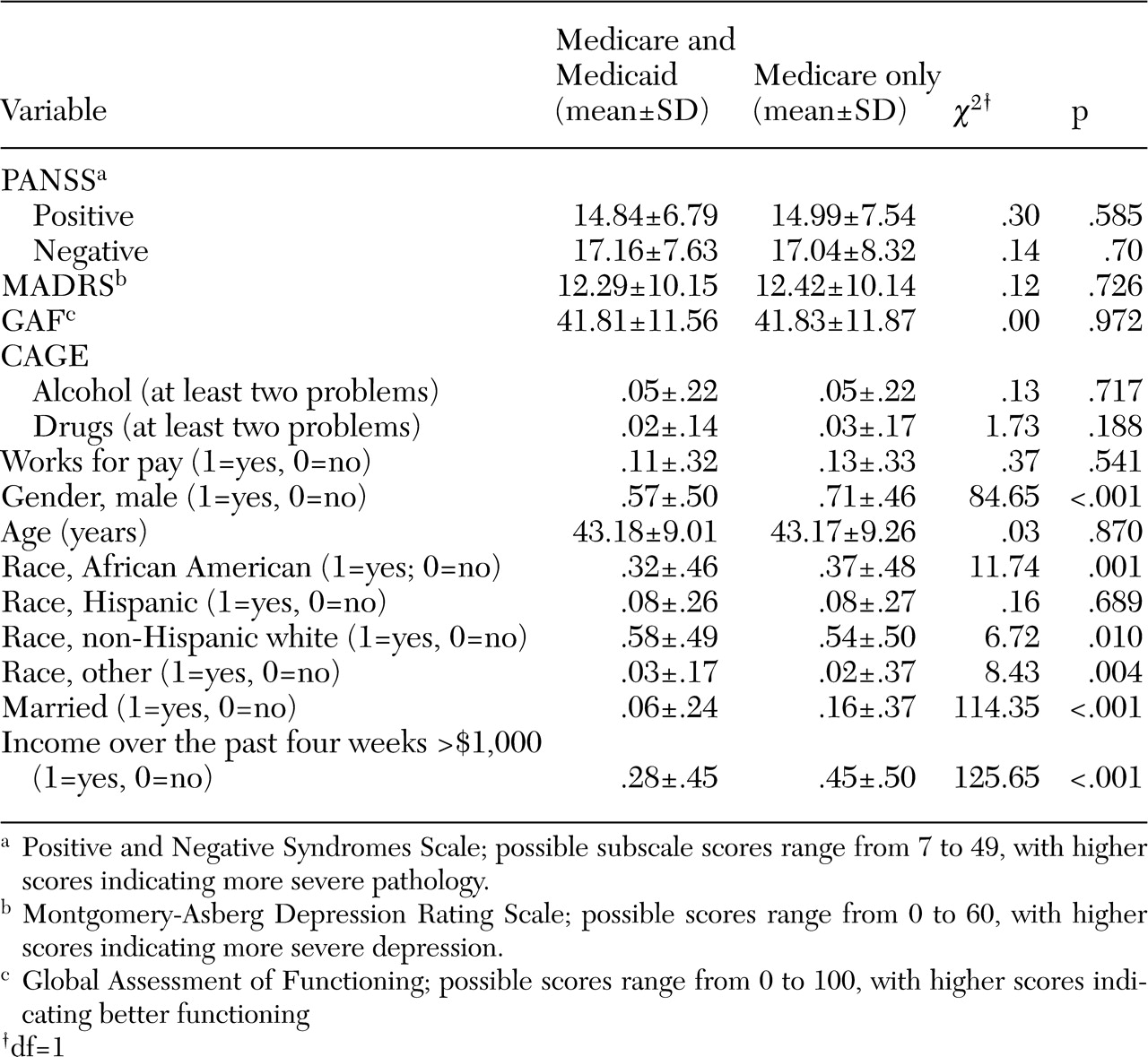
If dually insured and other Medicare enrollees differ in their average propensity to use services, unadjusted comparisons of service use by insurance status will be misleading. For example, it is possible that Medicaid enrollees are more severely ill on average, which implies relatively greater use of services. To check this possibility, we first compared the groups, by using chi square test statistics for group mean differences, in terms of symptoms of mental illness (scores on the Positive and Negative Syndrome Scale [PANSS] and the Montgomery-Asberg Depression Rating Scale [MADRS]) (
17,
18), functioning (percentage working for pay and Global Assessment of Functioning [GAF] score), and dependence on alcohol or controlled substances. The latter measures were defined as at least two symptoms on the alcohol or illegal substance CAGE indices (
19,
20). These comparisons were based on the presumption that service need is positively related to symptom levels and substance dependence and is negatively related to level of functioning.
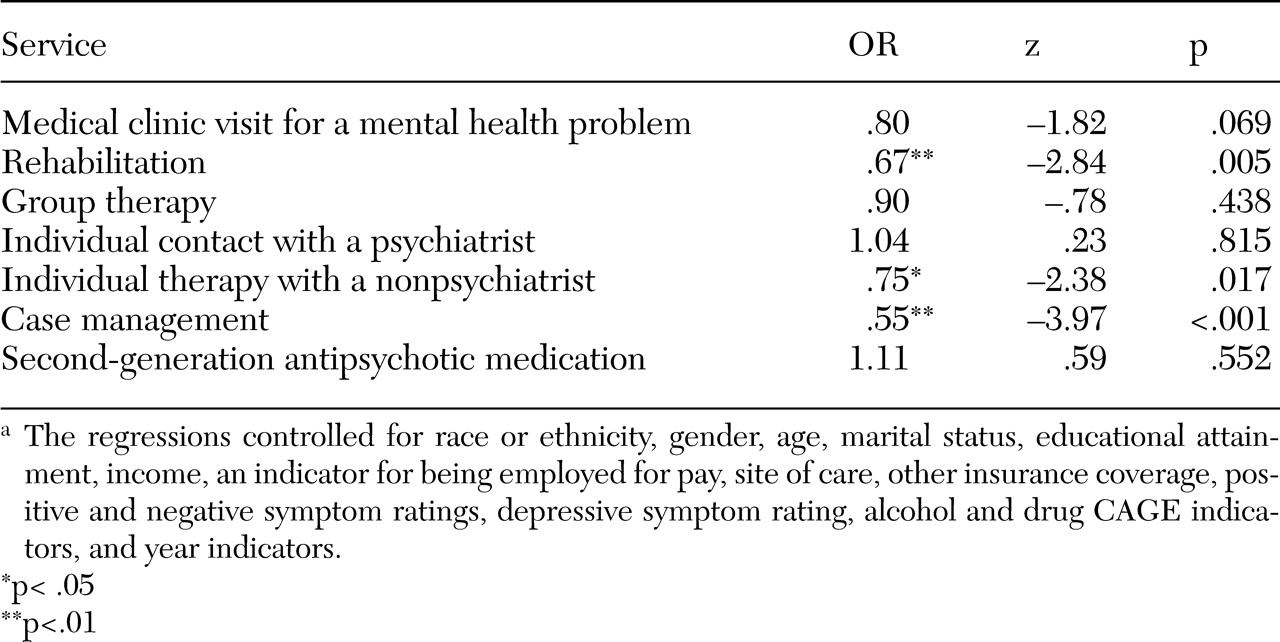
Logistic regressions were estimated for any service use in a given category in a six-month period. The regressions controlled for absence of Medicaid coverage (Medicare only) and for factors that may be correlated with the likelihood of using services: symptoms (PANSS and depression ratings), age, race or ethnicity, marital status, educational attainment, income, employment status, and drug and alcohol dependence (CAGE scores). The regressions also controlled for indicators of study site and year, to control for geographic and over-time variation in factors influencing service use.
Service use regressions used data from all available six-month assessment periods. The availability of repeated measures for the same individual implied that measures may have been correlated across observations for the same individual, which could result in biased variance estimates. Robust Huber-White variance estimates (
21,
22,
23) were used to account for correlated observations. An advantage of the Huber-White variance estimator compared with other methods is that it is robust to multiple forms of correlation within groups. No sampling weights were used in the analysis. However, higher rates of loss to follow-up resulted in significantly smaller samples at three of the six recruitment sites (Colorado, Baltimore, and San Diego).
Discussion
The results of this study suggest greater problems with access to rehabilitation services, case management, and individual contact with nonpsychiatrist therapists among Medicare enrollees with schizophrenia who lack Medicaid coverage compared with those enrolled in Medicaid. In particular, those who lacked Medicaid coverage were 33 percent less likely to use rehabilitation services, 25 percent less likely to have individual contact with nonpsychiatrist therapists, and 45 percent less likely to receive case management in a six-month period, with symptoms, substance dependence, gender, age, income, and other factors controlled for. No significant differences in probability of use over a six-month period were found for medical clinic visits for a mental health problem, group therapy, individual contacts with psychiatrists, or receipt of second-generation antipsychotics.
Our findings contrast with those of previous studies that have compared service use among Medicare enrollees with schizophrenia by Medicaid enrollment. Using data on Medicare claims, Dixon and colleagues (
13) found that over the course of a year persons who did not have Medicaid coverage were significantly less likely to receive group therapy and psychiatric somatotherapy (medication management) but were significantly more likely to receive individual therapy. In addition, Yanos and colleagues (
14) found that the proportion of Medicare enrollees who used individual therapy, group therapy, or family interventions did not differ by Medicaid enrollment. However, the latter study's use of a relatively small sample (N=257) may have made detection of significant differences in service use problematic. Differences between our results and those of previous studies may also be related to the availability in this study of a rich set of controls for differences in consumer symptoms, other individual characteristics, and site-of-care indicators and to the use of medical records abstracts, which may have provided a more complete record of service use.
The finding that there was no difference by Medicaid enrollment in the proportion of patients who received second-generation antipsychotics at any of the six study sites also deserves comment, given that Medicare does not currently cover prescription medication, and given that the prices of second-generation medications are substantially higher than those of first-generation medications (
15), and given that providers are generally required by law to seek payment in full for customary charges associated with services rendered to patients. However, our finding is consistent with the existence of public programs that provide free access to medications for persons with low incomes and with the fact that providers often maintain limited supplies of free samples. It is also important to note that SCAP participants were recruited from provider organizations and thus probably had better access to medication than is typical for other Medicare enrollees with schizophrenia. Providers at two of these organizations reported (upon inquiry) that samples of antipsychotic medications provided to the organizations by pharmaceutical sales representatives are regularly stockpiled and are later distributed free of charge to financially needy patients. It is unknown whether these organizations had a sufficient stockpile of free samples to account for our finding of no association between Medicaid enrollment and type of antipsychotic used. Thus the impact of free samples on antipsychotic use under various types of insurance coverage is one interesting avenue of future research.
The finding that, after other factors were controlled for, there was no significant association of Medicaid coverage with the probability of individual contact with a psychiatrist, group therapy, or medical clinic visits for mental health problems could be related to several factors. First, Medicare provides at least partial coverage for these services. Second, patients could have considered contacts with a psychiatrist to be less discretionary than use of other services—for example, vocational rehabilitation—at least over a six-month period. Third, local subsidies could have covered out-of-pocket costs associated with use of these services, whereas subsidies might not have been sufficient to cover the cost of case management services, therapy with nonpsychiatrists, and rehabilitation services.
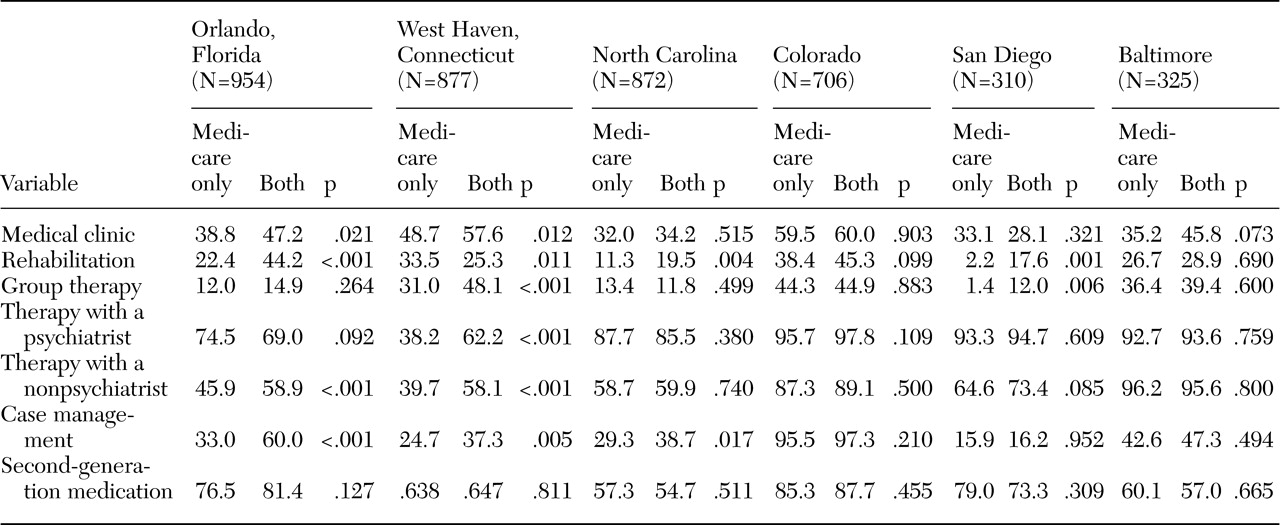
The possibility of significant differences in local subsidies for out-of-pocket costs associated with specialty mental health service use is consistent with the substantial variation across sites in the association between Medicaid enrollment and use of mental health services in this sample (
Table 3). In principle, the potentially positive impact of Medicaid on receipt of treatment is attenuated in states that more generously subsidize out-of-pocket costs for consumers who do not have Medicaid. However, the effects of local financing on access are difficult to pin down because of the difficulty of obtaining precise measures of the financing availability for different types of services in various locations.
Our sample and analyses had several potential limitations that deserve comment. First, comparison of sample characteristics by Medicaid enrollment (
Table 1) did not suggest observable differences in service need. Instead, Medicaid enrollment was related to administrative factors including income eligibility: consumers with Medicare but not Medicaid were 61 percent more likely to have total monthly incomes exceeding $1,000, an approximate indicator of Medicaid ineligibility, and were 176 percent more likely to be married, suggesting access to additional sources of income and assets that may have made them ineligible for Medicaid.
Second, it is possible that managed behavioral health care arrangements influenced our results. In particular, cost-sharing may matter more in an unmanaged fee-for-service insurance system, because managed care provides an alternative mechanism for rationing access to care. Nevertheless, sensitivity analyses that excluded observations from two sites where Medicaid enrollees were required to gain access to services through contact with a managed behavioral health care organization (San Diego and Colorado) did not qualitatively alter the findings.
Third, it is possible that service use could have increased the probability of Medicaid enrollment, because the process of enrollment into Medicaid often begins at provider organizations after use of services. It is unlikely that this factor was critical to the results, because all consumers were receiving treatment at the time of recruitment, and more than 98 percent of consumers in both insurance groups used at least one category of service every six months. Nevertheless, reverse causation may have increased the magnitude of the estimated associations with insurance coverage.
Fourth, it is possible that nonfinancial economic costs associated with service use were lower for consumers with Medicaid, and this may explain observed insurance-group differences. Medicaid provides a relatively structured system of reimbursement for publicly subsidized care, whereas obtaining other local subsidies may involve greater stigma, inconvenience, or red tape. This difference may have contributed to the relatively low probabilities of service use among Medicare-only patients, even when consumers received free care. However, we cannot measure these effects directly and leave this topic to be explored in future studies.
Finally, although the comparison of rates of six-month service use suggest that Medicare enrollees with schizophrenia who do not qualify for Medicaid may have less access to certain mental health care services, this study provided little or no evidence on the consequences of having less access for patients' health outcomes or quality of life. Simple comparisons of sample means for the clinical characteristics of the two subgroups (
Table 1) suggest that the groups were similar in terms of schizophrenia symptom (PANSS) score ratings and GAF ratings of functioning, which could be interpreted as evidence that differential access to services had no impact on patients' health outcomes.
However, any such interpretation requires extreme caution. The results of this analysis demonstrate only a cross-sectional association between greater generosity of insurance coverage (represented by Medicare plus Medicaid compared with Medicare only) and greater rates of six-month use of services, particularly case management, rehabilitation services, and individual therapy with nonpsychiatrist providers. In principle, greater frequency of contact with outpatient health care providers—that is, greater continuity of care—is a desirable objective for the treatment of patients with schizophrenia (
24).
Whether these utilization differences resulted in differential health outcomes is unknown. To test that proposition would require, at a minimum, more precise and detailed data on the quality and type of services, the intensity of service use, and health outcomes. The SCAP data set did not contain precise and reliable measures on all of these dimensions. Thus although the results of this study are provocative, further research is needed to illuminate the clinical significance of limitations in Medicare coverage of outpatient services among patients with schizophrenia.