Results
Case Number One
The patient is a 21 year-old male college student. He is the older of two siblings. He presented with symptoms of panic attacks, which had begun more than three months prior to the interview and which had been unresponsive to SSRI medications. The patient came from an intact family with supportive and loving parents. The one psychotrauma in his history involved the death of his beloved uncle (his mother’s brother) from human immunodeficiency virus. The patient’s mother suffered greatly from grief after her brother’s death, and her depression affected the patient. He developed symptoms of severe anxiety upon the possibility of sexual intimacy in relationships. The patient was diagnosed with unresolved loss both for his grief and secondarily to his mother’s bereavement.
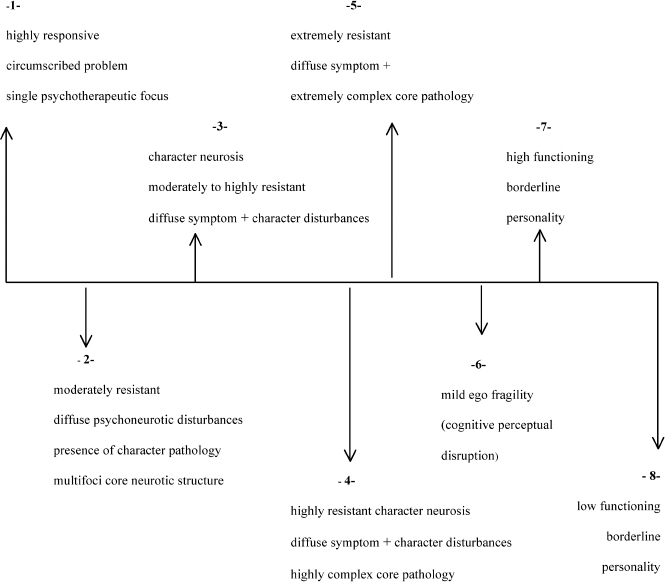
Predicted Category Placement Indices for unresolved/disorganized attachment observed during the clinical interview were: disorganization with respect to time (referencing different times when loss occurred), prolonged silences, unfinished sentences, and eulogistic speech. His defenses were seen as organized against vulnerability (perfectionism, repression, defiance, instant repression [empty head], humor; he would ignore or smile in response to the therapist’s interventions. He projected his fear about the loss of his uncle onto his mother and others (not wanting to “conjure up” negative feelings in the other). Anxiety manifestations observed were striated muscle tension (head to toe), sympathetic reactions (hypervigilance, increased heart rate, shallow breathing), and some mild parasympathetic reactions (stomach aches). This patient was diagnosed with panic disorder without agoraphobia. The position on Davanloo’s Spectrum of Psychoneurotic Disorders was 3.
On the whole this individual exhibited signs of secure-autonomous state of mind (good observing ego with correct labeling of anxiety and some instances of metacognitive monitoring), though he exhibited some signs of a dismissing state of mind (idealization of the father, restricted in feeling, and insistence of a lack of memory at moments when confronted with sadness). The main classification was assigned to unresolved/disorganized with respect to the loss of his uncle, with emergent properties of secure-autonomous state of mind, and some instances of dismissing state of mind (U/F/Ds). It should be noted here that subclassifications were not assigned for this case due to the authors’ initial attempts to work out a system of analysis that would capture the main classification only (once the authors became comfortable with the system of analysis for the first case, subclassifications were assigned for the remaining cases).
Assessed Character Assignment In Erik Hesse’s analysis, the main category U/d was likewise for the loss of the uncle due to lapses in reasoning (confusion surrounding the loss). The secondary placement of Cannot Classify (CC) was because a single strategy did not seem to prevail. (While Dr. Hesse considered the text to be globally closest to secure (F), there were too many examples of D-like instances of expressions of strength, normalcy, and “not caring” for the AAI transcript on the whole to be considered secure; likewise there were too many topics and responses in the AAI transcript that were unexplained.)
In this first case the authors attempted to analyze via the clinical interview, the CC classification should have been made following the U/d classification for the same reason noted by Dr. Hesse—a single strategy did not seem to predominate. The reason for this omission was simple error on the part of the authors while working out a method of analysis using the AA-CRS. The final classification, including subclassifications, rendered by Dr. Hesse was U/CC/F2/F4/Ds3.
Case Number Two
The patient is a 60-year-old retired male engineer suffering from panic disorder, agoraphobia, hypochondria, and atypical depression. He had Hodgkin’s disease when he was in his 40s and his heart valve had been damaged by radiation treatment. The patient became anxious when considering the possibility that he might need a heart valve replacement at some future time. He became progressively more housebound and more hypochondrical, with unrealistic fears of physical activity. He was clingingly link-dependent on his wife for safety. As a child he was favored by his mother as “the golden child,” and he transferred this dependency from his mother onto his wife.
Predicted Category Placement Indices observed for Preoccupied (E) category placement during the video-recorded clinical interview were: passive/vague discourse (implicit sense of failure, repetitious small complaints, and inchoate representations of implicit negative experiences), identity tied to fearful experiences, self-blame, and uncertainty about the past. On the whole, this individual projected his own fears of inadequacy onto others (unable to tolerate rejection due to poor self-esteem and preconceived ideas about others). Defenses observed in the clinical interview were passivity, compliance with the therapist, dependency, vagueness, projection, somatization, and withdrawal. Anxiety manifestations were noted in the striated muscles, smooth muscles (sympathetic nervous system), and in various reported physical illnesses. The DSM-IV diagnoses included panic disorder with agoraphobia, depressive disorder NOS, and dependent personality traits. Position on Davanloo’s Spectrum of Psychoneurotic Disorders: 4.
The main classification was assigned to E and the subclassification to E1 because the defining characteristic of this individual was that his identity was closely tied to early experiences with others (dependency with mother transferred to wife and dependent traits observed in relationship to the therapist). On the whole the individual appeared to be passive, compliant, and preoccupied with the past and with others’ perceptions of him (main features of E1 subclassification).
Assessed Character Assignment Dr. Hesse observed in his analysis that this individual was identified by characteristics typical of the E1 classification. He also observed that the individual exhibited a kind of “chronic mourning” about having grown up in childhood with a mother who had a serious illness. For this reason, Dr. Hesse assigned an additional secondary classification of Cannot Classify (CC) since the inchoate representations of implied negative experiences exhibited by this person may have been different than what is typical of most speakers falling in this category (which is why the “flavor” of the discourse violations appeared to differ from a classic E1 text). These instances of chronic mourning appeared in the loss section of the AAI, but did not fit into the unresolved/disorganized (U/d) scoring system. The final classification that was assigned by Dr. Hesse: E1/CC.
Case Number Three
The patient is a 51-year-old female who works as an executive assistant and who has suffered panic attacks during the preceding six months. The panic attacks were precipitated by an intimate relationship with a co-worker who, she reported, was immature and acted out sexually with pornography and strippers. She felt she could not be safe in the relationship with this partner, but was unable to leave it.
The patient is one of two siblings—a female fraternal twin. History is significant for early childhood abandonment trauma. When the patient was six years old her parents divorced because her mother had been unfaithful in the marriage. Upon discovering the affair, the patient’s father divided the siblings; he kept the sister with him and gave custody of the patient to her mother. The patient and her mother were homeless for two years after the divorce.
Predicted Category Placement Indices for placement in the preoccupied (E) category observed during the clinical interview were: linguistic confusion/slips; unbalanced blame towards self/others (including excessive guilt); identity tied to others (perceived things as a rejection); involving/preoccupying anger, and strikingly uncertainty and indecisiveness. Defenses included projection, projective identification (therapist as perpetrator), and acting out. This individual exhibited a regressed ego with a highly punitive superego with self and other. Anxiety manifestations included striated muscle tension and sympathetic nervous system activation (including frequent panic attacks). The patient had been diagnosed with panic disorder without agoraphobia, and she exhibited borderline personality traits. The position on Davanloo’s Spectrum of Psychoneurotic Disorders: 4.
A defining characteristic of the interview included preoccupied fear associated with early childhood trauma The patient would have been assigned an E3a classification on the AAI were it not for the patient’s responsiveness to therapist’s interventions over the course of the interview; F4b was the best-fitting alternative classification that allowed for both E3a traits and the earned secure attachment signified by the patient’s responsiveness. The E3 transcripts differ from E1 (passive) and E2 (preoccupied anger) in that the central theme relates to fearful preoccupation about traumatic events. The E3-type individual typically is seen to be confused, fearful, and overwhelmed—it is interesting to note that this category has been found to be associated with borderline diagnoses (
Hesse, 1999). In this example, an E3a category placement, the preoccupying fear was conceptualized in terms of frantic unconscious efforts to avoid internalized feelings of abandonment. The F4b is the best fitting alternative classification, signifying a move toward earned secure attachment (during the clinical interview this individual was responsive to therapeutic interventions designed to undo unconscious projections).
Assessed Character Assignment The AAI classification for this patient notes considerable trauma and chaos (witness to marital violence, sporadic outbursts of rage, victim of sexual abuse, and attempted rape). The secure (F) category placement for the main classification was assigned because the patient did not lapse in any notable way during the AAI interview when discussing her traumatic experiences. Dr. Hesse qualified this rationale for classification with his determination that “at some higher level, rejection and neglect must have occurred.” Thus one explanation for the difference between AAI prediction and AAI classification for this case (i.e., the fact that AAI prediction was based on preoccupation regarding childhood abandonment specifically and AAI classification was based on an ultimately rational overview with respect to other traumatic experiences) can be accounted for by superior biographical data on the part of the author (RJN). Final AAI classification F5/F4a/(other) acknowledges moderate preoccupation with relationships to attachment figures with acceptance of continuing involvement.
Case Number Four
The patient is a 51-year-old male executive who came to therapy because he was in an unhappy love relationship and felt conflicted about leaving his partner. His underlying trauma was deep guilt over an episode of violent acting out (shooting a gun) at his brother in his teenage years. The patient suffered from unresolved sibling rivalry between himself and his brother for his father’s affection. Indices of Secure (F) attachment classification were: linguistic coherence, metacognitive monitoring, coherence of mind, flexibility/adaptability during the interview process, and valuing of attachment.
Defenses included intellectualization, repression, and projective identification (identifying the therapist as the dismissive father figure). Anxiety manifestations occurred in the striated muscles and sympathetic nervous system. DSM-IV diagnoses: Dysthymia, Bereavement, and Partner Relational Problem. Position on Davanloo’s Spectrum of Psychoneurotic Disorders: 3.
Predicted Category Placement The F1 subclassification rationale: patient articulated some harsh childhood experiences that included moderate rejection of attachment; however, his state of mind (guilt over the episode with the gun, which created a need for punitive and avoidant/dismissive self-structures) did not prevent him from utilizing the therapy successfully (therapist was able to undo the projection and the patient made a breakthrough to unconscious feeling/impulse during the clinical interview).
Assessed Character Assignment Analysis of the AAI transcript indicated this case to be a fairly straightforward secure (F) transcript in general due to the following reasons: (a) no active indices of preoccupied anger; (b) relevance violations were not passive/vague; (c) no idealization of either parent; (d) no notable claims to lack of memory; (e) no derogation of attachment figures; and (f) no globally anomalous violations of coherence that could lead to a CC classification. The F1 subclassification was determined based on speaker’s articulation of a harsh childhood while maintaining a “cold” (setting aside) and “lead with your chin” stance about attachment-related experiences and an ongoing collaborative stance during the interview. F1 transcripts in general most closely resemble Dismissive (Ds) insecure attachment, which is why it was important in this case to rule out Ds category descriptors. Final classification determined by Dr. Hesse’s analysis of the AAI: F1
Case Number Five
The patient is a 48-year-old geologist (on disability at the time of testing) who is seeking therapy as an alternative to electric cortical shock therapy for severe bipolar depressive episodes. She has suffered from bipolar disorder since her early 20s and has had manic as well as depressive episodes. She also has had systemic lupus erythematosus for 10 years, which complicates her bipolar disorder. She is an only child whose mother was quite histrionic and narcissistic. The patient suffered from significant guilt because of her anger at her mother’s unavailability. She also developed a highly sexualized attachment to her father, for which she also felt guilt.
Predicted Category Placement Indices of Secure (F) attachment were: adaptive response to the therapist’s interventions in the clinical interview (derepression of the unconscious, de-activation of the punitive superego structure, and re-orienting of the observing ego), yielding high scores for autonomy, flexibility, and collaboration with the interview process.
Pathological defense structures included: instant repression (ignoring and minimization), projection, and somatization. Manifestations of anxiety included: striated muscle, smooth muscle (sympathetic nervous system activation), and cognitive-perceptual disruption (dissociation). DSM-IV diagnoses included: Bipolar I Disorder, Most Recent Episode Mixed; and Histrionic Personality Disorder. Position on Davanloo’s Spectrum of Psychoneurotic Disorders: 4. The F4b subclassification was determined on the basis that this individual exhibited ongoing pre-occupation about childhood experiences with parents (controlling father and role-reversing with mother), however the patient ultimately collaborated and responded adaptively to therapist’s interventions. Final AAI prediction: F/F4b
Assessed Character Assignment AAI transcript analysis likewise yielded F/F4b category placement for the following reasons: (a) some preoccupation with attachment-related experiences evidenced by excessively long turns of speech, occasional violations of relevance (i.e., discussing the father when the topic is the mother), and passive/vague discourse; (b) speaker reported experiencing a generally difficult childhood and adulthood with mental health problems in addition to medical condition (systemic lupus and chronic pain); (c) speaker reported experiences with parents on the whole described as unloving; (d) at times the speaker gave the impression of being vague and detached; and (e) the greater part of the interview was determined to be “ultimately rational and convincingly conscious.” Final AAI classification: F/F4b
Case Number Eight
The patient is a 40-year-old female yoga instructor who was in a conflicted marital relationship and experienced anxiety, depression, sexual acting out, and financial irresponsibility. The patient had suffered severe early childhood trauma: her mother succumbed to a deteriorating schizophrenic illness and had to be involuntarily hospitalized when the patient was six years old. The patient is the youngest of five siblings and closely attached to her older sister. Both the sisters were placed in an orphanage upon the mother’s hospitalization. At the orphanage, they were separated in different wards. The father raised the remaining older three male siblings. When the patient reached adolescence she was placed in foster care.
This patient was assigned the Cannot Classify (CC) because there were emergent secure (F) properties in the interview that reflected a shifting state of mind with respect to attachment experiences. In this case preoccupied (E) seemed like the closest, best-fitting alternative to CC classification due to the following characteristics of the interview: role-reversal (accommodations to the psychic needs of the other together with inattention toward the self); inchoate representations of negative experiences (resisting mental coherence at the level of the stimulus, using tactical defenses to keep new information or the therapist at bay, and splitting and dissociation defenses); fearful preoccupation about past traumatic events (E3), which was evidenced by an inability to shift attention away from traumatic events (for example, she would shift attention away from a discussion of feelings in favor of the relational strategy of “going dead” in response to situations or people perceived as threatening); poor boundaries between self and other; and an inability to tolerate separations from others. Secure (F) indices included responsiveness to therapeutic interventions and some metacognitive monitoring.
Pathological defense structures included: ignoring, neglecting, splitting (to overcome anxiety, the other is “made into” a very bad person), denial and dissociation (avoidance of underlying anger). Anxiety manifestations included: striated muscle tension and cognitive-perceptual anxiety discharge. The DSM-IV diagnoses included: anxiety disorder NOS, dysthymic disorder, and borderline personality disorder. Position on Davanloo’s Spectrum of Psychoneurotic Disorders: 6.
Predicted Category Placement The authors assigned this individual an E3 subclassification due to the central characteristic of the interview—a whole being preoccupied fear, overwhelmed, and confused, rather than angry (E2) or vague (E1). It is an interesting to note again that the E3 subcategory has been found to be associated with borderline diagnoses (
Hesse, 1999). The F4b as an alternative subclassification was assigned because of ongoing confusion and fearful preoccupation with traumatic experiences and some valuing of attachment (responsiveness to therapeutic interventions and metacognition).
Assessed Character Assignment The AAI transcript analysis yielded CC/E3/F4b classification because “the speaker’s mind remains traumatized by fear, but the effects have been altered (for the better) by therapy. . .in the end what the reader comes away with is an impression of a speaker who, while having come a long way, is still overwhelmed by frightening experiences related to attachment” (included in erik hesse’s notes along with final aai classifications). In summary, the text as a whole resembled an E3 classification with evidence of progress made toward earned secure attachment (forgiveness of parents, humor, recognition of the effects of experiences on the shaping of the self, and valuing of attachment). The AAI analysis also identified some characteristics common to Ds3 profiles in that the speaker attempted at times to down play the extreme nature of parenting experiences. This characteristic, however, was not pronounced enough to assign Ds3 to the final classification.
Case Number Nine
Patient is a 50-year-old female psychotherapist. She suffered from anxiety and depression along with extremely low self-esteem. She was in an abusive marriage and felt helpless to leave the relationship because of guilt about separating her son from his father. Secondary to her inability to leave the marriage was her perceive stigma of being a divorcee. The patient is the younger sister of two siblings. She grew up in a trailer park in a working-class environment with parents who were socially neglectful. Her mother was obese and poorly educated and her father was the “black sheep” of the family. The patient felt excessive shame as a child about her parents’ neglectful behaviour and low social stature. She expressed guilt about having these feelings towards them. She was also traumatized as the victim of a violent assault, having been stabbed randomly by an out-of-control psychiatric patient.
Predicted Category Placement This individual was seen to fit the CC classification during the video-recorded clinical interview because indices characteristic of two preoccupied profiles (E1 and E2) were present enough to make it difficult to assign one single classification. Indices common to E profiles included: excessive blame toward self, involving/preoccupying anger, identity tied to parents and early trauma, inchoate representations of negative experiences, implicit sense of personal failure, ambivalence between involving/preoccupying anger (E2) on the one hand and passivity (E1) on the other, and evaluatory oscillations (compliance on the one hand and defiance on the other—recognizing abusive domestic relationship at times and at other times defending the relationship). Indices of secure (F) classification included some metacognitive monitoring (responsiveness to therapeutic interventions), including rueful recognition of the power of the past in shaping self.
Defenses exhibited in the clinical interview included: denial, projection, obsessions, compliance/defiance, primitive identification with the victim parent (her mother), helplessness, and relentless self-attack. Manifestations of anxiety included striated muscle tension, and cognitive-perceptual discharge (some lapses in consciousness that would interrupt the progression of the narrative (evidenced by repeated ambivalence and turning back to masochistic position with respect to sadistic domestic partner). The DSM-IV diagnoses included: depressive disorder NOS and dependent personality disorder with masochistic features. Position on Davanloo’s Spectrum of Psychoneurotic Disorders: 6.
The E1 and E2 subclassification was determined for this case since one of the defining features of the clinical interview was the patient’s ambivalence between involving/preoccupying anger on the one hand (E2) and passive/helpless dialogue on the other. The F4b alternative subclassification was determined because there were emergent F properties within the interview as evidenced by the patient’s ability to sometimes monitor her own thoughts and respond adaptively to therapeutic interventions.
Assessed Character Assignment The AAI analysis indicated that this individual has the following characteristics of preoccupied (E) profiles: passivity of thought process, identity closely tied to parents, uncertain/indecisive/unobjective speaking, extensive jargon use, and psychological expressions (inappropriately clinical references, which were seen to be unrelated to an authentically reflective state of mind). Indices of a secure (F) transcript were: flexibility, valuing of attachment at times, forgiveness and compassion towards mother, and a lively personal identity. In terms of subclassification for this case, Dr. Hesse indicated that on the whole the transcription contained aspects of E1, E2, and F4b that were mixed together making the text Cannot Classify. It is interesting to note in this case that there was a positive outcome to the therapy in that the woman eventually divorced her abusive husband and married a man with whom she developed a loving and successful relationship. This result of therapy can be seen to be reflective of emergent F properties (signifying adaptive potential).
Case Number Eleven
The patient is a 61-year-old male who works part-time as a psychotherapist, part-time as a construction worker and who has a history of lifelong anxiety with secondary depression. He is a former heroin user who was addicted for more than 20 years (a large part of that time was spent homeless). The patient has an older brother. During childhood, and over the course of his life, he had been perceived as sensitive and artistic. This resulted in a great deal of conflict with his mother, who he reports as being cold, authoritarian, harsh, judgmental, and controlling. He reports experiencing symptoms of psycho trauma when he was removed from his first school (where he was happy, well adjusted), and placed in a regimented private school (where he did not fit in). At the time the patient presented for therapy, he was in a romantic relationship with a partner who he described as rigid and controlling. He was suffering panic about his aggressive feelings in that relationship.
Predicted Category Placement Indices of U/d disorganized classification during the video-recorded clinical interview included: lapses in the monitoring of reasoning, disoriented speech, prolonged silences, and dissociation. Cannot Classify (CC) was assigned as a secondary placement because both Dismissing (Ds) and Preoccupied (E) features were present during the clinical interview. Neither was considered to be predominant. Indices of D category placement included: ongoing detachment and dismissal as a defense against emotional closeness, insistence on lack of memory, little articulation of hurt or distress, minimization of negative experiences, and abstract/remote from memories and feelings. Indices of E main classification were: identity tied to parents, and involving/preoccupying anger.
Pathological defenses employed by the patient included: minimization, projection, detachment, humor, sarcasm, identification with the aggressor (in this case the aggressor was his mother who would shut him down if he exhibited even a minimal amount of defiance toward her rigidly set rules), dissociation and slouching. Anxiety manifestations included: striated muscle tension, parasympathetic discharge (numbness/shut down and dizziness), and cognitive-perceptual discharge (incoherent process and dissociation). The DSM-IV diagnoses included: panic disorder without agoraphobia, dysthymic disorder, and personality disorder with dependent traits. Position on Davanloo’s Spectrum of Psychoneurotic Disorders: 7.
The Ds1 subclassification was concluded based on the patient’s dismissal of most attachment-related considerations from thinking. The Ds4 subclassification was considered for this individual because the patient exhibited marked fear regarding the loss of his child through death; however, Ds4 subclassification was ruled-out due to the fact that in this case the fear could be traced to its source (the patient’s son was being stalked by gang members). In order to assign The Ds4 subclassification, the fear surrounding the loss of the child through death must be connected to an unknown source. The E2 subclassification was assigned based on this patient’s frequent underlying expressions of anger towards his mother during the clinical interview.
Assessed Character Assignment AAI analysis for this case yielded a main-classification assignment of U/d due to extreme behavioral responses related to traumatic losses of two girlfriends. The CC was added as an alternative main category placement due to there being passages in the transcript that were representative of both dismissing (Ds) and preoccupied (E) placement. Dr. Hesse assigned the subclassification Ds4 because in his assessment “there is fear of loss of imagined child which is not traced to its source.” In this case, as noted above, the authors were able to trace the fear of loss of death of the child to its source, leading to a Ds1 assignment. The AAI analysis indicated that the transcript on the whole was “E-like” with some notable instances of involving/preoccupying anger (E2). Final classification: U/CC/Ds4/E-general.