Research has focused on identifying empirically supported treatments (ESTs) for particular disorders, and has paid less attention to the cultural competency of those interventions (
Bernal & Sharrón-del-Río, 2001). However, as these treatments move from the university setting to the outside community, the importance of cultural competency is being re-emphasized. The effectiveness of ESTs appears less robust in community settings in which heterogeneous and minority populations are being treated (
Weersing & Weisz, 2002;
Weisz et al., 2013). Studies show that mental health services, especially empirically supported psychotherapies, have not been available and/or effectively delivered to minority populations (
Bernal & Sharrón-del-Río, 2001;
Hall, 2001;
Sue & Zane, 2006;
Markowitz, Spielman, Sullivan, & Fishman, 2000). The growth of minority populations—particularly the Latino population, which (along with the Asian population) grew the fastest in the last decade (
U.S. Census Bureau, 2010)—will continue to limit the relevance of efficacy trials for treatments unless their effectiveness with these populations can be demonstrated.
It is possible that interventions that have not been adapted for specific cultures may contain features that make them well-suited to these cultural groups. For example,
Rosselló and Bernal (1999) reported that the focus on current interpersonal conflicts make Interpersonal Psychotherapy (IPT) a culturally acceptable treatment to Latinos because of its relevance to Latino values of
familismo and
personalismo. Familismo refers to Latino culture’s emphasis on the importance of the family’s well-being over one’s individual needs and of connectedness to one’s family.
Personalismo refers to the desiring and valuing of personal relationships with others (
Añez, Paris, Bedregal, Davidson, & Grilo, 2005). With IPT’s emphasis on restoring harmony to one’s relationships, both familial and peer, IPT may help Latino patients feel that their values are respected and incorporated into the goals of treatment without requiring additional cultural adaptations. The culturally competent clinician would modify the style of communication to be more syntonic with cultural norms for conducting relationships and explore new ways of communicating that might be helpful in achieving improved relationships (
Markowitz et al., 2009).
Determining Cultural Competency: Therapist-Related Factors
Cultural competence is embedded in multiple aspects of an intervention, including the clinician’s ability to deliver the treatment in the patient’s preferred language, the clinician’s interpersonal style in delivering the intervention, and the clinician’s ability to provide a cultural context for the intervention (
Andrés-Hyman, Ortiz, Añez, Paris, & Davidson, 2006). One way that this concept has been examined is through ethnic matching of client and therapist.
Therapists who share their patients’ ethnic backgrounds are more likely to have similar cultural backgrounds, which helps to facilitate the provision of culturally responsive treatment (
Sue, Fujino, Hu, Takeuchi, & Zane, 1991;
Tharp, 1991). Ethnic matching appears to reduce the likelihood of miscommunication between patient and therapist stemming from cultural differences (
Sue, 1998), which may increase patient self-disclosure and empathy (
Fiorentine & Hillhouse, 1999) and reduce clinician ethnic biases (
Halliday-Boykins, Schoenwald, & Letourneau, 2005).
Fuertes and colleagues (2006) found that minority ethnic patients who rated their therapists more multi-culturally competent also rated them highly on measures of therapeutic alliance and empathy. Therefore, cultural competency is intertwined with general perceptions of the therapist-patient relationship. Additionally, studies have consistently shown that ethnic minority clients prefer an ethnically similar counselor over an ethnically dissimilar counselor (
Proctor & Rosen, 1981;
Terrell & Terrell, 1984;
Watkins & Terrell, 1988;
Watkins, Terrell, Miller, & Terrell, 1989).
Studies examining the effects of ethnic matching on treatment outcome are relatively rare (
Hall, 2001) and have primarily been conducted with adults receiving usual care in community settings (
Erdur, Rude, & Baron, 2003;
Fiorentine & Hillhouse, 1999;
Sue et al., 1991). Only a few studies have focused on these effects with children and adolescents (
Hall, Guterman, Lee, & Little, 2002;
Jerrell, 1998;
Yeh et al., 1994). The available findings on treatment outcomes associated with ethnic matching are mixed (
Gamst, Dana, Der-Karabetian, & Kramer, 2000,
2004;
Sue, 1991;
Yeh et al., 1994). However, results generally support the use of ethnic matching with Latino adolescents and adults in community settings (
Gamst et al., 2000;
Hall et al., 2002;
Russell, Fujino, Sue, Cheung, & Snowden, 1996;
Sue et al., 1991;
Yeh et al., 1994). Specifically, adolescent and adult studies have found that ethnically matched Latino clients tend to drop out less frequently from treatment and attend more sessions (
Hall et al., 2002;
O’Sullivan & Lasso, 1992;
Yeh et al., 1994). The impact of ethnic matching on the implementation of empirically supported psychotherapies, such as Interpersonal Psychotherapy with Latino adolescents, has not been examined to date.
Determining Cultural Competency: Patient-Related Factors
Although intervention-related factors are paramount in determining its cultural competency, the importance of these factors for treatment outcome may vary by the patient’s level of acculturation and assimilation. Acculturation refers to the sociocultural change process that individuals experience when encountering and adapting to a new culture (
Berry, Phinney, Sam, & Vedder, 2006;
Williams & Berry, 1991;
Lopez-Class, Castro, & Ramirez, 2011). This may entail assuming the values, language, and cultural practices of the host society or undergoing changes in language, socioeconomic status and/or cultural orientation such as alterations in values and attitudes (
Olmedo, 1979). Researchers have identified two components of the acculturation process: 1) culture of origin involvement (enculturation) and 2) host cultural involvement (assimilation), and recognize their effects on mental health in immigrants (
Gonzales, Knight, Morgan-Lopez, Saenz, & Sirolli, 2002).
Some of the changes inherent in the acculturation process can be stressful, including family separations and reunifications, trauma before and during the journey, change in socioeconomic status, and changes in family rules and roles (
Portes & Rumbaut, 2001). Adolescents may be particularly susceptible to the effects of stressors during the acculturation process. Acculturative stress during adolescence may lead to increased conflict with parents, which may intensify typical adolescent struggles with developmental changes, identity conflicts, individuation, and autonomy. Adolescents tend to adopt the language, values, and behaviors of the dominant culture more easily than their parents, which may result in a clash with the parents’ traditional values and behaviors (
Portes & Rumbaut, 2001). As a result, adolescents may become more immersed within mainstream culture of the United States (U.S.; more assimilated) than their more enculturated parents (
Fulgini, 1998), creating a gap and concomitant tension between the acculturation levels of adolescents and their parents (
Pasch et al., 2006).
Although adolescents may assimilate more quickly than their parents, research has shown that, for Latino adolescents, both high and low levels of acculturation may be risk factors for various problems, including depression (
Gonzales, Knight, Birman, & Sirolli, 2004;
Hovey & King, 1996), substance abuse (
Brook et al., 1998), poor school functioning (
Chapman & Perreira, 2005;
Vega, Khoury, Zimmerman, Gil, & Warheit, 1995), and delinquent behavior (
Fridrich & Flannery, 1995;
Gonzales et al., 2002).
Gonzales and colleagues (2002) reviewed 10 studies assessing acculturation and adolescent aggression, finding that 6 of the 8 adolescent studies reported that higher assimilation was associated with greater delinquency and stronger relationships with antisocial peers. In contrast,
Glover, Pumariega, Holzer, Wise and Rodriguez (1999) found that foreign birth and low English language fluency were significant risk factors for adolescent anxiety in the Latino population. Thus, the effectiveness of a treatment for a Latino patient may depend on how well it addresses acculturation level and associated difficulties.
The emergence of acculturation research has brought about diverse and changing views of the acculturation process, which influence how acculturation is measured. Early on, acculturation typically was measured by single items, such as place of birth or language predominantly spoken in the home and other proxy measures, for example, generational status and age at migration (
Lopez-Class et al., 2011). More recently, however, the definition of the acculturation process has expanded to include concepts such as changes in attitudes and values, and recognition that the process is influenced by the context in which it occurs. For these reasons, other measures of acculturation were developed to capture changes occurring on multiple dimensions, including beliefs, values, attitudes, and behaviors (
Thomson & Hoffman-Goetz, 2009). Extant measures examine the presence of racial or ethnic discrimination and the effects of the acculturation process on personal contexts, such as family and socioeconomic status (
Lopez-Class et al. 2011,
Abraido-Lanza, Armbrister, Florez & Aguirre, 2006). Several well-researched and validated measures include the Acculturation Scale for Mexican Americans II (
Cuellar, Arnold, & Gonzalez, 1995), the Bidimensional Acculturation Scale for Hispanics (
BAS; Marin & Gamba, 1996), and the Hispanic Stress Inventory (
Cervantes, Padilla, & Salgado de Snyder, 1991); however, since this was not initially part of the study design, we will be examining acculturation using proxy measures to obtain a preliminary look at how acculturation may affect Latino adolescents’ mental health and treatment outcomes.
The evidence for the role of acculturative stress in the development of negative outcomes in Latino youth makes it important to examine whether specific interventions may be more effective than others in treating depressed Latino youth who are at varying acculturation levels. Interpersonal Psychotherapy is a time-limited, empirically supported psychotherapy that may be particularly relevant for Latino youth given that the constructs and techniques can encompass and directly address the strains associated with changing family attachments, development of a new social support system, and intergenerational conflict arising from the acculturation process. Interpersonal Psychotherapy is based on the premises that depression occurs in an interpersonal context, depressed mood can affect relationships, and problems in relationships can affect mood. The targeted problem areas of IPT (grief, role transitions, interpersonal role disputes and interpersonal deficits) have demonstrated universality and relevance in diverse cultures (
Bolton et al., 2003,
2007;
Patel et al., 2010;
Markowitz et al, 2009). The adolescent adaptation, IPT-A, has demonstrated effectiveness for depressed adolescents, largely Latino and from underserved communities (
Mufson, Weissman, Moreau, & Garfinkel, 1999;
Mufson et al., 2004). It remains important to examine whether IPT-A, in its original form, meets the standard of cultural responsiveness and competency for a Latino adolescent population without specific cultural modifications beyond discussions of how to be sensitive to culturally accepted styles of communication between parents and their children.
Although research exists on the effects of level of acculturation and therapist-client ethnic matching, few studies have examined the effects of both these cultural competency factors as predictors and/or moderators of treatment outcomes for an empirically supported psychotherapy such as IPT. Moderators of treatment are patient characteristics present prior to treatment, independent of the type of treatment the patient receives. These have an interactive effect on treatment outcome with the type of treatment received (
Kraemer, Wilson, Fairburn, & Agras, 2002). These patient characteristics can also be predictors—characteristics related to treatment outcome, regardless of the type of treatment received (
Kraemer et al., 2002).
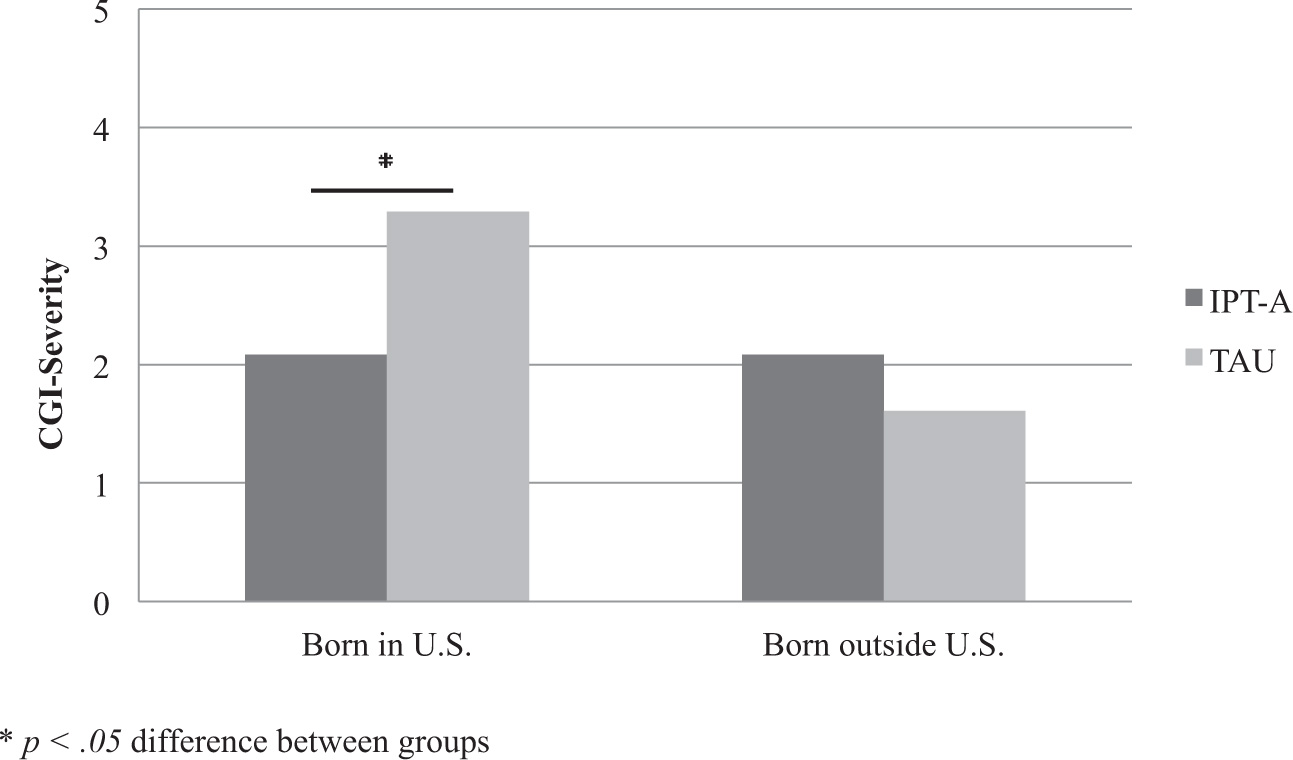
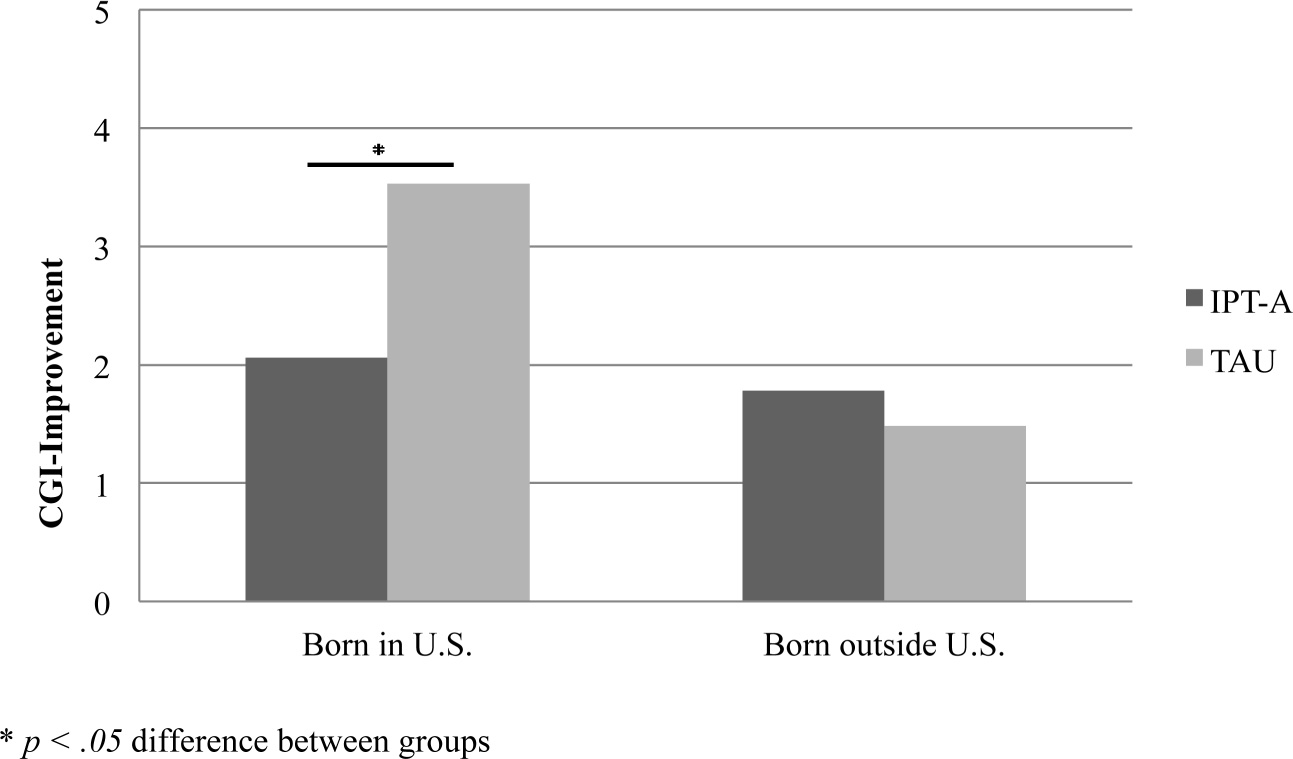
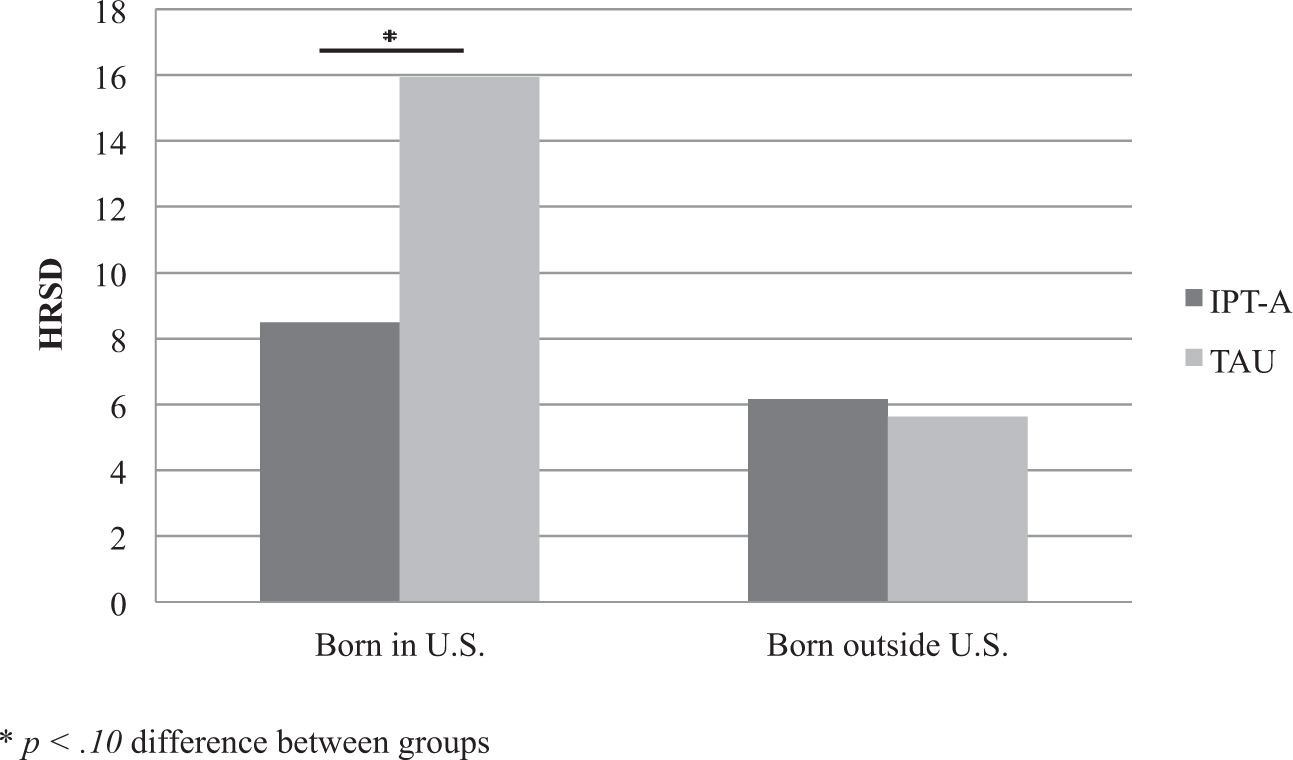
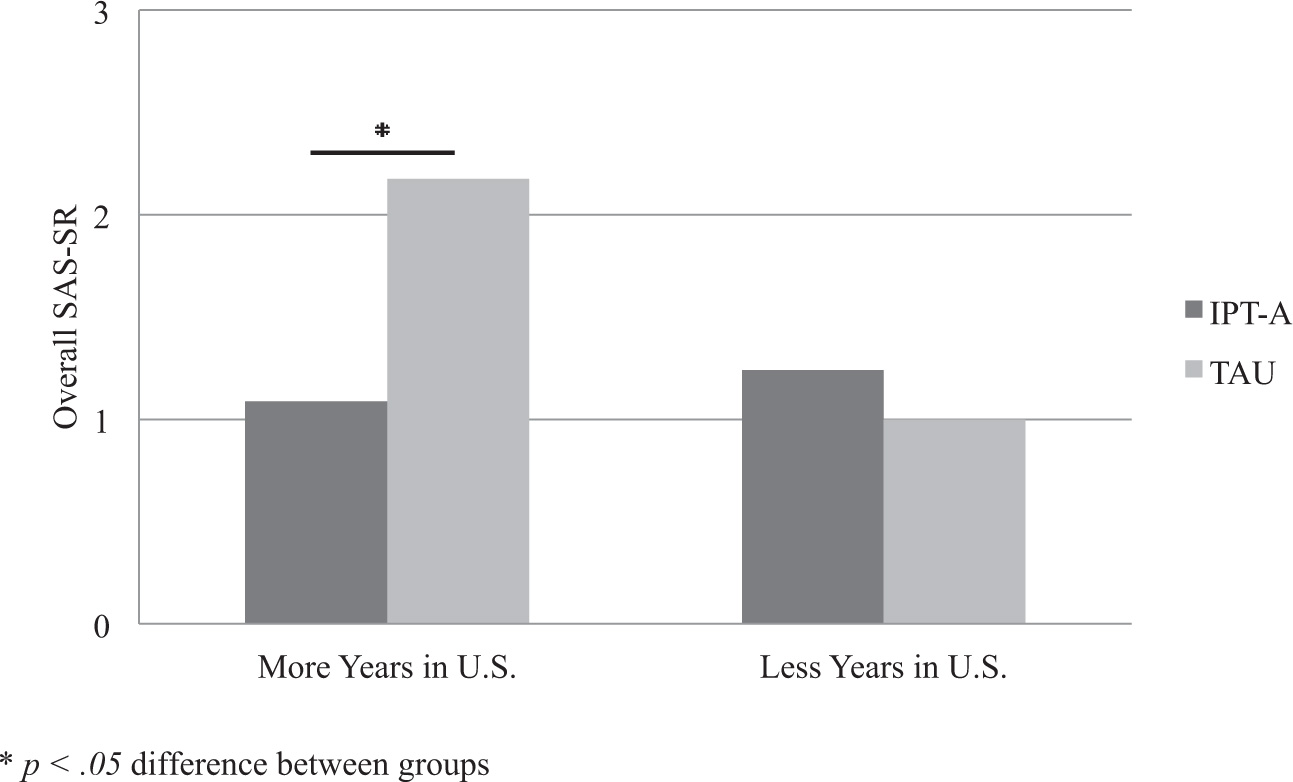
The current study examined two aspects of cultural competency: 1) the impact of level of acculturation, as determined by the proxy measures of place of birth (foreign or the U.S.) and length of residency in the U.S., and 2) the impact of ethnic matching between therapist and patient as predictors and/or moderators of treatment outcome in a randomized controlled trial of IPT-A compared to treatment as usual (TAU) for Latino adolescents suffering from depression. The impact of place of birth and length of residency on pretreatment levels of depressive symptoms and functioning was also examined. As these acculturation analyses were restricted to a Latino subset of the full sample used in
Mufson et al. (2004), this paper attempts to replicate the findings from the original clinical trial sample in the Latino-only sample. These analyses must be considered exploratory in nature as they are post hoc and limited by the use of proxy measures of acculturation. Although this study was exploratory, our a priori hypotheses were: 1) Adolescents who received IPT-A will have better treatment outcomes as measured by the primary outcome measures of depression (Hamilton Rating Scale for Depression, HRSD) and overall functioning (Children’s Global Assessment Scale, CGAS) despite level of acculturation, and 2) those adolescents who received IPT-A and were matched ethnically with their therapists would report better treatment outcomes on the primary measures.