Quick Reference for Schizophrenia
| Feature | Good Outcome | Poor Outcome |
|---|---|---|
| Age | Older | Younger |
| Gender | Female | Male |
| Social class | High | Low |
| Marital history | Married | Never married |
| Family history of schizophrenia | Negative | Positive |
| Perinatal complications | Absent | Present |
| Transcultural factors | Developing nations | Industrialized nations |
| Premorbid functioning | Good | Poor |
| Onset | Acute | Insidious |
| Duration | Short | Chronic |
| Sensorium | Clouded | Clear |
| Symptoms/subtypes | Paranoid subtype | Deficit syndrome |
| Affective symptoms | Present | Absent |
| Neurological functioning | Normal | Soft signs present |
| Neurocognition | Normal | Abnormal |
| Structural brain abnormalities | None | Present |
Reprinted with permission from Ho B, Black DW, Andreasen NC: Schizophrenia and other psychotic disorders, in The American Psychiatric Publishing Textbook of Clinical Psychiatry, 4th ed. Edited by Hales RE, Yudofsky SC. Arlington, Va, American Psychiatric Publishing, Inc, 2003, p 400.
| When the illness is new, to rule out alternative diagnoses and to stabilize the dose of antipsychotic medication |
| For special medical procedures such as electroconvulsive therapy |
| When aggressive or assaultive behavior presents a danger to the patient or others |
| When the patient becomes suicidal |
| When the patient is unable to properly care for himself or herself (e.g., refuses to eat or take fluids) |
| When medication side effects become disabling or potentially life threatening (e.g., severe pseudoparkinsonism, severe tardive dyskinesia, neuroleptic malignant syndrome) |
Reprinted with permission from Ho B, Black DW, Andreasen NC: Schizophrenia and other psychotic disorders, in The American Psychiatric Publishing Textbook of Clinical Psychiatry, 4th ed. Edited by Hales RE, Yudofsky SC. Arlington, Va, American Psychiatric Publishing, Inc, 2003, p 418.
| Efficacy |
| Schizophrenia (FDA approved for all) |
| Treatment-resistant schizophrenia (clozapine) |
| Mania (FDA approved for olanzapine) |
| Depression/anxiety/agitation (efficacy established but not FDA approved for these purposes) |
| Side effects |
| Weight gain |
| Sedation |
| Akathisia |
| Orthostatic hypotension |
| Dizziness |
| ↑ Triglycerides |
| EPS, NMS (rare) |
| Agranulocytosis (clozapine) (rare) |
| Seizures (clozapine) |
| Safety in overdose |
| Seizures with clozapine in overdose. Respiratory depression in combination with other CNS depressants. QT interval changes. Lavage and vital sign support |
| Dosage and administration |
| Clozapine: 12.5–25 mg; then increase dosage 25–50 mg per week, as needed and tolerated, to 300–600 mg/day |
| Risperidone: 0.5–1 mg b.i.d. to 3 mg b.i.d. by end of first week, as tolerated |
| Olanzapine: 2.5–5 mg h.s.; increase by 5 mg every week to 20 mg h.s. |
| Quetiapine: 25 mg b.i.d.; increase total daily dose by 50 mg, as needed and tolerated, to 300–600 mg/day |
| Ziprasidone: 20 mg/day or b.i.d.; increase by 20–40 mg per week, to a maximum dosage of 80 mg b.i.d. |
| Aripiprazole: 15 mg/day; increase up to 30 mg/day after 1 week |
| Full benefits in 4 weeks to 6 months |
| Discontinuation |
| Mild cholinergic rebound, faster relapse |
| Taper as slowly as titrated up |
| Drug interactions |
| Fluvoxamine (1A2 inhibitors): ↑ atypical antipsychotic levels |
| EtOH: ↑ sedation and orthostasis |
| Antihypertensives: may ↑ orthostasis |
| Carbamazepine: ↓ serum levels of olanzapine; contraindicated with clozapine |
| CNS depressants: ↑ sedation |
CNS = central nervous system; EPS = extrapyramidal symptoms; EtOH = ethanol; FDA = U.S. Food and Drug Administration; NMS = neuroleptic malignant syndrome
Reprinted with permission from Schatzberg AF, Cole J, DeBattista C: Antipsychotic drugs, in Manual of Clinical Psychopharmacology, 4th ed. Arlington, Va, American Psychiatric Publishing, Inc, 2003, pp 188–189.
| Drug | Major Metabolism Site(s) | Enzyme(s) Inhibited |
|---|---|---|
| Aripiprazole | 2D6, 3A4 | None known |
| Clozapine | 1A2, 3A4, 2D6, 2C19, UGT1A4, UGT1A3 | 2D6a |
| Olanzapine | 1A2, 2D6, UGT1A4, ?other UGTs, ?FMO3 | None known |
| Quetiapine | 3A4, sulfation | None known |
| Risperidone | 2D6, 3A4 | 2D6b |
| Ziprasidone | Aldehyde oxidase, 3A4, 1A2 | None known |
Note: Data presented relate to parent drug and metabolites combined. FMO3 = flavin monooxygenase; UGT = uridine 5’-diphosphate glucuronosyltransferase
a Mild
b Moderate
Modified and reprinted with permission from Cozza KL, Armstrong SC, Oesterheld JR: Psychiatry, in Concise Guide to Drug Interaction, 2nd ed. Arlington, Va, American Psychiatric Publishing, Inc, 2003, p 361.
| Women experience more mood symptoms |
| Men experience more deficit symptoms |
| Women present as more socially appropriate |
| Delusional themes differ between the two sexes |
| Men engage in more substance abuse |
| Women have more comorbid problems (allergies, endocrine disturbances, eating disorders, posttraumatic stress disorders, psychophysiological disorders) |
Reprinted with permission from Seeman MV: Gender differences in schizophrenia across the life span, in Schizophrenia Into Later Life: Treatment, Research, and Policy. Edited by Cohen CI. Arlington, Va, American Psychiatric Publishing, Inc, 2003, p 143.
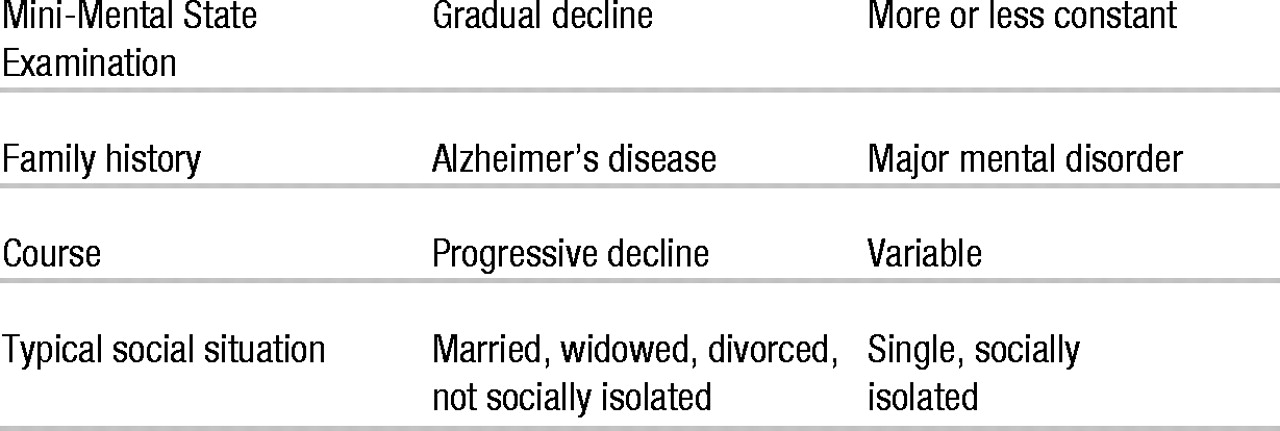
| Symptoms | Alzheimer’s Disease | Schizophrenia |
|---|---|---|
| Delusions | ||
| Someone stealing | +++ | ++ |
| Thought control | +/− | ++/+++ |
| Hallucinations | ||
| Auditory | +/++ | ++/+++ |
| Visual | ++/+++ | + |
| Cognitive impairment | ||
| Short-term memory loss | +++ | + |
| Word-finding difficulties | ++/+++ | −/+ |
| Disorientation | ++ | −/+ |
| Mini-Mental State Examination | Gradual decline | More or lesss constant |
| Family history | Alzheimer’s disease | Major mental disorder |
| Course | Progressive decline | Variable |
| Typical social situation | Married, widowed, divorced, not socially isolated | Single, socially isolated |
+/− = may or may not be present; + = may be present; ++ = often present; +++ = present in most
Reprinted with permission from Desai AK, Grossberg GT: Differential diagnosis of psychotic disorders in the elderly, in Schizophrenia Into Later Life: Treatment, Research, and Policy. Edited by Cohen CI. Arlington, Va, American Psychiatric Publishing, Inc, 2003, p 61.
| Extrapyramidal Side Effects/Tardive Dyskinesia | Prolactin Elevation | Weight Gain | Glucose Abnormalities | Lipid Abnormalities | QTc Prolongation | Sedation | Hypotension | Anticholinergic Side Effects | |
|---|---|---|---|---|---|---|---|---|---|
| Thioridazine | + | ++ | + | +? | +? | +++ | ++ | ++ | ++ |
| Perphenazine | ++ | ++ | + | +? | +? | 0 | + | + | 0 |
| Haloperidol | +++ | +++ | 0 | 0 | 0 | 0 | ++ | 0 | 0 |
| Clozapinea | 0b | 0 | +++ | +++ | +++ | 0 | +++ | +++ | +++ |
| Risperidone | + | +++ | ++ | ++ | ++ | + | + | + | 0 |
| Olanzapine | 0b | 0 | +++ | +++ | +++ | 0 | + | + | ++ |
| Quetiapinec | 0b | 0 | ++ | ++ | ++ | 0 | ++ | ++ | 0 |
| Ziprasidone | 0b | + | 0 | 0 | 0 | ++ | 0 | 0 | 0 |
| Aripriprazoled | 0b | 0 | 0 | 0 | 0 | 0 | + | 0 | 0 |
0 = no risk or rarely causes side effects at therapeutic dose; + = mild or occasionally causes side effects at therapeutic dose; ++ = sometimes causes side effects at therapeutic dose; +++ = frequently causes side effects at therapeutic dose
a Also causes agranulocytosis, seizures, and myocarditis
b Possible exception of akathisia
c Also carries warning about potential development of cataracts
d Also causes nausea and headache
Reprinted with permission from American Psychiatric Association: Practice Guideline for the Treatment of Patients With Schizophrenia, Second Edition. Arlington, Va, American Psychiatric Publishing, Inc, 2004, in press.
Information & Authors
Information
Published In


History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).