Personality types and personality disorders
Charting the history of efforts to understand personality types and differences among them would involve exploring centuries of scholarly archives, worldwide, on the varieties of human behavior. It is human behavior, in the end, that serves as the most valid measurable and observable benchmark of personality. In many important ways, we are what we do. The “what” of personality is easier to come by than the “why,” and each of us has a personality style that is unique, almost like a fingerprint. At a school reunion, recognition of classmates not seen for decades derives as much from familiar behavior as from physical appearance.
As to why we behave the way we do, we know now that a fair amount of the reason relates to our “hard wiring.” To varying degrees, heritable temperaments that vary widely from one individual to another determine the amazing range of behavior in the newborn nursery, from cranky to placid. Each individual’s temperament remains a key component of that person’s developing personality, added to by the shaping and molding influences of family, caretakers, and environmental experiences. This process is, we now know, bidirectional, so that the “inborn” behavior of the infant can elicit behavior in parents or caretakers that can in turn reinforce infant behavior: placid, happy babies may elicit warm and nurturing behaviors; irritable babies may elicit impatient and neglectful behaviors.
But even-tempered, easy-to-care-for babies can have bad luck and land in a nonsupportive or even abusive environment, which may set the stage for a personality disorder, and difficult-to-care-for babies can have good luck, protected from future personality pathology by especially talented and attentive caretakers. Once these highly individualized dynamics have had their main effects and an individual has reached late adolescence or young adulthood, his or her personality will usually have been pretty well established. We know that this is not an ironclad rule; there are “late bloomers,” and high-impact life events can derail or reroute any of us. How much we can change if we need to and want to is variable, but change is possible.
Twentieth-century concepts of personality psychopathology
Personality pathology has been recognized in most influential systems of classifying psychopathology. The well-known contributions by European pioneers of descriptive psychiatry such as Kraepelin (
1), Bleuler (
2), Kretschmer (
3), and Schneider (
4) had an important impact on early twentieth-century American psychiatry. For the most part, Kraepelin, Bleuler, and Kretschmer described personality types or temperaments, such as asthenic, autistic, schizoid, cyclothymic, or cycloid, which were thought to be precursors or less extreme forms of psychotic conditions such as schizophrenia or manic-depressive illness—systems that can clearly be seen as forerunners of the current axis I/axis II “spectrum” models. Schneider, by contrast, described a set of “psychopathic personalities” that he viewed as separate disorders co-occurring with other psychiatric disorders. Although these classical systems of descriptive psychopathology resonate strongly with the framework eventually adopted by the American Psychiatric Association (APA) and published in its
Diagnostic and Statistical Manual of Mental Disorders (DSM), they were widely overshadowed in American psychiatry during the mid-twentieth century by theory-based psychoanalytic concepts stimulated by the work of Sigmund Freud and his followers.
Freud’s emphasis on the presence of a dynamic unconscious—a realm that, by definition, is mostly unavailable to conscious thought but a powerful motivator of human behavior (key ingredients of his topographical model)—was augmented by his well-known tripartite structural theory, a conflict model serving as the bedrock of his psychosexual theory of pathology (
5). Freud theorized that certain unconscious sexual wishes or impulses (id) could threaten to emerge into consciousness (ego), colliding wholesale with strict conscience-driven prohibitions (superego), producing “signal” anxiety, precipitating unconscious defense mechanisms and, when these coping strategies proved insufficient, leading to frank symptom formation. For the most part, this system was proposed as explanatory for what were called at the time the “symptom neuroses,” such as hysterical neurosis or obsessive-compulsive neurosis. During the 1940s, 1950s, and 1960s, these ideas became dominant in American psychiatry, to be followed later by interest in other psychoanalytic principles, such as object relations theory.
Freud’s concentration on the symptom neuroses involved the central notion of anxiety as the engine that led to defense mechanisms and to symptom formation, and as a critical factor motivating patients to work hard in psychoanalysis to face painful realizations and to tolerate stress within the treatment itself (such as that involved in the “transference neurosis”). Less prominently articulated were Freud’s notions of character pathology, but generally, character disorders were seen to represent “preoedipal” pathology. As such, patients with these conditions were judged less likely to be motivated to change. Instead of experiencing anxiety related to the potential gratification of an unacceptable sexual impulse, patients with “fixations” at the oral dependent stage, for example, experienced anxiety when not gratifying the impulse, in this case the need to be fed. Relief of anxiety, then, could be accomplished by some combination of real and symbolic feeding—attention from a parent or parent figure, or even alcohol or drug consumption. Deprivation within the psychoanalytic situation, then, inevitable by its very nature, could lead to the patient’s flight and thus interrupted treatment.
In a way, social attitudes mirrored and extended these beliefs so that although personality pathology was well known, it was often thought to reflect weakness of character or willfully offensive or socially deviant behavior produced by faulty upbringing rather than understood as “legitimate” psychopathology. A good example of this view could be seen in military psychiatry in the mid-1900s, in which discharge from active duty for mental illness with eligibility for disability and medical benefits did not include the “character disorders” (or alcoholism and substance abuse)—these conditions were seen as “bad behavior” and led to administrative, nonmedical separation from the military.
In spite of these common attitudes, clinicians recognized that many patients with significant impairment in social or occupational functioning or with significant emotional distress needed treatment for psychopathology that did not involve frank psychosis or other syndromes characterized by discrete, persistent symptom patterns such as major depressive episodes, persistent anxiety, or dementia. General clinical experience and wisdom guided treatment recommendations for these patients, at least for those who sought treatment. Patients with paranoid, schizoid, or antisocial patterns of thinking and behaving often did not seek treatment. Others, however, often resembled patients with symptom neuroses and did seek help for problems ranging from self-destructive behavior to chronic misery. The most severely and persistently disabled of these patients were often referred for intensive psychoanalytically oriented long-term inpatient treatment (an option much more available at that time than today). Other patients, able to function outside of a hospital setting and often hard to distinguish from patients with neuroses, were referred for outpatient psychoanalysis or intensive psychoanalytically oriented psychotherapy. As Gunderson (
6) described, the fact that many such patients in psychoanalysis regressed and seemed to get worse rather than showing improvement in treatment was one factor that contributed to the emerging concept of borderline personality disorder, thought initially to be in the border zone between the psychoses and the neuroses. Patients in this general category included some who had previously been labeled as suffering from latent schizophrenia (
2), ambulatory schizophrenia (
7), pseudoneurotic schizophrenia (
8), psychotic character (
9), or “as-if” personality (
10).
These developments coincided with new approaches emerging within the psychoanalytic framework based on alternative theoretical models, such as the British object relations school. New conceptual frameworks, such as Kernberg’s model of borderline personality organization (
11) and Kohut’s concept of the central importance of empathic failure in the histories of narcissistic patients (
12), served as the basis for an intensive psychodynamic treatment approach for selected patients with personality disorders.
The DSM system
Personality disorders have been included in every edition of the DSM. In 1943, the need for standardized psychiatric diagnosis in the context of World War II drove the U.S. War Department to develop Technical Bulletin 203, describing a psychoanalytically oriented system of terminology for classifying mental illness precipitated by stress (
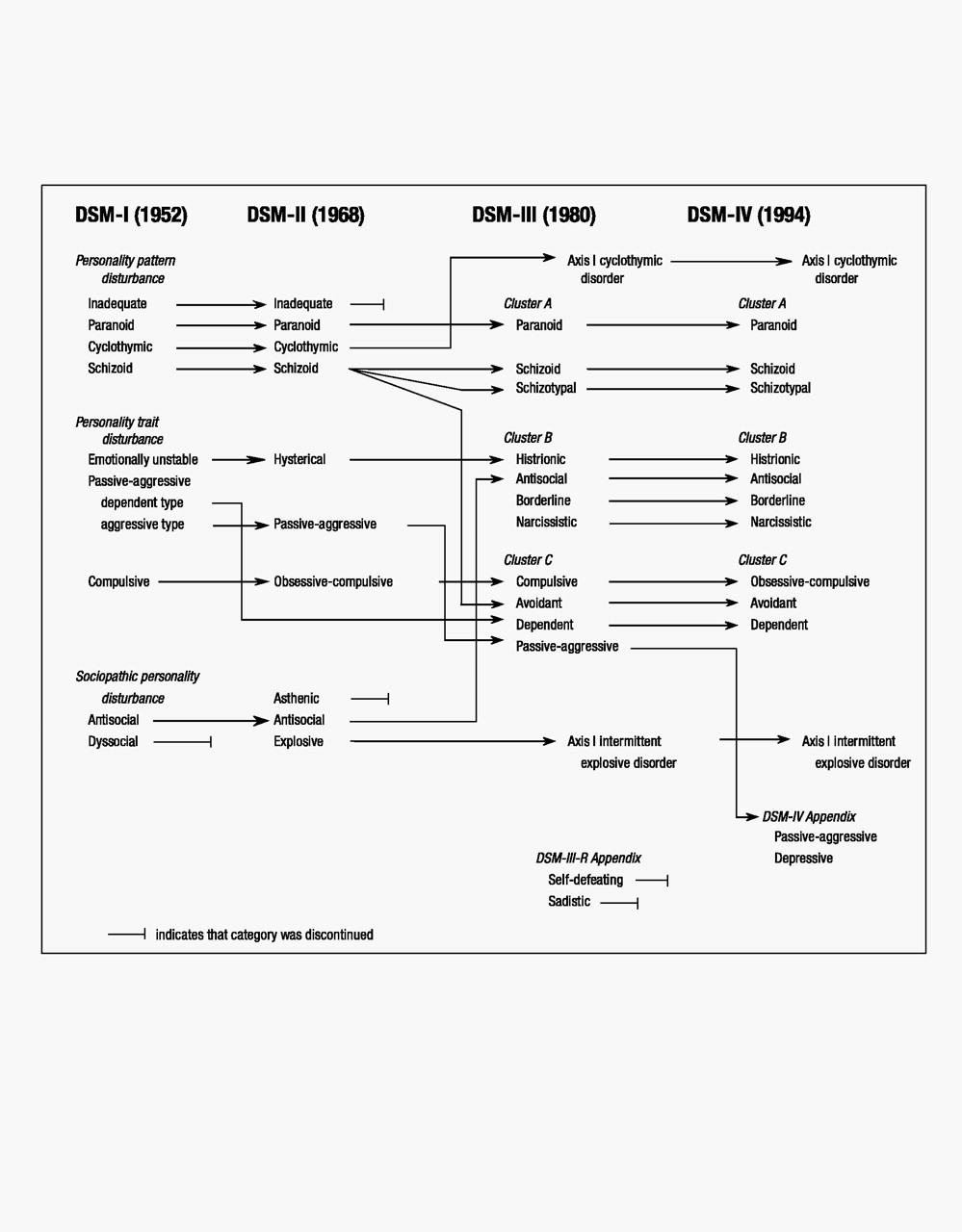
13). APA charged its Committee on Nomenclature and Statistics to solicit expert opinion and to develop a diagnostic manual that would codify and standardize psychiatric diagnoses. This diagnostic system became the framework for the first edition of DSM (1952). DSM-I was widely used and underwent revisions over the years, leading to DSM-II (1968), DSM-III (1980), DSM-III-R (1987), DSM-IV (1994), and DSM-IV-TR (2000). Figure 1 (
14) depicts the ontogeny of diagnostic terms relevant to the personality disorders from DSM-I through DSM-IV (DSM-IV-TR involved only text revisions but used the same diagnostic terms as DSM-IV).
Although not explicit in the narrative text, the first edition of DSM reflected the general view of personality disorders at the time, elements of which persist to the present. Generally, personality disorders were viewed as more or less permanent patterns of behavior and human interaction that were established by early adulthood and were unlikely to change throughout the life cycle. Thorny issues such as how to differentiate personality disorders from personality styles or traits, which remain actively debated today, were clearly identified at the time. Personality disorders were contrasted with the symptom neuroses in a number of ways; in particular, the neuroses were characterized by anxiety and distress, whereas the personality disorders were often “egosyntonic,” hence not recognized by those who had them. Even today, we hear descriptions of some personality disorders as “externalizing,” that is, disorders in which the patient disavows any problem but blames all discomfort on the real or perceived unreasonableness of others. Notions of personality psychopathology still resonate with concepts such as those of Reich (
15), who described defensive “character armor” as a lifetime protective shield.
In DSM-I, personality disorders were generally viewed as deficit conditions reflecting partial developmental arrests or distortions in development secondary to inadequate or pathological early caretaking. The personality disorders were grouped primarily into “personality pattern disturbances,” “personality trait disturbances,” and “sociopathic personality disturbances.” Personality pattern disturbances were viewed as the most entrenched conditions, likely to be recalcitrant to change, even with treatment. These included inadequate personality, schizoid personality, cyclothymic personality, and paranoid personality. Personality trait disturbances were thought to be less pervasive and disabling, so that in the absence of stress these patients could function relatively well. Under significant stress, however, patients with emotionally unstable, passive-aggressive, or compulsive personalities were thought to show emotional distress and deterioration in functioning, and they were variably motivated for and amenable to treatment. The category of sociopathic personality disturbances reflected what were generally seen as types of social deviance at the time. It included antisocial reaction, dyssocial reaction, sexual deviation, and addiction (subcategorized into alcoholism and drug addiction).
The primary stimulus leading to the development of the second edition of DSM was the publication of the eighth edition of the International Classification of Diseases and the APA’s wish to reconcile its diagnostic terminology with this international system. In the revision process, an effort was made to move away from theory-derived diagnoses and to attempt to reach consensus on the main constellations of personality that were observable, measurable, enduring, and consistent over time. The earlier view that patients with personality disorders did not experience emotional distress was discarded, as were the DSM-I subcategories of personality pattern, personality trait, and sociopathic personality disturbances. One new personality disorder was added, called asthenic personality disorder, only to be deleted in the third edition.
By the mid-1970s, greater emphasis was placed on increasing the reliability of all diagnoses, and, whenever possible, diagnostic criteria that were observable and measurable were developed to define each diagnosis. A multiaxial system was introduced in DSM-III. Disorders classified on axis I included those generally seen as episodic, characterized by exacerbations and remissions, such as psychoses, mood disorders, and anxiety disorders. Axis II included the personality disorders as well as mental retardation; both groups were seen to comprise early-onset, persistent conditions, but mental retardation was understood to be “biological” in origin, in contrast to the personality disorders, which were generally regarded as “psychological” in origin. The stated reason for placing the personality disorders on axis II was to ensure that “consideration is given to the possible presence of disorders that are frequently overlooked when attention is directed to the usually more florid Axis I disorders” (DSM-III, p. 23). It is generally agreed that the decision to place the personality disorders on axis II has led to greater recognition of the personality disorders and has stimulated extensive research and progress in our understanding of these conditions.
As shown in Figure 1, the DSM-II diagnoses of inadequate personality disorder and asthenic personality disorder were discontinued in DSM-III. The diagnosis of explosive personality disorder was changed to intermittent explosive disorder, and cyclothymic personality disorder was renamed cyclothymic disorder; both of these diagnoses were moved to axis I. Schizoid personality disorder was thought to be too broad a category in DSM-II, and it was unpacked into three personality disorders: schizoid personality disorder, reflecting “loners” who are uninterested in close personal relationships; schizotypal personality disorder, understood to be on the schizophrenia spectrum of disorders and characterized by eccentric beliefs and nontraditional behavior; and avoidant personality disorder, typified by self-imposed interpersonal isolation driven by self-consciousness and anxiety. Two new personality disorder diagnoses were added in DSM-III: borderline personality disorder and narcissistic personality disorder. In contrast to the previous notion that patients called “borderline” were on the border between the psychoses and the neuroses, the criteria defining borderline personality disorder in DSM-III emphasized emotional dysregulation, unstable interpersonal relationships, and loss of impulse control more than cognitive distortions and marginal reality testing, which were more characteristic of schizotypal personality disorder. Among the many scholars whose work greatly influenced and shaped our understanding of borderline pathology were Kernberg (
11) and Gunderson (
6,
16). Although concepts of narcissism had been described by Freud, Reich, and others, the essence of the current views of narcissistic personality disorder emerged from the work of Millon (
17), Kohut (
12), and Kernberg (
11).
DSM-III-R was published in 1987 after an intensive revision process involving widely solicited input from researchers and clinicians. It was based on principles similar to those articulated in DSM-III, such as assuring reliable diagnostic categories that were clinically useful and consistent with research findings and minimizing reliance on theory. Efforts were made for diagnoses to be “descriptive” and to require a minimum of inference, although the introductory text of DSM-III-R acknowledged that for some disorders, “particularly the Personality Disorders, the criteria require much more inference on the part of the observer” (DSM-III-R, p. xxiii). No changes were made in DSM-III-R diagnostic categories of personality disorders, although some adjustments were made in certain criteria sets, for example, making them uniformly polythetic instead of defining some personality disorders with monothetic criteria sets (e.g., dependent personality disorder) and others with polythetic criteria sets (e.g., borderline personality disorder). In addition, two personality disorders were included in Appendix A, “Proposed Diagnostic Categories Needing Further Study”: self-defeating personality disorder and sadistic personality disorder, based on clinical recommendations to the DSM-III-R personality disorder subcommittee. These diagnoses were considered provisional, pending further review and research.
DSM-IV was developed after an extensive process of literature review, data analysis, field trials, and feedback from the profession. Because of the increase in research stimulated by the criteria-based multiaxial system of DSM-III, a substantial body of evidence existed to guide the DSM-IV process. As a result, the threshold for approval of revisions for DSM-IV was higher than those used for DSM-III and DSM-III-R. Diagnostic categories and dimensional organization of the personality disorders into clusters remained the same in DSM-IV as in DSM-III-R, with the exception of the relocation of passive-aggressive personality disorder from the “official” diagnostic list to Appendix B, “Criteria Sets and Axes Provided for Further Study.” Passive-aggressive personality disorder, as defined by DSM-III and DSM-III-R, was thought to be too unidimensional and generic; it was tentatively retitled “negativistic personality disorder,” and the criteria were revised. In addition, the two provisional axis II diagnoses in DSM-III-R, self-defeating personality disorder and sadistic personality disorder, were dropped, reflecting insufficient research data and clinical consensus to support their retention. One other personality disorder, depressive personality disorder, was proposed and added to Appendix B. Although substantially controversial, this provisional diagnosis was proposed as a pessimistic cognitive style; its validity and its distinction from passive-aggressive personality disorder on axis II or dysthymic disorder on axis I, however, remain to be established.
DSM-IV-TR, published in 2000, did not change the diagnostic terms or criteria of DSM-IV. The intent of DSM-IV-TR was to revise the descriptive narrative text accompanying each diagnosis, when it seemed indicated, to update the information provided. Only minimal revisions were made in the text material accompanying the personality disorders.