VIGNETTE PART 1
M is a 20-year-old male sophomore at an Ivy League College who presents to the school's teaching hospital emergency department (ED) with complaints of sharp chest pain, radiating down his left arm, numbness and tingling in his distal extremities, especially his hands and feet, heart palpitations, diaphoresis, and dizziness, all lasting approximately 5–7 minutes. The event had occurred approximately 45 minutes before his arrival to the hospital. He was driven to the ED by his college roommate. He continued to have a strong fear of dying and insisted that the staff “check my heart!” The ED resident quickly began a workup for myocardial infarction but soon discovered there were no diagnostic correlates on an electrocardiogram and laboratory studies to indicate that the patient had experienced a myocardial infarction. He consulted the on-call resident psychiatrist by phone and was instructed to draw blood for a complete blood count, comprehensive metabolic panel, and thyroid function tests and collect a urine sample for urinalysis and a urine toxicology screen. The patient's laboratory values were within normal limits except for positive screen results for cannabis. The psychiatrist asked the ED resident to give the patient lorazepam 1 mg i.v., given the intravenous line access from the earlier workup. Within 10 minutes the patient had calmed considerably and no longer feared his imminent death, but remained quite worried.
The on-call resident psychiatrist appeared within the next hour and began a psychiatric evaluation of the patient. M reported that he had never before experienced such an episode as the one that brought him to the ED. He appeared frightened, despite the treatment with lorazepam. He asked what happened, and the psychiatrist explained that it appeared he had a panic attack. He asked M what he was doing just before the attack began. M reported that he was “hanging out with my roommate” and trying to motivate himself to study for an exam in 2 days' time. The roommate, still in the room, asked the psychiatrist how long the patient would be in the hospital because he had to get home and study. The psychiatrist told the roommate that the evaluation should not take much longer and they could leave together. He asked the roommate if he could please leave the room for privacy.
As the resident psychiatrist walked the roommate out of the patient's room to direct him to the waiting area, the roommate volunteered, “This test coming up is a big one. Physics. He needs to do well on it because he is pre-med.” Then, he added, “I don't know if I'm off-base here, but he seems more—I don't know—depressed or worried or something. I know his girlfriend broke up with him a couple months ago—she's actually a good friend of mine—and she said she just couldn't take his moods anymore.”
Decision Point A:
Given what you know about this patient, was the decision by the resident psychiatrist to ask the ED resident to give the patient lorazepam 1 mg appropriate? Points awarded for correct and incorrect answers are scaled from best (5) to unhelpful but not harmful (0) to dangerous (−5).
| A1._____ | The patient is suffering from severe anxiety due to the panic attack and administering a benzodiazepine intravenously is indicated to obtain near immediate relief of symptoms. |
| A2._____ | The patient is suffering from severe anxiety due to the panic attack and administering a benzodiazepine is indicated to obtain very quick relief of symptoms. However, giving it intravenously is not necessary. |
| A3._____ | The patient is suffering from severe anxiety due to the panic attack and administering a benzodiazepine is indicated to obtain very quick relief of symptoms. However, giving it intravenously is not a wise choice, given the patient's positive urine toxicology screen results for cannabis. |
| A4._____ | The patient has already calmed down and does not require benzodiazepine therapy. |
| A5._____ | The patient has already calmed down. You should start treatment with a selective serotonin reuptake inhibitor (SSRI) such as paroxetine or sertraline. |
VIGNETTE PART 2
The patient tells the psychiatrist that he has been under a lot of pressure from his parents, especially his mother, to do well in school. He started school at a young age and turned 18 as a freshman in college. His birthday is at the end of December; instead of waiting a year to start kindergarten, he began early and has always been the youngest in his class. “You have to know my parents,” he chuckled. He took a year off after his first year of college, uncertain about what he wanted to do and spending most of his time “partying, and being social, but not doing schoolwork.” His parents expected him to become a doctor because his father is an orthopedic surgeon and his grandfather was a general practitioner. “I don't know if I want to become a doctor. Definitely not like my father. I don't think he understands people very well. My parents' friends are mostly my mother's. I've heard people are afraid to work with him. He got into trouble a couple of times for throwing scalpels! He has a horrible temper. But that is another story. He wouldn't agree, but I think he's an alcoholic. He and my mother both have two or three drinks every night. Martinis. They have a special setup in the dining room. Special glasses, the shaker, all of that. My mother is always threatening to divorce him. If I do become a doctor, I think I'll become something less stressful. I don't know. I guess it is not really my choice, though, since they're paying for it.”
He is the oldest of three, with two younger sisters. “They're nothing like me. They don't have the pressure to become a doctor or a lawyer, although I think the older of the two is heading that way. She's just 2 years younger than me and she already volunteers at the public defender's office 1 day a week filing papers or something.” The patient at first seemed relieved to talk about his history, but then suddenly announces, “Listen, man. I have to get back to my apartment. I have to study. Can I get more of that medication they gave me to calm down?”
The resident psychiatrist asks if there is any family history of mental illness, which the patient denies. He admits to smoking marijuana “occasionally, not like one of my roommates who is always stoned. I can't be stoned and do all this work.” He then asks, “Do you think this is going to happen to me again? Or is it enough that I know about it? Will I be able to reason myself through it if I get nuts like this again?” He then continues, “I had a feeling it was in my head, but it is my heart, you know? I can't take chances on my heart.” The resident psychiatrist agrees with his being careful and tells the patient it was wise to come to the emergency department. He then tells the patient he would like him to come back to the psychiatric outpatient department for a full evaluation to determine how to best help him. The patient agrees and is scheduled for an urgent appointment in 5 days.
DECISION POINT B:
Given what you know about this patient, should you agree to his request and give him a supply of lorazepam to take home? What should you do? Points awarded for correct and incorrect answers are scaled from best (5) to unhelpful but not harmful (0) to dangerous (−5).
| B1._____ | The patient has not offered you a specific stressor that causes the attacks suggesting that his attacks are unpredictable. For safety, you should give him five lorazepam 1 mg tablets to last him until his urgent appointment. |
| B2._____ | Despite not knowing the specific stressor, there probably is one. You simply have not had an opportunity to learn this yet. Individual therapy, to begin 5 days hence, will help elucidate the precipitant. Meanwhile, the patient requires protection from attacks with a benzodiazepine. Prescribe lorazepam 0.5 mg p.o. b.i.d. for now. |
| B3._____ | The patient has an urgent appointment in 5 days. Offer several nonpharmacological interventions he can perform himself should he again have a panic attack. |
| B4._____ | The patient demonstrated the use of cannabis, known for playing a role in potentiating panic attacks. Giving a known drug abuser lorazepam, a known drug of abuse, to take home is unwise because it is potentially dangerous if used inappropriately. Ask for permission to speak with the patient's family to gather additional medical and psychiatric history. In addition, if permission is obtained, ask the family to assist in monitoring the patient until his upcoming urgent appointment. |
| B5._____ | The patient has an urgent appointment in 5 days. Evaluate the patient for any additional psychiatric symptoms, which may require closer monitoring before his appointment. |
VIGNETTE PART 3
You are now a psychiatrist working in the student mental health center of the patient's university. The patient arrives for his appointment 15 minutes late. He apologizes as he takes his seat and does not offer you eye contact. You ask how he is feeling today. He says, “I almost didn't come.” There is a long pause. “I don't know,” he tells you, “I just didn't want to leave my apartment. I haven't left it in the last 3 days. I'm missing classes, too.” He appears somewhat disheveled, hair unkempt. He is mildly malodorous. Once in his chair, he stares at his sneakers with his hair covering his eye. One of his thumbs taps the side of the chair quickly, then slowly, and then quickly again. You wait, noting that he is tearful.
“I'm—” he starts, “having a hard time. Really hard.” He tells you that he has been feeling very depressed for several months now. “It's my parents.… I don't know…my grades.…my girlfriend. It's everything.” He reports that his sleep has been disturbed for at least a year, with difficulty initiating sleep and frequent awakenings. He typically ruminates about the issues bothering him until he finally falls asleep; then often he has been sleeping late, sometimes until noon or 1:00 p.m., subsequently missing classes. His grades have been deteriorating over the course of the year, at first gradually, but in the last 2 months he has stopped attending many of his classes and is in danger of finishing the term on academic probation.
Decision Point C:
Which of the following statements regarding the epidemiology of panic disorder and comorbid psychiatric diagnoses are true and which are false? (2) points awarded for answering correctly.
| T | F | C1. | Panic disorder has a lifetime prevalence of approximately 1.6%–2.2% |
| T | F | C2. | Panic disorder may present first in prepubescent children, although this is relatively uncommon. |
| T | F | C3. | When panic disorder presents in adolescence, it occurs more frequently in boys than in girls, by a factor of 2:1. |
| T | F | C4. | Panic disorder is classified in the DSM-IV-TR as having two subtypes: with agoraphobia and without agoraphobia. The lifetime prevalence of the subtype with agoraphobia is approximately 20%. |
| T | F | C5. | Approximately one third of patients with panic disorder are depressed when they present for treatment. |
| T | F | C6. | Patients with panic disorder who have co-occurring depression have a lower risk for suicide attempts. |
| T | F | C7. | Patients with panic disorder are less likely to seek treatment than those with other psychiatric disorders. |
| T | F | C8. | Panic disorder has been shown to have a very strong familial pattern of inheritance. |
| T | F | C9. | Abuse of substances and alcohol is very high among patients with panic disorder, irrespective of subtype. |
| T | F | C10. | Between 40 and 50% of patients with panic disorder also meet criteria for one or more axis II disorders strictly from cluster B (antisocial personality disorder, histrionic personality disorder, borderline personality disorder, and narcissistic personality disorder). |
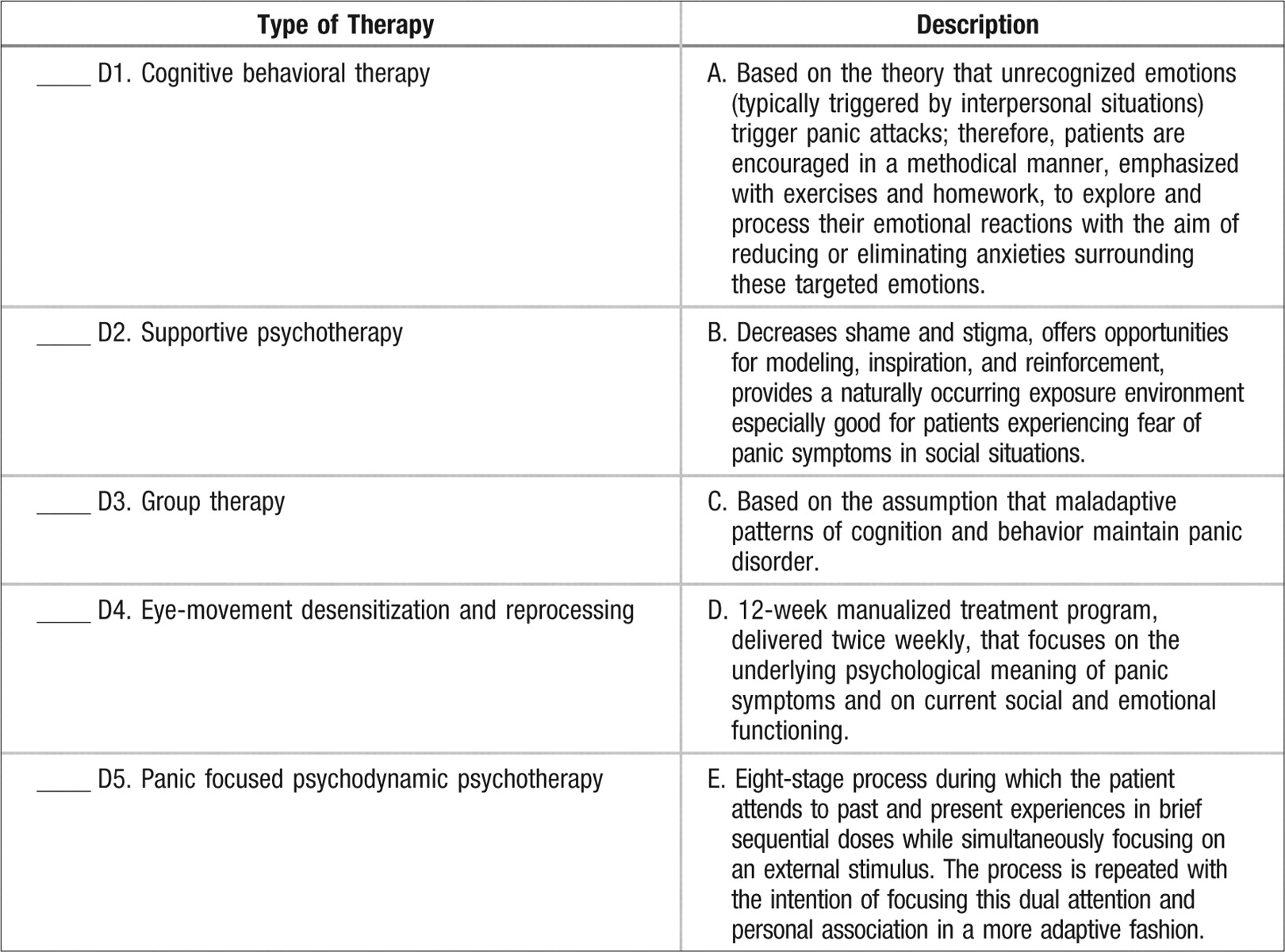
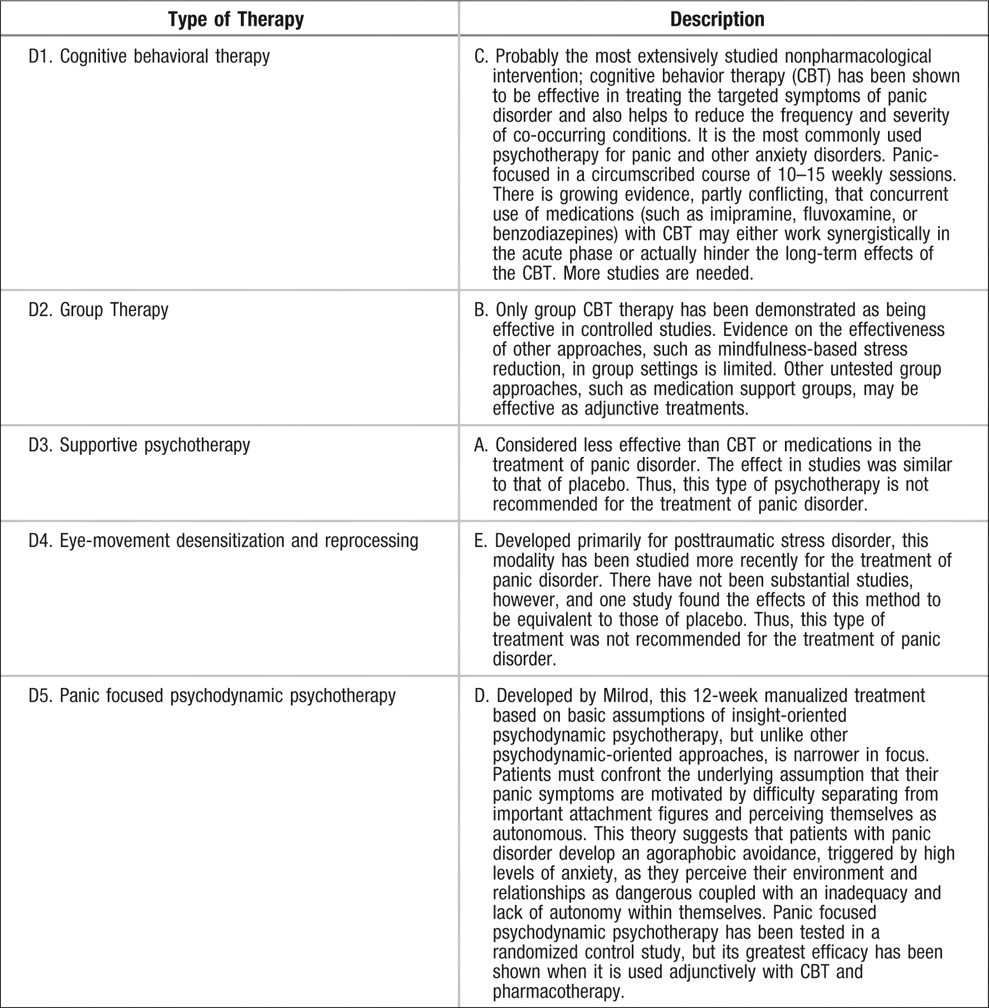
DECISION POINT D:
Match the following types of psychotherapy with their corresponding descriptions (2) points awarded for correct answer.
ANSWERS: SCORING, RELATIVE WEIGHTS, AND COMMENTS
DECISION POINT A:
| A1.____ | −5 There is no indication for administering intravenous benzodiazepine medications to a patient whose symptoms have abated. Although benzodiazepines for panic disorder have been demonstrated to be useful for patients whose symptoms are particularly distressing and impairing and for whom rapid control is critical, giving benzodiazepines to patients with presumed substance abuse (tested positive for cannabis) should be avoided whenever possible. These patients have a higher prevalence of benzodiazepine abuse, a greater euphoric response to benzodiazepines, and a higher rate of unauthorized use of alprazolam during treatment. |
| A2.____ | −5 For the same reasons stated in answer A1, giving benzodiazepines to a patient with a presumed substance abuse problem is not advised. Moreover, the patient's symptoms have abated enough that the wiser choice of treatment would be connecting the patient to a psychiatrist and/or psychotherapist who could follow the patient and offer more effective long-term treatments such as cognitive behavior therapy with or without psychopharmacological agents such as an SSRI. |
| A3.____ | −3 Although this answer addresses the issue of the patient's positive toxicology screen results for cannabis, suggesting abuse, and further suggesting the preference for alternative treatments, it does not account for the abatement of the acute symptoms and subsequently for an opportunity to choose a more effective long-term treatment strategy such as cognitive behavior therapy with or without psychopharmacological agents such as an SSRI. |
| A4.____ | %+5 This answer is true. It does not offer other possible treatment options, but the question does not require this. |
| A5.____ | −3 Although treatment of panic disorder with SSRIs such as sertraline or paroxetine is certainly indicated, you are an ED psychiatrist and unless you continue to see this patient as an outpatient, prescribing long-term psychopharmacological treatments is not considered safe practice. |
DECISION POINT B:
| B1.____ | −5 There is the possibility the patient has a substance abuse problem given his positive toxicology screen results for cannabis. Giving even a small amount of benzodiazepines to take home is not safe practice. Moreover, despite his negative toxicology screen results for benzodiazepines, he may still abuse them, as the threshold for positive results does not necessarily account for low-dose prescriptions. High-dose abuse of benzodiazepines can result in positive urine toxicology screen results for up to 6–8 weeks after the last use. |
| B1.____ | −5 If the patient had not demonstrated a positive toxicology screen for cannabis, this would be an acceptable treatment plan. |
| B3.____ | +3 This is a wise plan. Deep breathing exercises, rebreathing of CO2 in a paper bag, guided imagery, finding a supportive friend or relative to help calm the patient during the attack, and other techniques are likely to help in the short-run, before the patient engages in more substantive therapy. An emphasis on finding a supportive environment should be stressed, however. The prevalence of comorbid axis I or axis II diagnoses increases the patient's risk for suicide, even though the literature on suicidality or attempts in the context of panic disorder as the single diagnosis is still considered controversial. |
| B4.____ | +5 This is a sound, rational plan. |
| B5.____ | +5 There is a high prevalence of comorbid axis I or axis II diagnoses concurrent with panic disorder. It is essential to explore the patient's symptoms and history for more information to help guide immediate treatment options. |
DECISION POINT C:
| C1.____ | T Weissman et al. collected epidemiologic data from multiple countries and noted a similar lifetime prevalence of approximately 1.6%–2.2%. |
| C2.____ | T Panic disorder may have an onset before puberty, although this is less common. |
| C3.____ | F There is a higher risk for panic disorder in females during adolescence (approximately 2:1). The lifetime prevalence is also approximately twice as high in women than in men. Moreover, women are more likely to have panic disorder with agoraphobia than men. |
| C4.____ | T There are two subtypes as described; the prevalence of the agoraphobic subtype is approximately 20%. |
| C5.____ | T The lifetime prevalence of major depression as a comorbid diagnosis with panic disorder without agoraphobia is approximately 34.7% and is 38.7% for panic disorder with agoraphobia. The onset of depression has been found to occur with or after the onset of panic disorder in approximately two-thirds of patients and precede the onset of panic disorder in one-third. |
| C6.____ | F Given the high comorbidity of panic disorders with mood disorders as stated in answer C5, plus the associated risk of suicidal ideation, attempts, and completion with mood disorders uncomplicated by panic disorder, the risk of suicide with complicated panic disorder is higher. In addition, these patients have a higher risk for impaired social and marital functioning, work impairment, use of psychoactive medication, and substance abuse. |
| C7.____ | F Patients with panic disorder are more likely than those with other psychiatric disorders to seek treatment relatively frequently. They more often seek help from nonpsychiatrists and from EDs. |
| C8.____ | T The results of multinational studies have shown a median risk of panic disorder to be eight times as high in the first-degree relatives of probands with panic disorder as in the relatives of control subjects. Early-onset panic disorder demonstrated the greatest familial risk, at approximately 17 times greater. |
| C9.____ | T Irrespective of panic disorder subtype, clinical and epidemiological studies have demonstrated a higher than average rate of substance and alcohol abuse and dependence. Interestingly, approximately 50% of those with panic disorder had prior onset of the comorbid substance or alcohol abuse/dependence disorder. |
| C10.____ | F It is true that 40%–50% of patients with panic disorder will also meet criteria for one or more of the axis II disorders; however, they typically have been shown to have many of the traits associated with cluster B personalities, such as affective instability from borderline personality disorder, impulsivity from borderline personality disorder or antisocial personality disorder, and hypersensitivity to people from paranoid personality disorder. The most common personality disorders most frequently diagnosed fall in cluster C, sometimes known as the “anxious” cluster: avoidant personality disorder, obsessive-compulsive personality disorder, and dependent personality disorder. At least one study of longitudinal data has suggested that the early onset of panic disorder predicts a subsequent onset of personality disorders. |