Research on child temperament and personality breaks down the overall construct into a number of specific higher order dimensions such as extraversion, neuroticism, and novelty seeking (
1,
2). The traits themselves are typically derived from theory and previous research and then tested with factor analytic procedures to establish the taxonomy as reliable and valid (
3,
4). Individual traits are designed to be relatively independent, although modest correlations are generally found between dimensions (
5,
6). Mean scores for these dimensions, in turn, often serve as the main outcome measures when compared between various predefined groups such as between men and women or between patients and controls.
A growing literature of this type has developed revealing strong associations between various temperament dimensions and nearly all types of psychopathology. High levels of neuroticism or negative affectivity, for example, have been found to predict later internalizing and externalizing disorders (
7). Some researchers have demonstrated that certain dimensions such as low effortful control or persistence may reflect a general vulnerability to many behavioral disorders (
8), whereas others relate more to the direction of symptoms such as the link between early social inhibition and later social anxiety disorder (
9). Furthermore, the relations between temperament and psychopathology are mediated and moderated through a number of other factors including attachment, cognitive styles, and environmental selection, among others (
10,
11).
Although there is little doubt that these techniques have contributed to an explosion of important findings regarding the link between temperament and psychopathology (
11–
13), there remain limitations to the variable-centered approach. Specifically, these techniques impose both theoretical and statistical constraints by assuming that the effect of a particular temperament dimension operates independently from the effects of other dimensions (
14). Previous results have suggested that the association between one temperament dimension and a corresponding area of psychopathology depends in part on other temperament dimensions in both the child and the parent (
8,
15). These methods also give no information about how levels of multiple dimensions tend to cluster naturally within a population.
An alternative approach that can address some of these limitations is to combine variable-centered approaches with individual-centered approaches (
11). One specific technique that has been applied successfully in the psychiatric literature is latent class analysis (LCA) or latent profiles analysis (LPA) (
16,
17). With these procedures, responses to items of interest such as criteria for different psychiatric diagnoses, individual questionnaire items, or even quantitative scores for several subscales are examined with the goal of identifying classes of individuals with a similar underlying response profile.
Latent class techniques have been applied to psychiatric diagnoses such as alcoholism, attention-deficit/hyperactivity disorder, obsessive-compulsive disorder, and eating disorders. Results of these investigations have pointed to the existence of categories and subtypes substantially different from current
DSM-based conceptualizations (
18–
20). These differences are not just of academic interest to methodologists. Subsequent analyses have found that clusters identified through LCA and other techniques may be more informative than the existing typology as measured through other external validators such as prognosis or underlying genetics (
21–
23). Thus, this work represents an exciting advance to clinicians and clinical researchers who rely on a valid classification system as a vital prerequisite to all of their subsequent investigations and interventions (
22,
24).
Although application of these methods is relatively new, its conceptual antecedents in modern temperament research can be traced to the seminal work of Thomas and Chess (
2) in their attempts to develop a working classification system. In addition to the nine basic dimensions (mood, distractibility, persistence, activity, rhythmicity, adaptability, approach/withdrawal, threshold, and intensity), Thomas and Chess also advanced the well-known person-centered “constellations” of traits that combined into classes termed easy, slow to warm up, and, most famously, difficult (
25). The difficult category described a temperamental profile of children who were easily frustrated and poorly regulated, required prolonged adjustment to new routines or situations, and had relatively frequent and loud periods of crying and/or tantruming. It was individuals in this category who were deemed most susceptible to psychopathology in certain environmental contexts (
25). This category continues to be a cornerstone of modern temperamental research and teaching despite little empirical replication for this framework or others. One attempt using inverse factor analysis in adolescent boys found three main personality types labeled resilient, overcontrolled, and undercontrolled (
26,
27). The resilient group was found to have low levels of psychopathology and high academic achievement, overcontrollers had high levels of internalizing problems, and undercontrollers had high levels of externalizing problems or comorbid internalizing and externalizing problems.
Caspi and Silva (
28) used factor and cluster analyses to describe five classes of 3-year-old children as part of the Dunedin Study. Their groups were labeled as well-adjusted (40%), undercontrolled (10%), confident (27%), inhibited (8%), and reserved (15%) based on observer ratings. Prospective studies have revealed significant predictive relationships between age 3 temperament categories and later psychopathology and achievement (
29,
30).
In applying LCA techniques to more recent temperament constructs, we have previously reported an LCA of questionnaire items related to the temperamental trait of behavioral inhibition (
31). This study found evidence not only of a class of children who were fearful and reticent to social and nonsocial novelty, as defined by the construct, but also classes fearful only to social or nonsocial novelty (
32). We are not aware, however, of LCA or LPA being applied to any of the most widely used temperament instruments.
To these ends, we attempted to apply LPA to a group of children and adolescents whose temperament was assessed with the Junior Temperament and Character Inventory (JTCI) (
33). We hypothesized that the technique would identify a relatively small number of clusters of individuals with distinguishing profiles. We further hypothesized that at least some of these profiles would relate strongly to both negative and positive outcomes.
METHOD
Subjects
The participants for this investigation came from a family study conducted in the northeastern United States that was designed to examine the genetic and environmental contributions to attention and aggression. Details of this sample are described in more detail elsewhere (
34,
35). Inclusionary criteria were proband child between the ages of 6 and 18; proband child living with at least one biological parent; and proband child with at least one sibling within the same age range. Potential families were recruited from local pediatricians and psychiatrists in a university-based outpatient clinic based on a review of clinical records. Local newspaper advertisements, and posters were also used. The families who responded to community advertisements were screened by telephone for demographic inclusion criteria.
If families were able to meet those requirements, then they were then sent the parent-rated Child Behavior Checklist (CBCL) (
36) and teacher-rated Teacher Report Form (TRF) to assess levels of child behavior problems. Four target groups of probands were sought based on the CBCL. These groups included subjects with
T scores ≥67 on the attention problems (AP) scale and <60 on the aggressive behavior (AG) scale;
T scores ≥67 on AG but <60 on AP;
T scores ≥67 on both scales; and
T scores <60 on both scales. Siblings were not subject to any of the
T score restrictions placed on probands. A diagnosis of autism was exclusionary as was an IQ <70 as assessed by two subtests of the WISC III (
37). From clinical chart review of 704 patients, 358 were found to be eligible and 75 (21%) participated in the study. Of 172 eligible families who responded to community advertisements, 131 (75%) participated. Thus, a total of 206 families entered the study. Of these, 447 children from 182 families had complete data to be included in the present report. All of the subjects signed informed consent, and the study complied with all of the requirements of the institutional review board.
Temperament assessment
Temperament was assessed using the JTCI. This widely used measure has been found to have good psychometric properties (
33,
38). Internal consistency, for the four temperament scales, as calculated with Cronbach α, has been found to be between 0.50 and 0.83 (
33). Test-retest has been found to range from 0.62 to 0.85 (
38), The JTCI is composed of 108 statements that the respondent rates as true or false based on how the person usually acts and feels, such as “I often feel tense and worried in unfamiliar situations (harm avoidance).”
According to this framework, personality can be conceptualized along four temperament and three character dimensions. The four temperament dimensions of the JTCI, thought to reflect propensities in automatic responses to emotional stimuli, are novelty seeking (NS), harm avoidance (HA), reward dependence (RD), and persistence (P). NS relates to a tendency to seek out stimulation and is composed of subscales of impulsivity, extravagance, and disorderliness. HA refers to inhibitory behavior and contains elements of worry, shyness, and fatigability. RD considers the level of response to cues of social reward and includes the degree of sentimentality, social connection, and dependence. Finally, P reflects the ability of an individual to persevere despite obstacles or frustration. The character dimensions, which are hypothesized to develop from relations between temperament, family environment, and individual experiences, were not used for these analyses.
Studies that have examined the JTCI and the Temperament and Character Inventory in comparison with other temperament or personality scales have shown significant correlations between comparable dimensions. For example, studies in adults and children comparing HA to the trait of neuroticism show significant correlations between 0.41 and 0.63 while correlation between NS and extraversion range from 0.26 to 0.45 despite no claims to be measuring the exact same contruct (
5,
39).
Psychopathology and wellness measures
CBCL.
We assessed the level of psychopathology and wellness using the CBCL (
36), which had been collected from parents of the child participants. Briefly, the CBCL is a sex- and age-sensitive questionnaire used for parents to respond to 118 problem behaviors exhibited by their child over the previous 6 months. The parent responds along a 3-point scale with the code of 0 if the item is not true of the child, 1 for sometimes true, and 2 if the item is often true for the child. The characteristics and psychometric stability of the CBCL have been well established. The CBCL yields eight psychopathology subscales that can be combined into three broad areas of “internalizing,” “externalizing” that combine with other subscales to form the “total problems” scale. In addition, there exist domains of wellness or competency for activities, social functioning, and school performance that can be combined into a total competency score. The content validity of the competency scales has been supported and found to be sensitive not only to demographically similar referred and nonreferred children but also between children with different types of psychopathology (
40,
41).
TRF.
The TRF is also a sex- and age-sensitive questionnaire similar in format to the CBCL. To limit the number of analyses, we used the total adaptive functioning score that is comprises the subscales labeled “academics,” “working hard,” “appropriate behavior,” “learning,” and “happy.” For psychopathology, the internalizing, externalizing, and total problems scales were used similar to the CBCL.
DSM-IV Diagnoses.
Although categorical
DSM-IV disorders were not used as a primary outcome variable, they were assigned based on a structured interview, the Vermont Structured Diagnostic Interview. Diagnoses were counted as positive if
DSM-IV criteria were met according to an interview with the mother and child (12 and older). The psychometric properties of the Vermont Structured Diagnostic Interview were found to be good with mean test-retest reliability of 0.62 for disruptive behavior disorders and 0.69 for internalizing disorders (
34). Intraclass correlation coefficients for symptom counts averaged 0.83 for disruptive behavior and 0.74 for internalizing disorders. Interviews were conducted by trained research assistants supervised by a board-certified child and adolescent psychiatrist. Diagnostic data were available for 422 subjects.
Data analysis
To estimate latent profiles from four observed variables, the Mplus statistical package (
42) was used. This program is able to account for the nonindependence of multiple family members using a clustering sampling design by means of an EM algorithm (
43). As mentioned, this statistical procedure attempts to identify groups of individuals with similar responses across a series of items. The fit of the model using one-, two-, and three-class solutions were compared in terms of likelihood ratio fit statistics and indices that take account of model complexity and parsimony such as the Bayesian Information Criterion and the Akiake's information criterion (
44), as well as the distinctiveness of latent profiles. Once the best fitting model was identified by the LPA and the optimal number of classes determined, these classes were given descriptive labels based on consensus of the authors after reviews of each class's unique profile. For each subject, the probability of belonging to each class was calculated and each subject was assigned membership to a particular class based on the class with the highest probability using the “known classes” algorithm during the validation phase of latent profiles. The classes were then treated as groups to examine their relations between the broad-based psychopathology and competency domains. For these analyses, latent profile membership was predicted from competency and problem scales after controlling for gender in a multinomial regression. In essence, these procedures are similar to logistic regression and are used when there are multiple levels of the dependent variable rather than just two. Separate multinomial regressions were conducted for mother reports, father reports, and teacher reports on child pathology and competency. Simulation studies have demonstrated superiority of this procedure over estimating the LPA with covariates without the known-classes algorithm (
45).
RESULTS
The average age of child participants was 11.0 (SD 3.1) years and the sample was 58% male. Of the 447 children in this study, all were rated by mothers on the CBCL, 194 by fathers on the CBCL, and 146 by teachers on the TRF. Child participants for whom a TRF was obtained had higher mother-rated CBCL scores than those for whom no TRF was obtained (total problems mean of 42.73 versus 33.09,
F1,430,
p < .001). The mean age of parents was 39.2 (SD 5.4) and 43.0 (SD 6.3) for mothers and fathers, respectively. The sample was almost exclusively white with an average score of 6.4 (SD 2.1) on the Hollingshead socioeconomic status scale (
46).
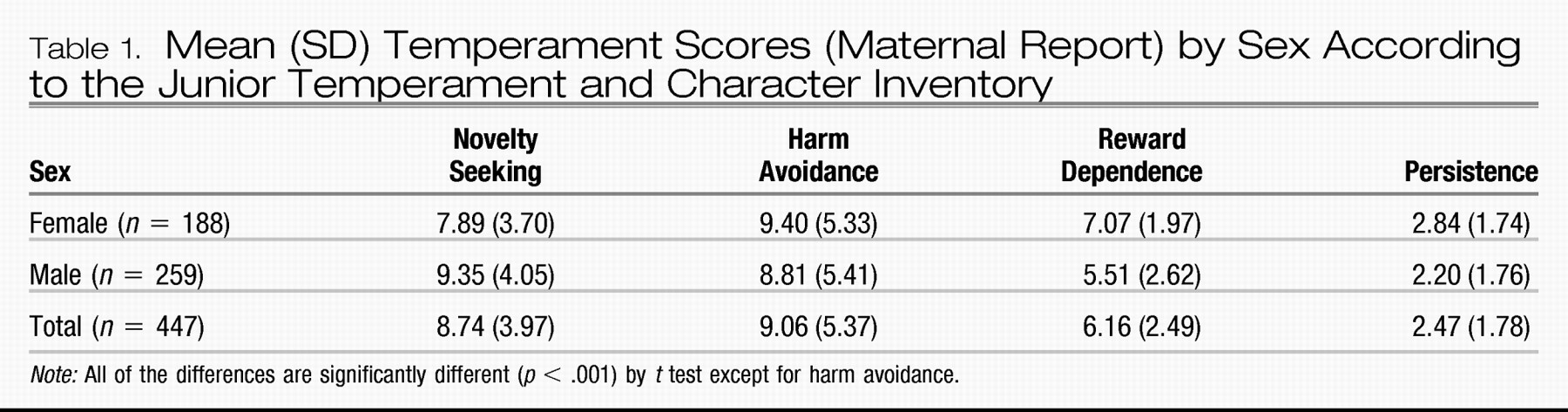
JTCI scores for the four domains used in the analysis are given in
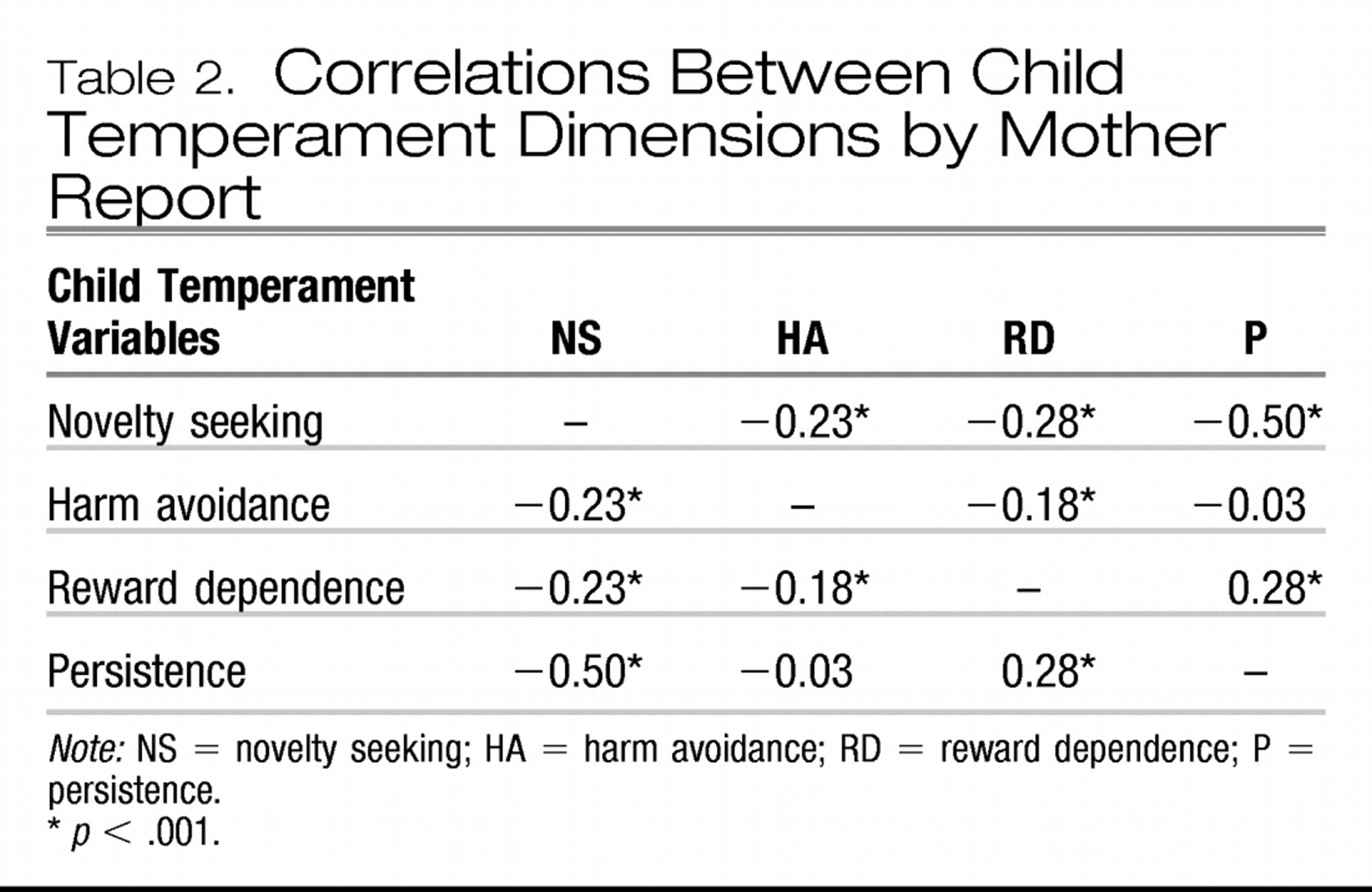
Table 1. Because of the wide range in the number of questions relating to each dimension, standardized scores were used in the LPA and multinomial regressions. Correlations among the four temperament dimensions are shown in
Table 2. NS was negatively and significantly correlated with HA, RD, and, most prominently, P. HA was also negatively correlated with RD, whereas RD and P were positively related. Regarding the CBCL and TRF domains within informants, the correlation between internalizing and externalizing problems ranged between 0.57 and 0.62 (all
p < .001). Between informants, the correlation between parents was 0.71 (
p < .001) and 0.21 (
p < .005) for total problems and total competence, respectively, whereas the correlation between mother and teacher was 0.46 (
p < .001) and 0.54 (
p < .001).
LPA
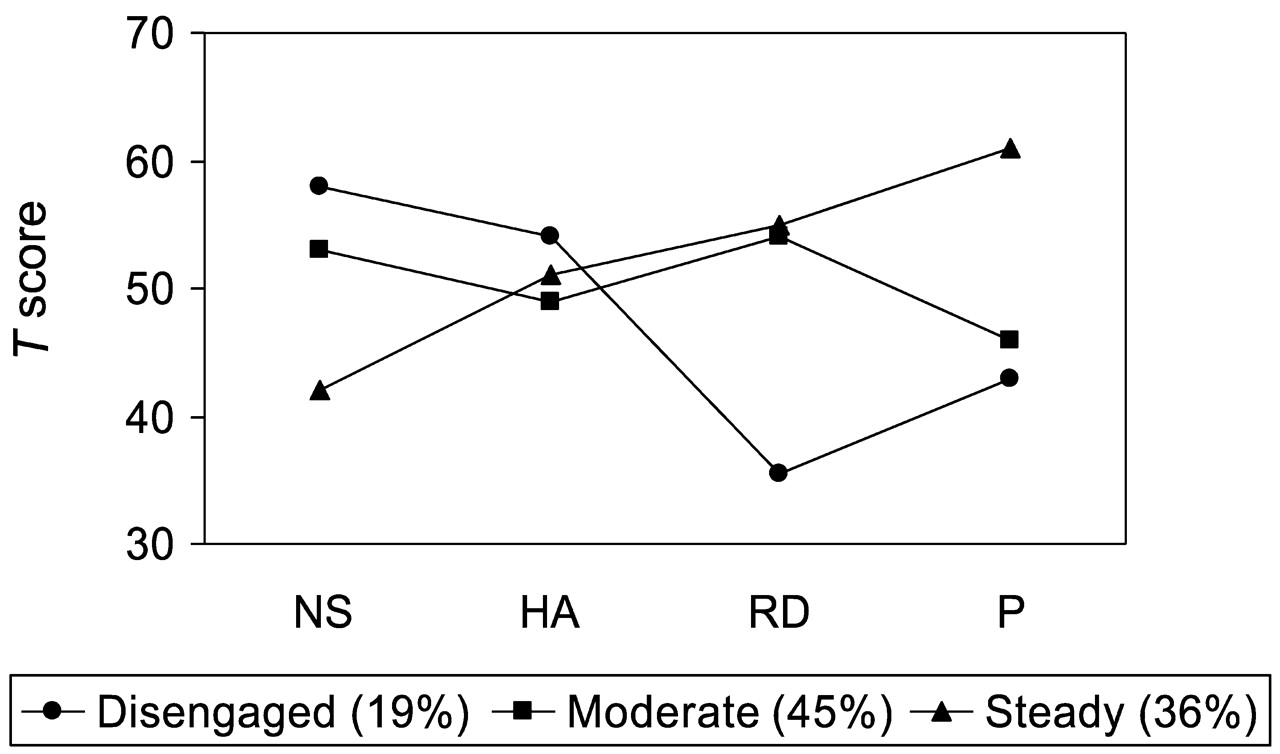
All three information indices favored the three-class model over its alternatives. The log likelihood value was −6,496.12 with 18 free parameters. As an indicator of latent profile distinctiveness, the average latent class probability was 0.87, which is not only the highest among the compared models but also exceeded the adequate value of 0.80. Thus, a three-class solution was chosen as the best fitting model. Average temperament
T scores across the four dimensions are shown in
Figure 1 for the three classes.
As mentioned, subjects were assigned a class based on the highest probability of membership. Names for these classes were based on their unique profiles. The majority of children were assigned to a class with average item scores across the four temperament domains. This moderate class comprised approximately 45% of the sample. The second most prevalent class was distinguished primarily from the others through a combination of low NS and high P. These children, therefore, would likely be described as being nonimpulsive, orderly, and with the strong ability to persevere despite obstacles or frustration. We termed these individuals the steady class, and this class comprised approximately 36% of the sample. The final class consisted of children with a pattern of high NS, low P, and most prominently low RD. These children would often be both stimulus seeking and somewhat fearful and fatigued, with lower P. Most strongly, these children tend to be less socially connected and less likely to share their emotions with others. This group of children was labeled the disengaged class, and this group comprised about 19% of the sample. The disengaged class contained mostly boys (85%), whereas the steady (43%) and moderate (57%) classes were more evenly divided. Because of the sex differences between classes, we controlled for sex in subsequent regressions between class membership and outcome.
Latent classes and measures of pathology and competency
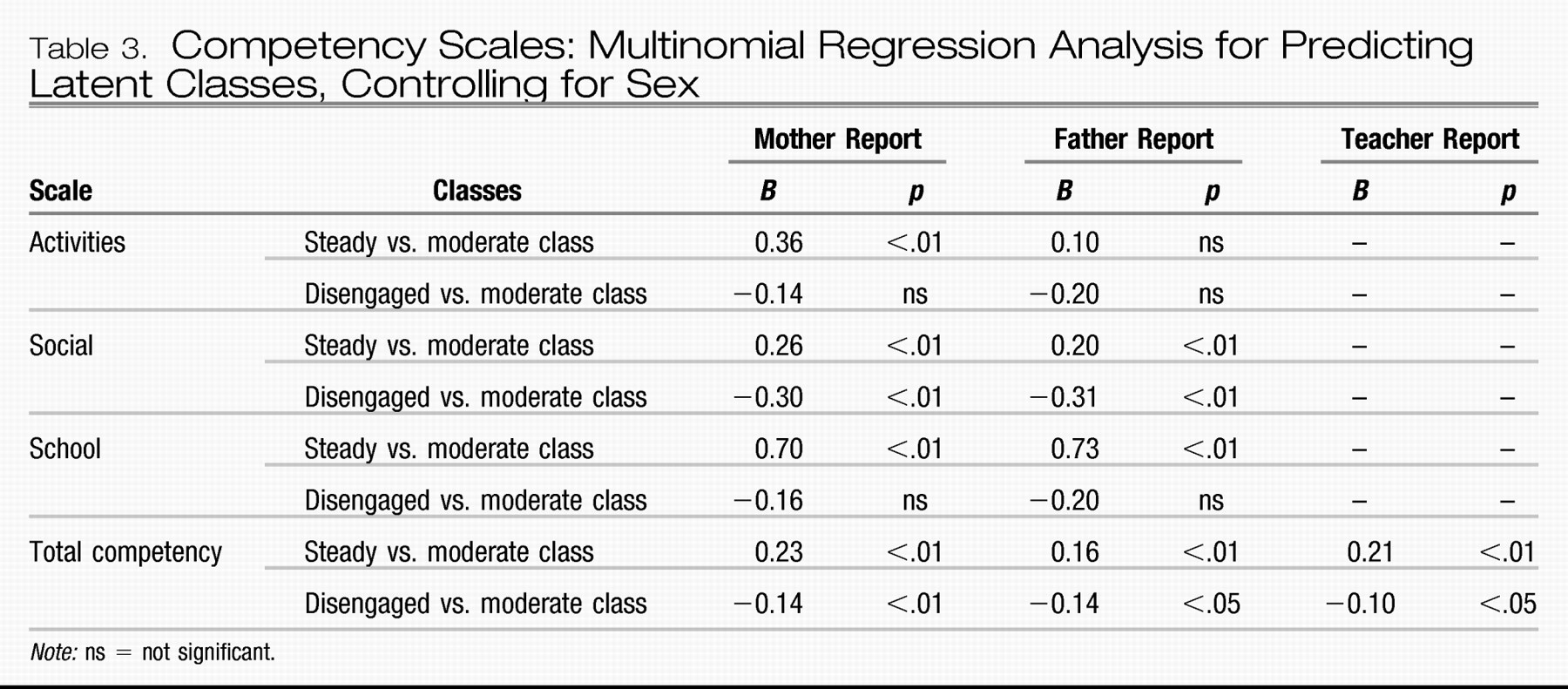
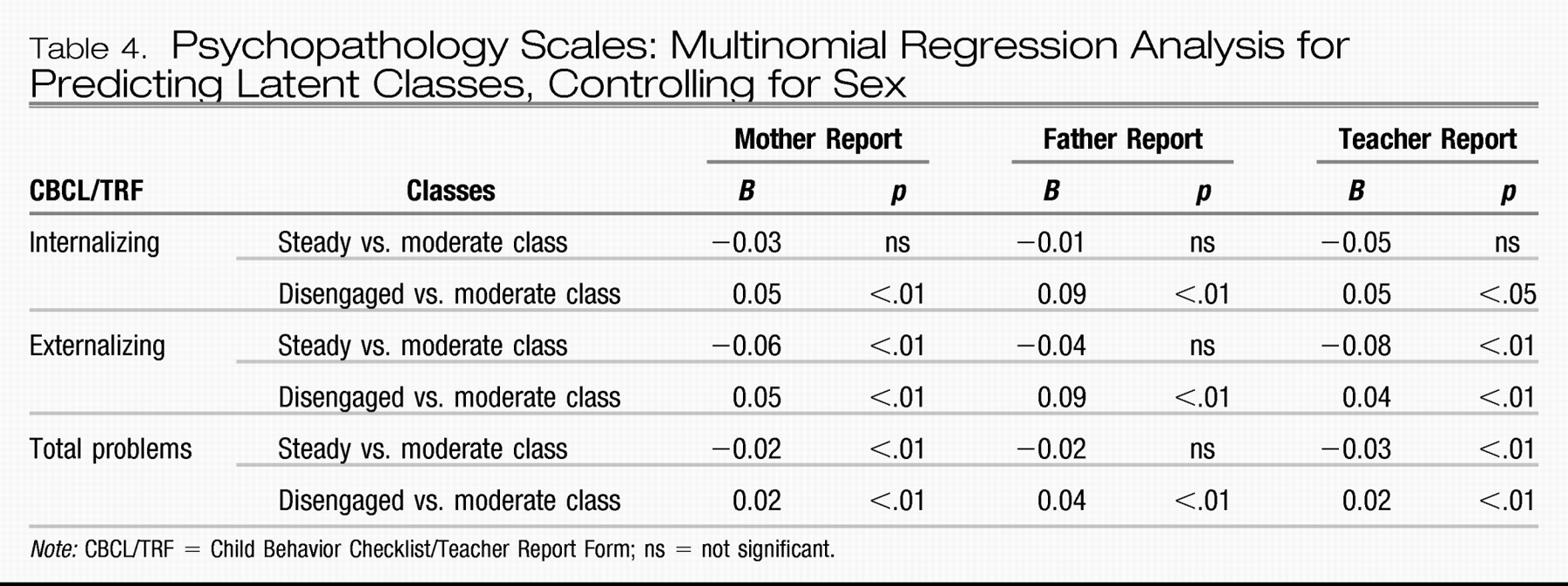
To determine possible relations between class assignment and measures of both psychopathology and wellness, the competency and problem area scales of the mother- and father-rated CBCL in addition to the TRF were analyzed by class using a multinomial regression. In general, strong associations were found between class assignment and multiple measures of psychopathology and wellness. Results from the regression analyses are shown in
Tables 3 and
4. Mean scores across the three latent classes are available by request.
Competency measures
High CBCL competency scores indicate a higher level of involvement and success in each of the three areas of activities, social functioning, and school. With regards to parent report of wellness and functioning, the steady class was associated with significantly higher competency in the areas of social functioning, school, and total competency by both mother and father report. Increased involvement and success in activities were found for the steady class for the mother report but not the father report. In contrast, the disengaged class was negatively and significantly related to poorer performance in social and total competence by both parent reports although not significantly associated with activities or school functioning. The total adaptive score on the TRF similarly showed higher scores related to the steady class and lower scores for the disengaged class relative to the moderate group.
Psychopathology
The reverse pattern generally emerged for the psychopathology measures. Once again, there were consistent results across informants. The steady class was associated with significantly lower total problems in comparison to the moderate class by all of the informants and lower levels of externalizing problems according to mother and teacher reports. All of the informants found no association between the steady class and levels of internalizing problems. Comparing the disengaged and moderate classes, the disengaged class was significantly related to higher levels of internalizing, externalizing, and total problems according to all informants (mother, father, teacher).
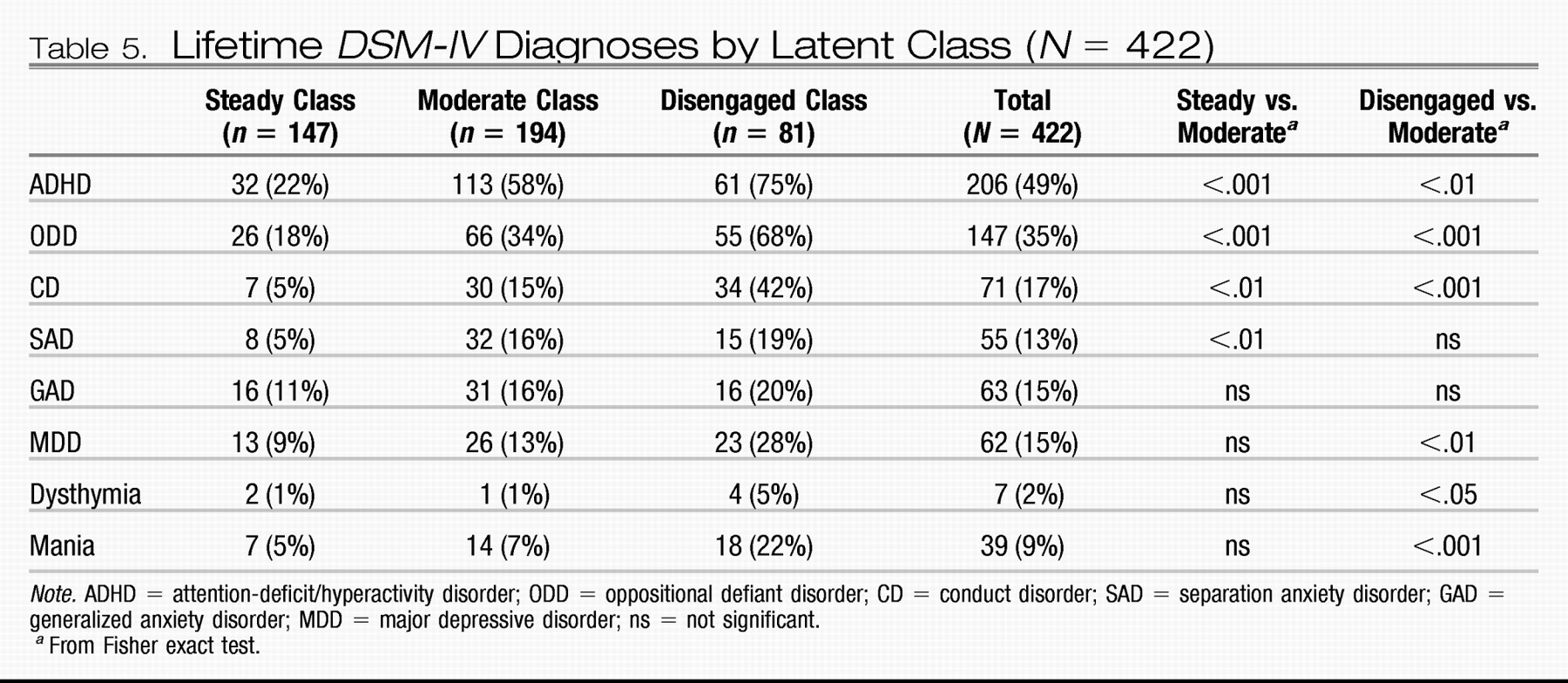
Assessment of psychopathology using categorical
DSM disorders revealed a similar pattern. Among externalizing disorders such as attention-deficit/hyperactivity disorder, oppositional defiant disorder, and conduct disorder, the rate of lifetime disorder was significantly lower in the steady class compared to the moderate class, which in turn was significantly lower than the disengaged class, as shown in
Table 5. For internalizing disorders such as mood and anxiety disorders, there were few significant differences between the steady and moderate classes, whereas higher rates of mood disorders were present in the disengaged class compared to the moderate class. Of note, the overall rate of psychiatric disorders was high in this study that oversampled for certain types of psychopathology.
DISCUSSION
To our knowledge, this study is the first to extract temperament profiles from a commonly used temperament instrument and examine their relations to functioning and psychopathology. The results underscore the importance of examining temperament dimensions in relation to each other rather than in isolation. Our findings lend further support to the usefulness of these procedures in phenotype refinement and highlight the important links between temperament and psychopathology. The consistency of findings across informants (mother, father, teacher) help bolster the validity of these results, especially given the finding that those subjects who did have a teacher rating appear to have higher levels of overall behavior problems.
The three temperament classes identified in these analyses show some important similarities with previous formulations developed through both observations and empirical procedures. The number of classes found in this study is similar to previous investigations, approximately three to five. Some qualitative similarities also exist. The easy class described by Thomas and Chess (
25) and the resilient category described by Robins et al. and Hart et al. share distinguishing features with this study's steady group such as lower distress tolerance and higher achievement orientation (
26,
27). Thomas and Chess found a rate of about 40% for this group, which is quite similar to the 36% rate of the steady class in this study. One difference, however, between the two categories relates to the relatively low NS in our steady group in contrast to the generally higher level of approach behaviors described in the easy group by Thomas and Chess.
Furthermore, the social detachment and lower distress thresholds are elements of both the traditional difficult child in addition to the disengaged class of the present study, which shows not only decreases in social connection and perseverance but also modest elevations of both NS and HA. The latter characteristic is worth noting because most dimension-based correlation studies in both clinical and nonclinical samples have shown that the two dimensions are usually inversely related. Indeed, correlations from our own data show a −0.22 correlation between HA and NS across the entire sample. The identification of a smaller subgroup of individuals with higher levels of both dimensions suggests the possibility that the two dimensions may interact differently in this more impaired group. The combination also illustrates a possible push/pull pattern in which youngsters seek out and crave stimulation while at the same time being fearful and apprehensive.
Unlike most other class structures, our data show evidence of a large group with fairly average levels of all four temperament dimensions. Undoubtedly, some of the discrepancies between our class structure and others relates to the variability between studies in sampling method and method of temperament assessment, including the particular instrument chosen. Future studies using both community and referred samples and employing different temperament assessment procedures and instruments would be useful in determining the generalizability of the class structure found here. Despite these potential differences, however, our moderate group bears some similarity with a class of children labeled well-adjusted from the Dunedin Study (
47).
One interesting and somewhat surprising finding from this report is the prominent role of RD in these temperamental profiles. This dimension has arguably received the least amount of attention relative to traits such as NS and HA. In this study, however, RD was found to be one of the key distinguishing features between the disengaged class and others. RD includes elements of sociability (“It wouldn't bother my child to be alone all of the time”), empathy (“My child does not seem emotionally moved by sad songs or movies”), and emotional sharing with others. The disengaged class was also primarily male. Additional research in this dimension, especially in relation to NS and HA appears warranted. Future investigations may wish to consider combining the questionnaire method of temperament assessment with observation methods because it is possible that any reporting bias may vary according to the very temperament dimensions being studied.
The validity of this approach to incorporate multiple temperament dimensions in latent profiles is supported by the strong associations that were found between these profiles and both positive functioning and psychopathology. These links were found whether competency and problem behavior was rated by the mother, father, or teacher and whether psychopathology was assessed using quantitative scales or categorical
DSM diagnoses. Although the associations were robust between the disengaged class and psychopathology, they were nonspecific and related to both internalizing and externalizing psychopathology. This finding is similar to the Robins et al. (
27) study that found associations between the undercontrolled class and co-occurring internalizing and externalizing. Analyses of the specific subscales of the CBCL confirmed the relationships between membership in this class and behavioral problems ranging from aggression to being withdrawn and anxious. Similarly, the
DSM-IV diagnoses associated with particularly the disengaged class were numerous and diverse. These data, thus, point to the possibility of a particular temperament profile common to multiple categories of psychiatric illness and may partially account for the high rates of comorbidity found in child and adolescent psychiatry (
48). Indeed, although internalizing and externalizing problems are often viewed as opposite poles, correlations between 0.45 and 0.58 have been found in large samples as well as with our own data (
40). Another interesting comparison lies in the similarities between the latent profile of the disengaged children and the temperamental profiles of children diagnosed with attention-deficit/hyperactivity disorder and juvenile bipolar disorder. Both children with attention-deficit/hyperactivity disorder and juvenile bipolar disorder have been shown to have temperament profiles characterized by high NS and low RD and P by parental report (
49). The steady class showed somewhat more specificity in its reduced level of externalizing symptoms and disorders but not, with the exception of separation anxiety disorder, internalizing psychopathology.
Domains of positive functioning such as school performance, activity level, and social functioning also revealed strong associations with temperament class. By examining specific areas of competence, the diminished social functioning of the disengaged class is particularly evident, especially in light of the lack of significant findings with regard to the number or success in various activities. Despite comparable levels of sports and activities, these children continue to struggle with making friends and participating in groups. In contrast, the steady class was related to higher functioning relative to the moderate class in multiple areas of functioning. These findings with competency were consistent across parent reports despite the relatively low correlation between parents in the rating of their child's competence (
40). Because these data are cross-sectional in nature, we cannot determine the direction of causality (i.e., to what degree temperament causes increased or decreased functioning or to what degree less involvement leads to temperament change). Although the public perception of temperament is of highly genetic and stable attributes, empirical studies have demonstrated the important role of particularly unique environmental factors influencing many temperament dimensions (
50,
51).
This study benefits from being a relatively large and well-characterized sample; however, some limitations should be noted. First, as previously mentioned, these mainly parent-report data were collected in a crosssectional sample that was enriched with children who had attention problems and higher levels of aggression. Thus, we were unable to make any firm implications about their prevalence in the general population or about the direction of causality between these temperament classes and outcome. It is likely, for example, that the 19% prevalence of the disengaged class was influenced by our recruitment strategy. Given the similarities between the empirically defined classes in this report and previous investigations, however, we would not expect large deviations in the number of classes or their temperamental composition in less clinically derived samples. In addition, a large number of regressions were performed and it is possible that some of the statistically significant results could have occurred by chance. We also note that the vast majority of subjects for this study were white, and results may not generalize to other ethnic populations. Finally, more comprehensive measures, especially of child competency and functioning, could potentially illuminate more specific associations with temperament profiles.
In summary, this study identifies discrete groups of children who share similar temperament profiles across several dimensions. Furthermore, the meaningfulness of latent profiles is supported by the strong associations between membership and a broad range of psychopathology and positive functioning. The common temperament profile associated with wide-ranging behavioral problems may help explain the high level of comorbid psychiatric disorders that are commonly encountered. It is our hope that these kinds of approaches to person-centered temperament structure can serve as a useful adjunct to factor or dimensional models to further the understanding of temperament development and its relationships to both psychopathology and wellness.