Acute stress disorder (ASD) was introduced in DSM-IV as a new diagnosis to describe acute stress reactions (ASRs) that may precede posttraumatic stress disorder (PTSD). In the prelude to DSM-5, it is appropriate to review the utility of ASD as a diagnosis and to determine the extent to which it adds value to the current diagnosis of PTSD. The ASD diagnosis was introduced for two primary reasons: to describe ASRs that occur in the initial month after trauma exposure, which have earlier gone unrecognized or were labeled adjustment disorders, (
1) and to identify trauma survivors who are high risk for developing subsequent PTSD (
2). At the time of its introduction, there was far less evidence than we have now to support the definition of the diagnosis (
3). This review addresses (a) the definition of ASD, (b) the distinction between ASD and ASRs, (c) the overlap between ASD and Adjustment Disorder, (d) the capacity of ASD to predict subsequent PTSD, (e) the role of dissociation in ASD, (f) the benefits of the ASD to enhance early intervention, (g) the range and utility of emotional responses in the A2 definition, (h) cross-cultural considerations for ASD, (i) the utility of an ASD diagnosis, and (i) finally, a proposal for the modified ASD definition in DSM-V. This article was commissioned by the DSM-5 Anxiety, Obsessive-Compulsive Spectrum, Post-Traumatic, and Dissociative Disorders Work Group. It represents the work of the authors for consideration by the work group. In the course of this review, the DSM-IV Source Book and DSM-IV Options Book were also reviewed. Recommendations provided in this article should be considered preliminary at this time; they do not necessarily reflect the final recommendations or decisions that will be made for DSM-5, as the DSM-5 development process is still ongoing. It is possible that this article's recommendations will be revised as additional data and input from experts and the field are obtained.
DISTINCTION BETWEEN ASD AND ACUTE STRESS REACTIONS
One of the goals of ASD was to describe ASRs. There is much evidence in the literature of a range of distressing responses in the aftermath of trauma, including posttraumatic anxiety, mood disturbances, sleep problems, aggression, substance abuse, and many other physical and psychological symptoms (
4,
5). That is, by focusing on acute posttraumatic stress reactions, the ASD diagnosis does not encompass a broader array of psychological reactions that commonly occur and can be as distressing as ASD responses. For example, despite not yet being formally recognized as a psychiatric disorder, prolonged grief may develop after traumatic loss with documented adverse mental health outcomes (
6). This condition is currently recognized 6 months after the loss because most bereaved individuals adapt during this time (
7). Before that time, however, and certainly within the initial month, many bereaved people suffer intense grief reactions.
Despite the broad range of emotional reactions reported by trauma survivors in the acute phase, ASD is conceptualized in DSM-IV as on the one hand depicting an array of relatively common pathological acute responses to trauma, and yet also constrained by symptom similarity as a precursor to PTSD. Accordingly, it has focused on anxiety and dissociative responses. There is strong evidence that the symptoms reported in ASD are common in the aftermath of trauma, including re-experiencing (
8,
9) and avoidance (
10,
11). Arousal symptoms are also common, including insomnia, (
10,
12,
13) concentration deficits, (
10,
11) irritabilty, (
12) and agitation (
12,
13). A criticism of the current focus of ASD on anxiety responses is that it neglects other early distressing emotional reactions, including depression, guilt, shame, anger, disgust, shock, or somatic reactions (
5). In the current diagnostic system, these reactions—which may be as impairing as fear/anxiety responses—may be diagnosed as Adjustment Disorder when they contribute to marked impairment.
The theoretical position that underlies the DSM-IV conceptualization of ASD can be contrasted with the description of ASRs in the tenth edition of the
International Classification of Diseases (
14). Instead of being considered a precursor of subsequent psychopathology, the ICD-10 conceptualizes ASR as a transient reaction that can be evident immediately after the traumatic event and usually resolves within 2–3 days after a trauma. The ICD description of ASR includes primarily dissociative (daze, stupor, amnesia) and anxiety (tachycardia, sweating, flushing) reactions. Some commentators have suggested that this wide-ranging description may be more useful for clinicians than the more focused DSM-IV criteria (
5,
15). This approach allows for the consideration of acute distress which may warrant intervention (e.g., sleep disturbance) but does not attempt to predict subsequent disorder. Further, ASR notes that the very initial period after trauma exposure may result in a rather amorphous distress state that encompasses many emotional responses that cannot be readily classified into different responses (
16). In the subsequent period, responses may crystallize into more classifiable responses, such as anxiety or mood reactions (
17). Although there is some evidence that people who suffer ASR are more likely to suffer persistent psychological reactions beyond 48 hr, (
18,
19) this knowledge base is very limited. By definition, ASR occurs before ASD can begin—the first 48 hr. ASD covers the time period from 48 hr to 1 month, when PTSD could begin. Thus, those whose symptoms persist or start after 48 hr may represent a different group of trauma responders.
Related to ASR is the construct of combat stress reactions (CSR). This is a similar construct to ASR, except that it is not time-limited. This classification can describe combat personnel who are not able to function at any point after being exposed to severe stress in the course of combat. This construct has a very long historical tradition in military circles as a means to describe the broad range of psychological responses in the immediate and longer term periods following combat (
1). One important difference of CSR in contrast to ASD and ASR is that there is no requirement of functional impairment, which may lead to overidentification of people in need of mental health services (
2). There are longer term follow-up studies of CSR personnel, and these tend to report statistically higher rates of PTSD and dysfunction in those with initial CSR (
20). Despite this relationship, there is a dearth of evidence about the specificity of CSR to predict subsequent PTSD.
DISTINCTION BETWEEN ASD AND ADJUSTMENT DISORDER
Adjustment disorder currently describes a broad range of psychological responses to a stressful event (that may not necessarily be traumatic). These responses can occur immediately after the event, and although it has traditionally been regarded as a short-term adjustment problem, there is also provision for the diagnosis to be made when the person has chronic impairment secondary to the consequences of the event. It is distinguished from ASD in several ways. First, whereas ASD is limited to fear/anxiety responses, Adjustment Disorder encompasses all forms of distressing responses (e.g., depression, anger, guilt). Second, although Adjustment Disorder is predictive of subsequent impairment, (
21) the disorder intentionally describes current dysfunction and it does not contain the explicit goal of identifying people who will suffer subsequent impairment. Third, whereas ASD can be diagnosed from 2 days after the event up to 1 month, Adjustment Disorder can be diagnosed immediately after the event. It should be noted that Adjustment Disorder can have broad clinical utility because it allows a clinician to describe the various psychological disturbances that a person may be experiencing in the immediate aftermath of an aversive event. For example, after the New York terrorist attacks of 9/11, clinicians were able to offer many survivors formal mental health care by describing their diverse reactions with Adjustment Disorder. Thus, Adjustment Disorder in DSM-IV can be used, by temporal definition, to cover situations described as ASR (F43.0) in ICD-10, whereas ASD cannot.
A limitation of Adjustment Disorder is that its broad definition has not resulted in focused treatment interventions to alleviate the condition. One potential advantage of ASD is that it has identified a specific form of initial adjustment difficulties that occur in the acute phase of trauma that is distinguished by its symptom structure and is amenable to early interventions. That is, whereas most difficulties that are described by the Adjustment Disorder diagnosis are diverse, poorly defined, and not specific to a treatment intervention, ASD has allowed the identification of an anxiety-based acute response that responds positively to treatment.
PREDICTIVE UTILITY OF ASD OF SUBSEQUENT PTSD
As noted above, one goal of the ASD diagnosis was to identify people in the initial month following trauma exposure who are not experiencing a transient stress reaction, but rather display severe acute responses and the prodromal symptoms of PTSD. To evaluate the capacity of ASD to identify people who are at high risk for PTSD development, Bryant recently conducted a systematic analysis of the literature of prospective studies of ASD and PTSD by searching PsycINFO, MEDLINE, PubMed, and PILOTS for English-language articles published between 1994 and 2009 using keywords that combined
ASD and
stress disorders/ PTSD. Studies were then included if they assessed ASD within 1 month of trauma exposure and prospectively followed the same participants over time to assess PTSD diagnosis. Inclusion required studies to use measures of ASD and PTSD that permitted diagnostic prevalence rates based on DSM-IV criteria. Twenty-two studies were identified that assessed ASD within a month of trauma exposure and determined the relationship between ASD and subsequent PTSD; (
22–
43) 19 with adults and 3 with children (a detailed report of this analysis is reported elsewhere (
44)).
The rates of full ASD ranged from 7 to 28%, with a mean rate of 13%. It is noteworthy that a proportion of these studies have also reported the prevalence of subsyndromal ASD, which is typically defined as satisfying at least three (typically not requiring the dissociative criterion) of the symptom clusters. Including subsyndromal cases of ASD, together with cases that meet full ASD criteria results in markedly higher rates of identified cases, with the range from 10–32% and a mean of 23%. Across some of these studies, the rates of trauma survivors displaying acute stress are increased primarily by not requiring the dissociative criteria to be met. Bryant's review of these studies reported that the positive predictive power of studies was moderately strong, with most studies of adults indicating that at least half of those trauma survivors with ASD meeting criteria for subsequent PTSD (
44). These studies suggest that people who do meet criteria for ASD are at higher risk for persistent PTSD. In contrast, the sensitivity across most studies was poor, indicating that the majority of trauma survivors who eventually developed PTSD did not meet the full criteria for ASD. Specifically, the 22 identified studies included follow-up assessments of 3,335 individuals. Although 497 of these trauma survivors met criteria for PTSD at the follow-up assessment, only 238 (48%) of these individuals had met criteria for ASD in the month following trauma exposure. This suggests that if a major goal of ASD is to predict people who will subsequently develop PTSD, it is failing to identify half of those who will meet criteria for PTSD at some later time. In some cases, this may be because significant psychopathology simply does not emerge until later. In other cases the ASD criteria may lack sufficient sensitivity.
Some studies reported data that permitted calculation of the predictive capacity of subsyndromal ASD, defined as satisfying only three of the ASD symptom clusters (often by omitting the requirement that dissociation be present). Overall, these analyses indicate that the sensitivity is generally better when one adopts a subsyndromal approach. That is, by focusing on general posttraumatic stress symptoms rather than emphasizing dissociation, more people who eventually develop PTSD can be identified in the acute phase. This pattern may be explained, in part, by the fact that the reexperiencing, avoidance, and arousal clusters in ASD match onto the same symptom clusters in PTSD, whereas dissociation encompasses a different symptom set that is not as strongly represented in the PTSD diagnostic criteria. This approach resulted in significant proportions of trauma survivors who developed PTSD not being identified in the acute phase. It should also be noted that the relationship of ASD to other later occurring psychiatric disorders has been less studied (e.g., depression, alcohol use, prolonged grief).
Recent research developments have identified a range of peritraumatic markers of high risk for PTSD that may facilitate identification of acutely trauma-exposed people who may benefit from early intervention. This research has extended beyond the ASD diagnosis in different ways to improve prediction of subsequent PTSD. Numerous studies indicate that people who develop PTSD have higher heart rates immediately after trauma than those who do not develop PTSD (
45). A comparable pattern has been found for acute respiration rate (
46). Numerous studies have found that maladaptive appraisals about oneself and one's environment is strongly predictive of subsequent PTSD (
47–
49). Other approaches have adopted a broader framework and assessed pretrauma, peritraumatic, and posttrauma risk factors that potentially predict PTSD. For example, one screening measure was developed that included items about psychiatric history, perceived level of threat, and access to social support, and was found to usefully predict PTSD (
50). These developments under-score the point that there are potentially better means to identify people at risk for PTSD development than an acute diagnosis. However, although such biomarkers are of considerable research interest, they have not been employed successfully to correlate or predict diagnosis.
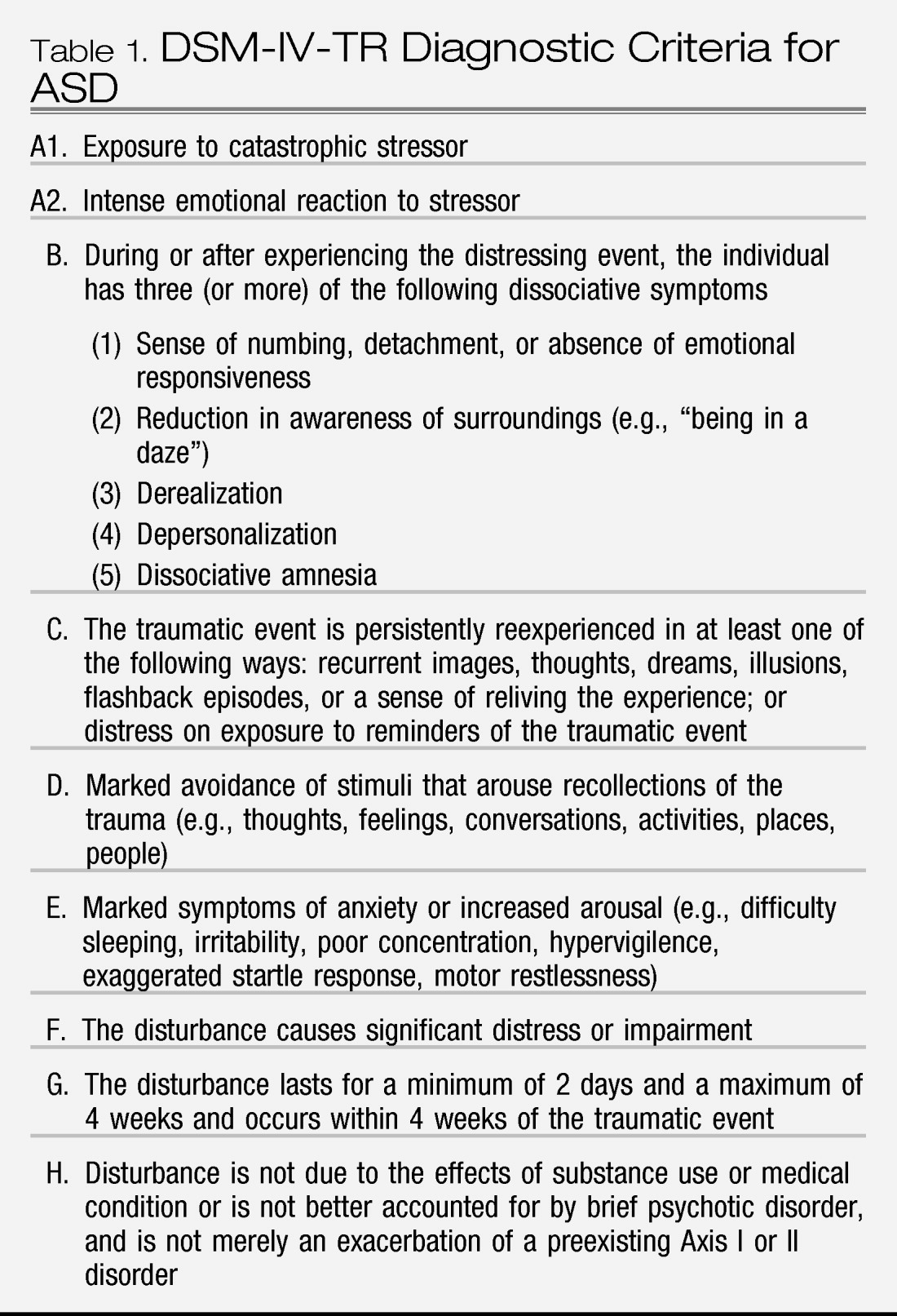
ROLE OF DISSOCIATION IN ASD
A cornerstone of the current ASD diagnosis is that the survivor has at least three dissociative symptoms. From a theoretical perspective, this position was influenced by the view that dissociative responses in the wake of trauma may impede access to affect and memories about their traumatic experience, which may limit emotional processing and recovery (
51). From an empirical perspective, there is much evidence that peritraumatic dissociative reactions are very common, including emotional numbing, altered time sense, reduction in awareness of one's surroundings, depersonalization, and amnesia (
10,
13). Furthermore, there are many studies indicating that peritraumatic dissociation is predictive of subsequent PTSD (
35,
52–
55). Despite this evidence, there are several issues that raise significant concerns about the emphasis currently placed on dissociation in ASD.
First, some recent meta-analyses have suggested that, in the majority of longitudinal studies, peritraumatic dissociation has not emerged as an independent predictor of PTSD, (
56,
57) although others show that it does (
58). Second, a major reason for ASD not predicting PTSD adequately is the requirement that dissociative symptoms be present, which precludes many high-risk people from being identified (
59). Third, there is much evidence that dissociative responses are common under conditions of high stress and may not necessarily be associated with psychopathology (
60,
61). It should be noted, however, that this argument may also be made in reference to arousal, which may be normal in many cases but does not predict later PTSD.
There are several possible mechanisms that may account for the mixed findings about peritraumatic dissociation and subsequent PTSD. First, dissociation may play a role in PTSD development in some individuals but not others. Diathesis stress models of dissociative disorders suggest that only people who possess dissociative tendencies respond to trauma with dissociative reactions (
62,
63). This notion is supported by evidence that higher levels of hypnotizability have been reported in people with ASD compared to those who have a comparable ASR, but lack dissociative symptoms (
64). Although both groups may have high risk for developing PTSD, only the subset of people who possess dissociative tendencies seem to respond with acute dissociative symptoms. Second, it is also possible that peritraumatic dissociation is associated with subsequent PTSD because it is associated with other known risk factors for PTSD development. For example, there is documented relationship between a history of childhood trauma and subsequent dissociation tendencies (
65). Moreover, childhood trauma is a known risk factor for adult PTSD (
66). It is possible that peritraumatic dissociation may be linked to PTSD because of its association with childhood trauma (
67). Third, another potential role of dissociation is its association with hyperarousal and extreme anxiety in the acute phase after trauma exposure. Peritraumatic dissociation may be a consequence of elevated arousal that occurs during trauma (
68). This interpretation is consistent with evidence that the relationship between peritraumatic dissociation and acute stress depends on levels of peritraumatic panic (
69,
70).
Another problem with the DSM-IV definition of dissociation was that it stated that dissociation in ASD could occur “either during or after experiencing the distressing event.” The ambiguity concerning the time frame for dissociation is problematic because transient dissociation (peritraumatic dissociation) and persistent dissociation can lead to contrary predictions concerning outcome. Cognitive models of trauma would predict that persistent dissociation would be maladaptive and would be associated with subsequent PTSD, because it impedes retrieval of emotional memories that are required for adaption (
71). In contrast, transient dissociation at the time of the trauma could be a normal response under stress, and even protective because it may limit the encoding of trauma of experiences. In this context, it is worth noting that persistent dissociation is more predictive of ASD (
72) and subsequent PTSD (
73) than dissociation that only occurs at the time of the traumatic experience. Similarly, a recent prospective study found that persistent dissociation was a stronger predictor of subsequent PTSD than dissociation occurring immediately after the trauma (
35). This pattern accords with evidence that much peritraumatic dissociation is transient. For example, one study found that the vast majority of trauma survivors who experienced dissociative reactions at the time of the trauma did not develop pathology, and their dissociative symptoms did not persist beyond the trauma (
74). However, the DSM-IV definition of ASD provides some protection against this problem by requiring that symptoms “last for a minimum of 2 days” (p. 472). There is some ambiguity about the transient and persistent nature of dissociation in ASD because whereas it does require a minimum of 2 days, it also states that dissociation may occur during or after the trauma. There seems to be inadequate specification of the exact dissociative symptoms described in ASD. Although studies of chronic samples have found that dissociative symptoms load onto distinct clusters (
75), this has not been found to be the case in recently trauma-exposed individuals. For example, one study of acute dissociative responses reported that 85% of individuals who reported lack of awareness of their surroundings also report derealization (
76). Furthermore, it seems repetitive to conclude that a traumatized individual suffers amnesia if that same individual did not adequately encode an event because of reduced awareness. However, although failure of encoding could result in amnesia, it is a different problem than retrieval difficulty, especially if amnesia is potentially reversible. Dissociation in the acute phase may function differently than more chronic dissociation. These issues suggest that the DSM-IV definition of dissociation may require greater delineation of dissociative symptoms to ensure that strongly overlapping con-structs are not being assessed multiple times. In this context, it is worth noting that a recent factor analysis of the Peritraumatic Dissociative Experiences Questionnaire (
68) found two distinct factors: Lack of Awareness and Derealization (
77). Whereas Lack of Awareness was not associated with ASRs, Derealization was. This pattern suggests that dissociative symptoms involving altered perceptions of self or one's surrounds may reflect more severe stress reactions than alterations in attention.
Taken together, these data suggest that dissociation does not warrant the central place in ASD that it has held. Nonetheless, it is clearly an important emotional response that many people do experience, and it can often be associated with severe reactions. The major problems with its prominence in ASD seems to be (a) mandating its presence in order to diagnose ASD, although as noted above, dissociative responses may be frequent in the acute aftermath of trauma, (b) using it to predict subsequent PTSD, which is a secondary and not a primary purpose of the disorder, (c) artificially distinguishing between overlapping dissociative responses, and (d) loosely combining dissociation occurring at the time of the trauma and in the following period. Future iterations of acute dissociative definitions need to more specifically operationalize the phenomena and specify the timeframe of the defined dissociative response. Despite these criticisms of current definitions of peritraumatic dissociation, the limitations of acute dissociation in predicting subsequent PTSD are also applicable to other ASD symptoms. As noted above, even when the dissociation cluster is not required, subsyndromal ASD is still only a modest predictor of PTSD. Nonetheless, the presence of dissociative symptoms in many trauma survivors suggests these reactions need to be considered among the constellation of acute stress responses.
ROLE OF SUBJECTIVE EMOTIONAL STRESSORS (A2) IN ASD
As with PTSD, in order to meet the Stressor (A) Criterion in the current definition of ASD, individuals exposed to threatening events (A
1) must also experience an intense subjective (A
2) reaction characterized as “fear, helplessness, or horror.” In DSM-IV, A
2 was included in ASD (and PTSD) to more specifically identify people who had a negative reaction to a traumatic event rather than simply survive the experience. The utility of the A
2 criterion has been challenged by a series of studies focusing on PTSD but have relevance to the role of A
2 in ASD. One study found that intense levels of acute postexposure fear, helplessness, and horror were weakly predictive of PTSD 6 months later (
87). Furthermore, other posttraumatic emotional reactions (such as anger or shame) also predicted PTSD. Finally, a small number of people who denied postexposure A
2 emotions also met PTSD criteria at 6 months. Another study reported that within a sample of A
1 exposed individuals who went on to meet PTSD B-F criteria, a substantial minority (23%) failed to receive a PTSD diagnosis because of the absence of A
2 (
88). Furthermore, there were no differences with regard to B-F symptom severity or impairment between the A
2 positive and A
2 negative cohorts examined among a community sample of 6,104 adults with a history of trauma exposure, and a substantial minority (24% males and 19% females) failed to meet criterion A
2 (
89). There is also evidence that only helplessness, but not fear or horror, is correlated with posttraumatic symptomatology (
90).
Supporting this accumulating evidence are reports that the presence of A
2 had no effect on PTSD prevalence in the DSM-IV Field Trials (
91) and in a sample of older male military veterans (
92). These results were replicated by Karam et al. (submitted, under review), regarding data from 102,846 respondents to the WHO World Mental Health Survey Initiative, who found that only 1.4% of respondents who met all other PTSD criteria failed to meet the A
2 criterion. Based on such findings, a number of investigators have called for the elimination of the A
2 criterion because of its poor positive predictive value, and it does not enhance identification of people who will develop PTSD. On the other hand, a consistent finding from three studies is the negative predictive value of A
2 (
87,
91,
92). In other words, people who do not exhibit an intense posttraumatic emotional reaction are unlikely to develop PTSD.
It has been suggested that the context for acute posttraumatic reactions should be expanded beyond the “fear, helplessness and horror” derived from a fear conditioning model of PTSD. For example, panic attacks have been one distinctive reaction that has received attention. In the DSM-IV Field Trials, the predominant indicator of posttraumatic distress was a panic reaction consisting of two components: “panic-physiological arousal” and “other panic symptoms” (such as trembling, shaking, tachycardia, and fear of dying), rather than A
2 symptoms (
91). This accords with proposals that the physical and cognitive symptoms of panic mediate dissociation, as well as (A
2) fear, helplessness, and horror. Other investigators have suggested that the focus should be on the positive predictive value of a fright reaction (
93) or peritraumatic autonomic activation (
94).
As noted earlier, a number of investigators (
95) have argued that other strong peritraumatic emotions are also associated with PTSD, such as sadness, grief, anger, guilt, shame, and disgust. The DSM-IV Field Trial observed that people could deny A
2 (fear, help-lessness, or horror), as well as a panic reaction but report confusion, negative affect, embarrassment, and disgust (
91). Such a wide spectrum of posttraumatic reactions calls into question the utility of limiting A
2 to the fear conditioning model. The DSM-IV does not consider other emotions, such as anger and rage, which are experienced during fight rather than flight responses, shame if an individual is made to endure degradation or guilt if there is a violation of one's moral beliefs or ethical standards (Resick and Miller, in press). Finally, military and emergency medical personnel (for example) often recall that they did not experience any acute A
2 or other emotional reaction in the immediate aftermath of trauma exposure. Rather, they report that their “training kicked in” as they carried out their responsibilities (
96,
97).
CROSS-CULTURAL CONSIDERATIONS FOR ASD
Whereas there is some evidence on cross-cultural manifestations of ASRs, there is very little cross-cultural work on the predictive power of ASD. Comparing prevalence across studies for ASD is difficult because (a) studies have used different assessment tools (ranging from validated measures to existing instruments for PTSD that have been amended to index ASD criteria but have not been validated), and (b) assessed patients from very different types of trauma. Generally speaking, most Western studies have focused on survivors of traumatic injury because these are convenient samples that can be located in hospitals; several studies from non-Western settings have measured reactions to war or massive natural disaster. These different contexts result in major confounds between culture and severity and type of traumatic experience. A further possible confound in comparing settings is the timeframe adopted by DSM-IV. ASD is defined as the satisfaction of the symptom criteria between 2 days and 4 weeks after the traumatic event. This definition implicitly presumes that the traumatic event has a discrete onset and offset, such as a motor vehicle accident or assault. In contrast, in the case of people responding to a massive natural disaster, civil conflict, or refugee relocation, these traumatic experiences can be experienced for months or years—in these cases it is problematic to compare prevalence rates in a setting where the traumatic event is discrete compared to ongoing. Highlighting the variability of ASD prevalence across trauma events is evidence that ASD has been identified variably following terrorist attacks after 9/11 (9%),(
98) motor vehicle accident (13–25%), (
59) and witnesses to drive-by shooting (33%) (
99). In terms of comparing prevalence, it is most useful to compare estimates across the same type of event. The most studied type of event is traumatic injury. In this context, prevalence does vary across settings. For example, prevalence of ASD following traumatic injury has been reported in populations in Australia (1, (
100) 6, (
101) 13, (
22) and 14% (
23)), United Kingdom (21 (
25) and 10% (
35)), Switzerland (4% (
102)), Germany (6% (
43)), and Japan (9% (
31)). These variable rates highlight that the prevalence rates do vary across settings, even when the trauma type is held constant, although there is inevitable variability across studies in stressor severity. Although most injury studies converge on prevalence rates between 6–10%, there are significant outliers (i.e., 1% in Australia and 4% in Switzerland, and up to 21% in the United Kingdom). This variability suggests that even among Western settings, the ASD prevalence varies.
In terms of prediction, across most studies there is convergence that whereas the majority of people who meet criteria for ASD subsequently develop PTSD, most people who develop PTSD do not initially meet criteria for ASD (
59). This pattern is reflected across cultures insofar as ASD has modest sensitivity in identifying people who will subsequently develop PTSD in Australia, the United Kingdom, the United States, Switzerland, Germany, Norway, and Japan.
The hallmark feature of ASD is dissociation. The role of dissociation is complicated in cross-cultural contexts because dissociative states have different connotations in different cultures. It is worth noting that general dissociation levels differ across racial groups; for example, African-Americans and Asian-Americans report higher rates of dissociation than white Americans (
103). Whereas DSM-IV presumes that peritraumatic dissociation is a maladaptive response that is a precursor to psychopathology, many different cultures perceive dissociative states in spiritual or religious frameworks that may be considered adaptive (
104). For example, the Candomblé religion in Brazil perceives dissociative states as part of a spiritual life history that needs to be narrated for self-healing (
105). Several studies have reported that depersonalization is reported more often in Western settings than Columbia (
106) and Peru (
107). It has been suggested that, whereas in individualistic societies (i.e., Western societies) having a detached view of oneself is regarded as aberrant, in collectivist societies it is common to view oneself in relation to one's surrounds. Although dissociative states can reflect maladaptive reactions across many cultures, it is premature to presume that dissociative states after trauma are indicative of poor adjustment in different cultures until appropriate studies are conducted. It should be noted that the same could be said of fear, anxiety, sadness, and other responses that can be appropriate and adaptive in some contexts and maladaptive in others.
From a cross-cultural perspective, there may also be problems in presuming a fear circuitry perspective with ASD that focuses on a narrow definition of the manifestation of anxiety. Some societies have reported acute reactions that extend beyond these responses. For example, a study in the collectivist society of Micronesia found that the majority of youth exposed to traumatic stress responded with
s'a'aw, which is a term that fuses anger with fear and reflects the negative emotional reaction to youth feeling that their standing in their local community was threatened (
108). Focusing specifically on fear in the sense of fear circuitry described could omit this ASR.
There is considerable evidence that ASRs are characterized by panic attacks (
109). Although there is not a significant body of evidence pertaining to panic in the acute phase after trauma, there is much evidence concerning the nature of panic attacks in different cultures. It is reasonable to conclude that these culturally specific features of panic attacks in different cultures will apply to posttraumatic panic in the acute phase. For example,
ataques de nervios have been documented in Dominican and Puerto Rican people, which has shown that although this constructs overlaps with panic, it is not identical (
110). Whereas
ataques de nervios shares features with panic attacks (fear of losing control, dizziness, fear of dying), there are other features not included in DSM-IV definitions of panic attacks (e.g., screaming, hitting out). Much work on
ataques de nervios has focused on the overlap with
ataques de nervios and panic disorder; however, the relevant issue for ASD is the breadth of description of acute reactions of panic attacks that does not limit it to strict panic disorder-type panic attacks. Similarly, there has been much work done on panic attacks in Cambodians (
khyâl), which involves a perception that a “wind”can enter the body in the diaphragm and rise through the body and cause a range of symptoms, including shortness of breath, tinnitus, dizziness, soreness in the neck, and catastrophic fears for ones well-being (
111,
112). Rather than specify the exact nature of the panic symptoms associated with Cambodian reactions, it is sufficient to note that culturally specific descriptions of panic should be applied to ASD because panic attacks (as distinct from panic disorder) are common in the acute phase after trauma.
ASD currently requires marked avoidance to satisfy criteria. This has conceptual overlap with emotional numbing, which is described as one of the dissociative symptoms. It is important to note that certain Asian cultures explicitly discourage emotional displays because it may lead to adverse consequences. For example, people from Bali may adopt a “smooth” facade following trauma to mask emotional distress; this is adopted to avoid personal illness, harm to others, and harm to the spirits of lost loved ones (
113). Similarly, the Toraja in Indonesia avoid strong emotions which is commonly regarded as adaptive, because intense emotions are considered to be linked to poor health outcomes (
114). To presume that all forms of avoidance are markers of impaired emotional processing and are maladaptive may ignore important local cultural standards of coping. At this point, there is insufficient data to inform us about the extent to which different forms of avoidance are adaptive or maladptive across cultural settings.
Timeframe for ASD
In DSM-IV, ASD could be diagnosed between 2 days and 4 weeks following the traumatic event. There was no sound evidence for the minimum 2-day delay between the onset of the traumatic event and the symptoms. There is concern that diagnosing people within 48 hr of an event may identify many trauma survivors who are experiencing transient stress reactions that will subsequently abate in the following days. In terms of the timeframe, the available evidence points to extending the current minimum delay from 2 days to a longer timeframe, to reduce the likelihood of false positive diagnoses; that is, by classifying people as satisfying ASD who may no longer display these symptoms 1 or 2 days later. There is a need to find a balance between introducing the diagnosis too early, yet ensuring that highly distressed people can receive diagnosis and treatment as soon as they need it. There is very little evidence to guide DSM-5 regarding the optimal timeframe, because this decision is largely influenced by situationally specific factors and by the posttrauma environment. It is highly probable that ASD reactions will be higher when current threat is still present relative to when the threat has passed. For example, one study reported PTSD prevalence of 99% in Sierra Leone; however, this study was conducted in the context of active civil unrest and direct threat to respondents (
115). It would be useful to study datasets that have assessed ASRs at different timeframes within the initial weeks following trauma exposure, because this can shed light on the trajectory of acute symptoms over the initial weeks, which would provide some guidance on the optimal number of symptoms required to identify people who are likely to be suffering acute symptoms beyond the immediate period.
Distinction between normal and pathological stress reactions
One of the major challenges for a diagnosis of ASD is to operationally distinguish between normal and pathological stress responses to a traumatic event. As noted above, acute posttraumatic stress reactions are very common and the majority of these subside within a short timeframe. If the new aim of ASD is to identify severe ASRs, how does one quantify severe or pathological stress reactions? It is important to note that the underpinning rationale of this proposed diagnosis is not to predict longer term disorder, but to facilitate treatment for those suffering significant distress and whose response suggests that this distress may be interfering sufficiently or distressing the person excessively such that treatment may facilitate recovery. In this sense, it may be more appropriate to describe the ASD construct in terms of severity of ASR rather than “psychopathology.” Several criteria may be considered in operationalizing the distinction between severe and less severe reactions. Is a requisite number of acute symptoms associated with impairment of functioning, as described in most DSM disorders? This is a problematic criterion to apply to ASD because it is often difficult to measure functioning in the weeks after trauma, because social disruptions, environmental upheaval, or changing medical status may limit scope for measuring functioning accurately. Another possibility is to define the required number of symptoms in order to identify a limited proportion of individuals. It would be erroneous to define ASD in a liberal fashion such that the majority of trauma survivors met criteria, because it is well documented that the majority of trauma survivors, even in the acute phase, adapt in the weeks from the severe levels of distress that may be initially experienced. Ultimately, the number of symptoms that should be required to meet an ASD diagnosis needs to be empirically determined to ensure that (a) only the minority of trauma survivors are captured by the diagnosis, and (b) the symptoms are likely to describe marked stress responses that will be assisted by targeted intervention.
Utility of an ASD diagnosis
In considering the utility for the ASD diagnosis, it is important to consider the conceptual, empirical, and practical bases for such a diagnostic category. In terms of conceptual issues, the ASD diagnosis has been criticized because the major distinguishing factor ASD and PTSD is the duration of symptoms (
4,
5). One rationale for retaining the ASD diagnosis is to formally describe the severe posttraumatic stress that some people experience in the initial month after trauma exposure without labeling them as suffering PTSD. There has justifiably been a reluctance to describe severe stress reactions as PTSD because many cases in the acute phase will be transient. The issue that has to be resolved is the manner in which these reactions are described. Distinguishing syndromes according to a timeframe can be justified by acknowledging that different assumptions underlie this distinction: whereas PTSD is presumed to be a disorder that persists beyond a timeframe when the majority of people will experience remission of severe reactions, (
6,
7) ASD is recognized as a potentially transient disorder that may or may not develop into PTSD. Although the argument could be made that PTSD could include an “acute” subtype or specifier, this could artificially elevate the prevalence rates of PTSD.
The question may be asked: why do we need the ASD diagnosis? If the predictive role of ASD is abandoned, what is the need to describe severe acute reactions? A major rationale for the inclusion of ASD is to provide health care rebates for US citizens. At a service delivery level, this has been identified as important in order for many people, who suffer distress in the acute phase after a trauma, to receive a formal diagnosis that will allow them to receive compensable health care services for mental health problems. The timeframe of 1 month before PTSD may preclude some survivors from receiving diagnosis and health-care. In this context, we need to acknowledge that DSM-5 is not driven simply by theoretical or scientific priorities but also by practical issues faced by US practitioners. In this sense, DSM-5 is primarily a US product that at times may have less relevance to international communities that may not share the same health care financing problems as the United States. A cogent argument could be made that if there was no need for a diagnosis to facilitate access to appropriate mental health services in the United States, the need for the ASD diagnosis would markedly diminish. Nonetheless, the expectation is that the proposed definition of ASD will provide clinicians anywhere to identify the more severely distressed survivors of trauma who may benefit from early interventions that have proven efficacy with ASD patients.
Literature-informed recommendations
1.
There is strong evidence that ASD does not identify the majority of people who subsequently develop PTSD, in that it is sensitive but not specific. Accordingly, the definition of the diagnosis should not necessarily be shaped by factors that are predictive of PTSD. Current studies indicate that variations of the ASD diagnosis do not adequately address the poor predictive capacity of ASD. Accordingly, it is useful to distinguish between the goals of describing acute reactions from predicting people who will develop chronic disorder. In light of the reviewed evidence that ASD does not adequately identify the majority of people who subsequently develop PTSD, it is proposed that it's predictive role be abandoned. To that end, it is more appropriate to conceptualize the ASD diagnosis as a means to describe ASRs that are severe enough to warrant clinical attention. In many health systems (especially in the United States), receiving a diagnosis can facilitate access to mental health services, and so the ASD diagnosis may allow people in need of mental health services to receive adequate care. In this sense, ASD may be conceptualized as severe distress in the acute phase but without the presumption that it will develop into subsequent disorder. This can actually be conceptualized as a benefit of this diagnostic category.
2.
An outstanding issue is the extent to which ASD should focus on fear/anxiety/posttraumatic stress responses or should be broadened (in a manner similar to ASR) to encompass the range of emotional problems trauma survivors can experience in the acute phase. The attraction of the latter option is that it will be applicable to most people who suffer anxiety, depression, grief, guilt, anger, or somatic reactions. The problem with this option is that it does not necessarily translate to specific treatment options, which the current ASD formula does. A parsimonious solution seems to describe people in the acute phase who present with predominant posttraumatic stress responses as ASD (and who will then receive targeted intervention), and Adjustment Disorder can be applied to other trauma survivors who display other forms of distress.
3.
If the goal is to describe acute anxiety reactions following trauma, the remaining question is to define the requisite symptoms. At present, the ASD criteria are clustered into four categories (dissociation, re-experiencing, avoidance, and arousal), and one needs to display reactions in each category to meet criteria. The current data suggest that there is considerable heterogeneity in acute responses and being prescriptive about the specific symptoms may be difficult and exclude those who report anxiety-related distress in different forms. In this sense, it needs to be recognized that, whereas chronic forms of PTSD symptoms do tend to cluster into recognized groupings of symptoms, this may develop as time progresses. Accordingly, it may be more appropriate to describe ASD in terms of people suffering a requisite number of symptoms, but not prescribing that they need to be from specific clusters. For example, current data indicate that many patients respond in the acute phase with dissociative responses, but comparable numbers display acute stress in the absence of dissociation. Requiring a requisite number of symptoms may increase identification of acute distressed people who may benefit from treatment by acknowledging the diversity of acute posttraumatic stress responses.
4.
The remaining question is what potential symptoms should comprise the ASD diagnosis and how many of these should be required to meet diagnostic threshold. Across studies, there is convergent evidence that re-experiencing symptoms are a hallmark feature of anxiety responses in the initial period after trauma. This observation is consistent with fear conditioning models of trauma response, (
116) and accords with the finding that the absence of these symptoms in the acute phase is highly predictive of the absence of acute or chronic anxiety (
58). Reviewing the literature, however, indicates that re-experiencing needs to be defined somewhat broadly because it does not always involve repeated intrusive memories. Re-experiencing following the trauma may include memories, nightmares, flashbacks, or psychological, somatic, or behavioral reactivity to reminders. This is ultimately an empirical question that requires calculating the requisite symptoms reported by patients in the acute phase to capture those patients who also display marked distress on independent measures. There is a need to limit overdiagnosis, insofar as it would be a mistake to describe all stress reactions in the acute phase as ASD when they may be short-term transient responses that may not require mental health intervention. In this context, it is worth emphasizing that the ASD diagnosis in DSM-V may be conceptualized as an acute response that may be temporary and resolve rapidly
or may continue to PTSD. Unlike many other disorders, ASD is not likely to be tested in the context of field trials because it requires identifying people who have very recently been exposed to traumatic events. On the other hand, there are many datasets in the field in which researchers have assessed ASD symptoms. A potential means to clarify the optimal number of symptoms would be to calculate the requisite number of symptoms that patients report in the acute phase that optimally captures those patients who are reporting significant distress (as measured by independent measures of posttraumatic stress/anxiety).
5.
In terms of timeframe, it will be important in text to highlight that clinicians need to evaluate the extent of the disorder in relation to which the threat has passed or if the person is still living in a highly stressful environment (e.g., soldier in combat or survivor of massive disaster). At this point in time, it may be appropriate to extend the delay from 2 to 3 days to not only minimize overdiagnosis, but also to ensure that distressed people are able to be assessed and treated in the acute phase.
Proposed ASD diagnostic criteria for DSM-V
The rationale for the proposed diagnostic criteria is to identify trauma survivors in the initial month following trauma who are displaying marked fear/anxiety responses and may benefit from mental health services. The focus of the diagnosis is on acute posttraumatic stress, because the disorder is conceptualized as a diagnosis of early PTSD and because there is a strong evidence base for intervening in cases that are characterized by fear/anxiety (rather than more diverse emotional responses that can be described by Adjustment Disorder).
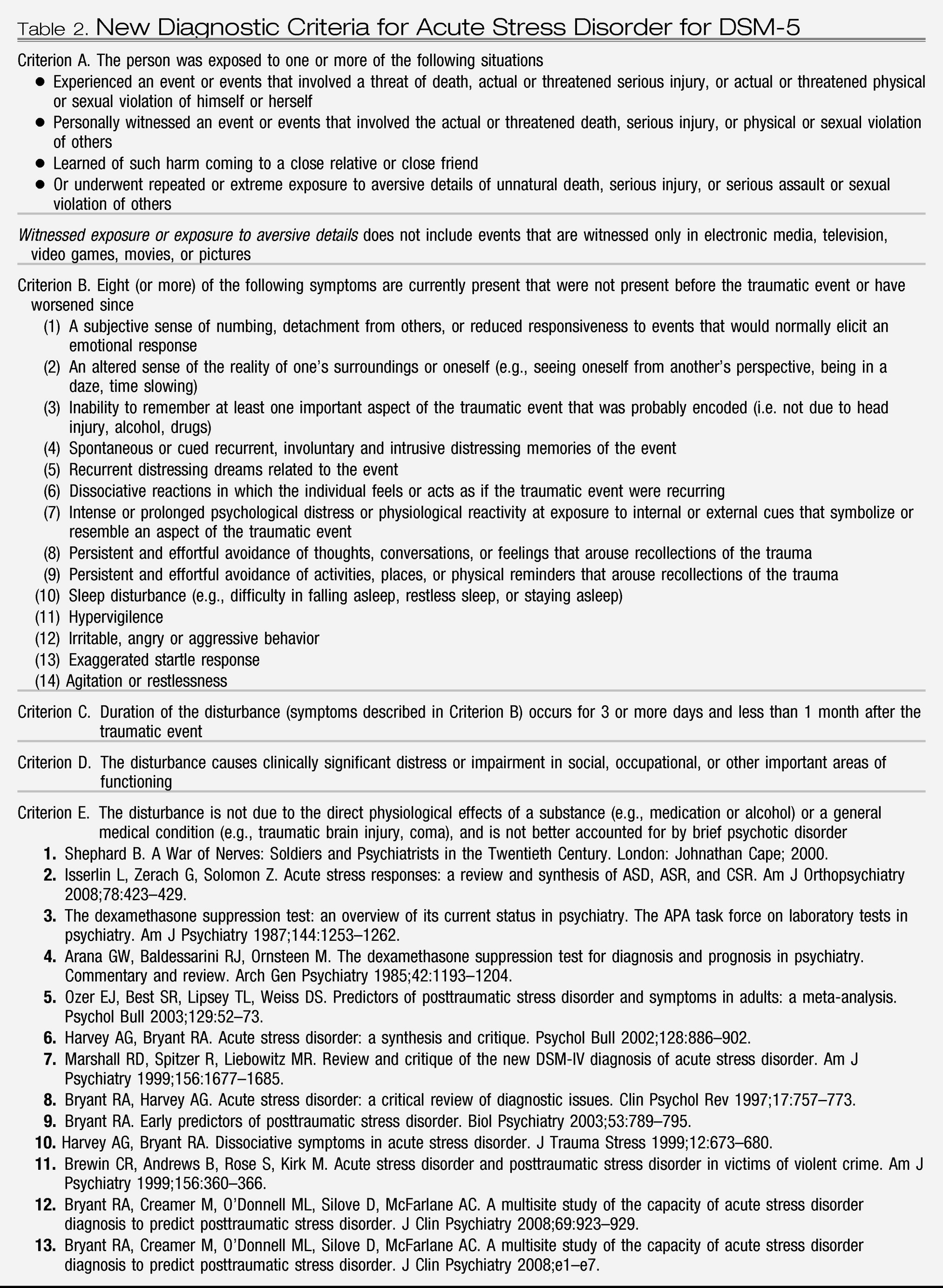
This revision is a radical shift from the DSM-IV definition. This shift is justified by that (a) the ASD diagnosis was new to DSM-IV and at the time there was very little evidence to substantiate the defining symptoms, (b) there is now strong evidence that ASD is not the optimal means to identify trauma survivors who are high risk for PTSD, and (c) ASD is better conceptualized as a description of severe ASRs. The proposed revision will comprise the major changes to the DSM-IV definition of ASD: (a) modifying the Stressor definition to eliminate A
2, and (b) requiring a minimum number of symptoms to present, but these do not need to be from prescribed clusters. The specific proposal is:
1.
Criterion A1 (stressor) will probably not change substantially. The language of A1 has been revised to emphasize that qualifying events must involve direct exposure to actual or threatened death, serious injury, or a threat to the physical integrity of others. The most controversial aspect of the DSM-IV A1 Criterion is having been “confronted by” traumatic events. The proposed revision limits such “confrontation” to learning about the traumatic exposure of a close friend or loved one or learning about aversive details of unnatural deaths, serious injury or serious assault to others. This includes learning about the homicide of a family member, learning about the gruesome death or grotesque details of rape, genocide, or other abusive violence to others.
2.
Criterion A2 (subjective sense of fear, helplessness, or horror) will be eliminated because there is little evidence to support it.
3.
B1 (sense of numbing) is largely unchanged but moved to B5.
4.
B2 (reduction in awareness) is deleted because earlier studies indicate that it overlaps largely with other dissociative symptoms.
5.
B3 (derealization) and B4 (depersonalization) are combined into B6 because of evidence that depersonalization and derealization are strongly overlapping.
6.
B5 (dissociative amnesia) is largely unchanged and becomes B7.
7.
The re-experiencing symptoms (previously Cluster C) are now delineated as specific symptoms in accordance with considerable evidence concerning ASRs. These symptoms are intrusive memories (B1), nightmares (B2), flashbacks (B3), and psychological distress/physiological reactivity on reminders (B4).
8.
The avoidance symptoms (previously Cluster D) are now delineated as two separate symptoms: avoidance of thoughts, feelings, and conversations (B8) and avoidance of situations (B9). This will refine the earlier description of “marked” avoidance.
9.
The arousal symptoms (previously Cluster E) are now delineated as five separate symptoms to refine the earlier description of “marked” arousal: sleep disturbance (B10), hypervigilence (B11), irritability (B12), startle reaction (B13), and agitation (B14).
10.
The major revision is that rather than requiring endorsement of each of the four clusters, the new criteria recognize that there is heterogeneity in acute stress responses, and thus it requires a specific number of symptoms without requiring any particular symptoms to be present. At this stage, the evidence indicates that requiring people to satisfy specific clusters may not be appropriate in the acute phase because current evidence that satisfying the four ASD clusters is restrictive of people satisfying acute stress (
4,
7). It is premature to definitively conclude that there should not be a requirement that specific symptoms/clusters be present in order to satisfy ASD diagnosis because the available datasets have not been exhaustively studied. There is a theoretical reason that re-experiencing may be mandatory because fear conditioning models posit that these symptoms will drive all other reactions; however, this has yet to be empirically validated across datasets.
The proposal described here is tentative and is dependent on comprehensive analyses of at least 12 existing datasets that have collected ASD responses from numerous countries (including datasets from the United Kingdom, the United States, Israel, Japan, The Netherlands, Norway, and Australia). The eventual criteria need to be empirically validated across these datasets to ensure that the structure and number of symptoms is consistent across settings and accurately identifies the minority of people with severe stress reactions that would indicate early intervention.
At this point, it is tentatively proposed that 8 out of the 14 symptoms be present to make an ASD diagnosis. The tentative proposal of 8 from 14 symptoms was derived from two steps. The 14 potential symptoms were derived from the current list of ASD symptoms, with the combination of several symptoms that have been shown in earlier studies to be strongly over-lapping; for example, reduced awareness was deleted because of strong overlap with other symptoms, and derealization was combined with depersonalization because of the theoretical and documented overlap between these symptoms (
8). Three large-scale datasets (one unpublished dataset from Israel and two published datasets from the United Kingdom (
9) and Australia (
10,
11)) were analyzed to determine an optimal cut-off to identify 20% of recently trauma-exposed people. We emphasize that this decision-rule was adopted only to calculate an approximate number of symptoms that could be tested (and modified) in more comprehensive analyses of more datasets. On this basis, it was noted that 8 of the potential 14 symptoms tended to capture approximately 20% of the samples. Accordingly, we propose that this requisite number of symptoms should be tested across datasets.