Physical or sexual traumatization during childhood has been associated with development of multiple personality disorder,
1 refractory psychosis,
2 borderline personality disorder,
3,4 somatoform disorder,
5 and panic disorder.
6 Childhood physical abuse may also sensitize patients to the development of posttraumatic stress disorder (PTSD) in adulthood.
7 Researchers have long believed, on the basis of animal studies, that early deprivation or abuse may result in neurobiological abnormalities.
8–10 However, there has been little evidence for this in humans.
11 Green et al.
12 suggested that many abused children show evidence of neurological damage even in the absence of apparent or reported head injury. They found that soft neurological signs and nonspecific EEG abnormalities were more common in abused children and considered this to be an additional source of trauma—amplifying the pathological impact of the abusive environment.
13 Childhood incest has been associated with abnormal EEG activity. Davies
14 reported that in a sample of 22 patients involved as children or as the younger members of an incestuous relationship, 77% had abnormal EEGs and 36% had clinical seizures. Davies suggested that these children were at greater risk for sexual abuse by family members because of their neurological handicap.
More recently, Teicher and colleagues
10,15–19 hypothesized that early traumatic experience, in the form of childhood abuse, could affect the development of the cerebral cortex and limbic system. They first tested this hypothesis by using a self-report questionnaire, the Limbic System Checklist-33 (LSCL-33), to ascertain whether there was an association between early abuse and symptoms suggestive of temporal lobe epilepsy in 253 adult outpatients.
15 Abuse history had a prominent effect on scores. Physical abuse was associated with a 38% increase, sexual abuse with a 49% increase, and combined abuse with a 113% increase. Physical or sexual abuse was associated with elevated LSCL-33 scores only if the abuse occurred before age 18.
In another study, a chart review was conducted to examine blindly the association between abuse history and neurological abnormalities in 115 consecutive patients admitted to a child and adolescent psychiatric inpatient unit.
18 Abused children had a greater incidence of electrophysiological abnormalities compared with nonabused patients (54.4% vs. 26.9%,
P=0.021). Interestingly, abused and nonabused patients differed only in the prevalence of left hemisphere abnormalities. The results of neuropsychological testing indicated that left hemisphere deficits were 6.7-fold more prevalent than right hemisphere deficits in the abused group; this ratio was 3-fold less in the nonabused group. Schiffer et al.
19 used probe auditory evoked potentials as an indirect, noninvasive measure of auditory cortex activity. They compared 10 unmedicated adults with no currently active psychopathology who grew up in psychologically abusive families with 10 intact control subjects from nonabusive families. Probe evoked potentials were measured while subjects focused on a neutral work-related memory or a distressing childhood memory. In comparison to intact control subjects, adults from psychologically abusive families had highly lateralized evoked potential patterns. During the neutral memory task, evoked potentials were strongly suppressed over the left cortex in the abused group (indicative of enhanced left cortex cognitive activity), and this pattern switched to right cortical suppression during recall of the distressing memory. Control subjects showed no significant degree of laterality or switch between these two tasks, even though they had equally strong emotional reactions. These findings suggest that the two hemispheres may function more autonomously in patients with childhood abuse.
The goal of the present study was to ascertain whether early childhood trauma was associated with alterations in the pattern or degree of cortical development. Teicher et al.
17 previously theorized that abuse may affect cortical development by activating monoamine transmitters that exert trophic effects; by enhancing stress hormones that can affect cell migration, glial mitosis, and myelination;
20,21 and by affecting the flow of information between the right and left hemispheres.
Quantitative analysis of EEG coherence can provide important noninvasive measures of brain development. Briefly, EEG coherence is a parameter that indicates the degree of synchrony (“shared activity” or interconnectivity) between two EEG leads across a portion of the bandwidth. Thatcher and colleagues
22,23 proposed that EEG coherence is determined by two primary compartments. The first compartment represents the local effect of short axonal connections of neighboring pyramidal cells; the second compartment represents long axonal propagation via intracortical association pathways. These two compartments have opposite effects on coherence. Local cortical connections process and alter the temporal properties of the EEG signal, so coherence decreases with differentiation. In contrast, long axon pathways propagate the signal without distortion. Thus, coherence increases with myelination and development of association pathways.
Many studies have shown that coherence measures can provide useful information about brain development. EEG coherence has been fruitfully applied to the study of normal development, mental retardation, and learning disorders.
24,25 Coherence measures have also been reported to be particularly useful, and more powerful than spectral EEG measures, in discerning differences between control subjects and patients with schizophrenia.
26–31 EEG coherence measures appear well suited for detecting the relatively subtle structural brain abnormalities that presumably occur in schizophrenia, and coherence is less susceptible to medication effects than spectral EEG.
26,27 EEG coherence changes throughout childhood and adolescence, in concert with Piaget's stages of intellectual development.
24 Thus, measurement of EEG coherence is a suitable technique to test the hypothesis that early childhood abuse affects cortical maturation and laterality.
METHODS
Subjects
Fifteen child or adolescent inpatients (mean age±SD=10.7±2.5 years, male:female=7:8, 10 medicated) with a history of intense physical or sexual abuse, confirmed by the Massachusetts Department of Social Services (DSS), were recruited. Briefly, intense sexual abuse was defined as penetration or fondling by an adult or significantly older individual, accompanied by force, coercion, or distress. Physical abuse was defined as blows, beatings, burns, whipping, and other forms of violence, with the exception of spankings administered in context of what could be considered appropriate discipline. Further, there had to be a persistent pattern of abuse sufficiently severe to be substantiated by DSS investigation. These investigations often led to removal of the child from the home or criminal prosecution of the abuser. Subjects were excluded if there was any known history of physical abuse to the head or other form of head trauma.
The control subjects were 15 healthy volunteers (mean age 10.1±3.1 years, M:F=6:9), assessed by clinical interview and the Child Behavior Checklist.
32,33 The two groups did not differ significantly in age (
F=0.34, df=1,28,
P>0.5), or gender (
F=0.13, df=1,28,
P>0.7). All subjects were between 6 and 15 years of age, were right-handed, and had no history of neurological disorders or abnormal intelligence, except 3 patients with borderline IQ scores between 73 and 78. No subject had a learning disorder diagnosis. Diagnostic data were derived by consensus based on discharge diagnosis (DSM-III-R,
n=15) and structured clinical interviews (either the Diagnostic Interview Schedule for Children–Current Episode [DISC-C;
n=8] or the Schedule for Affective Disorders and Schizophrenia for School-Age Children, epidemiologic version [K-SADS-E;
n=2]). The 10 children who received medication were predominantly treated with antidepressants (3 on fluoxetine, 1 on desipramine, 1 on nortriptyline, and 1 on trazodone), stimulants (3 on methylphenidate, 1 on
d-amphetamine), or mood stabilizers (2 on valproate, 1 on lithium). One child received haloperidol. Informed consent was obtained from parents or guardians, and informed assent was obtained from the child.
Apparatus and Procedures
Subjects were seated comfortably in a reclining chair in a sound-attenuated, semidarkened room. EEG measures (QSI-9000; Ontario, Canada) were obtained from 19 gold electrodes of the International 10–20 System
34 digitally referenced to linked ear lobes. Eye movements were detected using a bipolar vertical EOG lead. A single forehead electrode served as ground. Electrode resistances were below 5 kΩ. Typical amplification was 80 or 40 K, with bandpass filters set at 0.5–30 Hz. Sampling time was 9.77 ms. Subjects were instructed to minimize movement and to be alert during the tests. At least 8 minutes of eyes-closed resting EEG were recorded. Results were carefully examined to eliminate epochs with eye movement or muscle artifact. A total of about 40 seconds (16 epochs) of artifact-free recording were selected for analysis. In almost all instances data were derived from the early part of the recording period, but in some cases data from the middle of the recording period were used if the subject was less drowsy during this time. Although 4 patients had diffuse slow-wave bursts or sporadic focal spikes, records selected for analysis contained no paroxysmal discharges.
Data Analysis
Fast Fourier transforms (FFTs) were performed to calculate absolute power in eight non-midline channels per hemisphere. Intrahemispheric coherence measures were computed for the alpha (8–13.6 Hz) frequency band as described by Thatcher et al.
22 Measures of EEG coherence between all combinations of the eight lateralized leads per hemisphere (28 measurements) were averaged to provide a composite hemisphere measure (
Figure 1A). These measures were log transformed (log[
X]/[100−
X]) to obtain Gaussian distributions for statistical analysis.
22,35 Although common reference coherence has been used in nearly all published EEG coherence studies, Fein et al.
36 suggested that large differences in phase or power could produce erroneous measures. Thus, asymmetries in hemispheric coherence were also assessed by using a bipolar montage that is not susceptible to these artifacts.
36 Bipolar coherence measures were computed between the eight adjacent electrode pairs along the anterior–posterior axis and the eight adjacent electrode pairs around the periphery (
Figure 1B). Seven independent coherence measures were calculated per hemisphere based on these bipolar derivations, which were averaged to obtain composite hemisphere measures and were log transformed for statistical analysis (
Figure 1B). Lateralized differences were assessed by calculating a laterality index on the nontransformed composite data. The laterality index was defined as 100×([L−R]/[Average (L+R)]).
A major statistical problem in the analysis of EEG coherence data is that there are literally thousands of possible statistical comparisons that can be made. To avoid potential problems with multiple comparisons, we aggregated the data into composite hemisphere measures, and only discrete prespecified hypotheses were tested. Three primary questions were addressed. The first was whether there was any evidence for asymmetric cortical development. This was tested by ascertaining whether there was a difference between abused patients and control subjects in the average level of right versus left hemisphere alpha coherence. If there was evidence of asymmetries, then the next question was whether these asymmetries could be localized to particular regions. The method of Besthorn et al.
37 was used to calculate average short-distance coherence for each lead. As illustrated in
Figure 1C, the numbers of measures averaged for each lead varied with location. The third question, given evidence for an overall asymmetry in EEG coherence, was whether the asymmetry was a consequence of abnormalities in myelination or cortical differentiation. This was assessed by calculating the rate of decay of alpha EEG coherence over intraelectrode unit distance. Thatcher et al.
22 proposed that the rate of decline in coherence over distance reflected the ratio of short axon fibers to long axon fibers, and that a rapid rate of decline was associated with a greater degree of cortical differentiation. To calculate the rate of decay, all common reference intrahemispheric coherence measures were grouped into three levels of distance, based on unit distance within the 10–20 System grid (
Figure 1D).
I unit distance consisted of the 15 adjacent electrode pairs per hemisphere,
II unit distance consisted of 8 electrode pairs separated by one intervening electrode, and
III unit distance consisted of 4 pairs separated by two intervening electrodes. Rate of decay was calculated for each subject by using a power decay function (
y=
Ax−
b), where
b is the decay slope.
Statistical Analysis
Statistical differences between patients and control subjects were calculated by using analysis of variance (SYSTAT, Evanston, IL). Although the groups did not differ significantly in either age or gender distribution, it is known that age
24 and gender
38 can influence coherence values. Thus, regression measures were used to ascertain if these intervening variables were exerting a significant effect; if they were, gender was used as a factor, and age as a covariate, to ascertain whether group differences persisted after additional statistical control for these variables. Left–right lateralized differences within each group were assessed by using two-tailed Student's
t-tests to accept or reject the null hypothesis that the laterality index was equal to zero.
RESULTS
Intrahemispheric Coherence
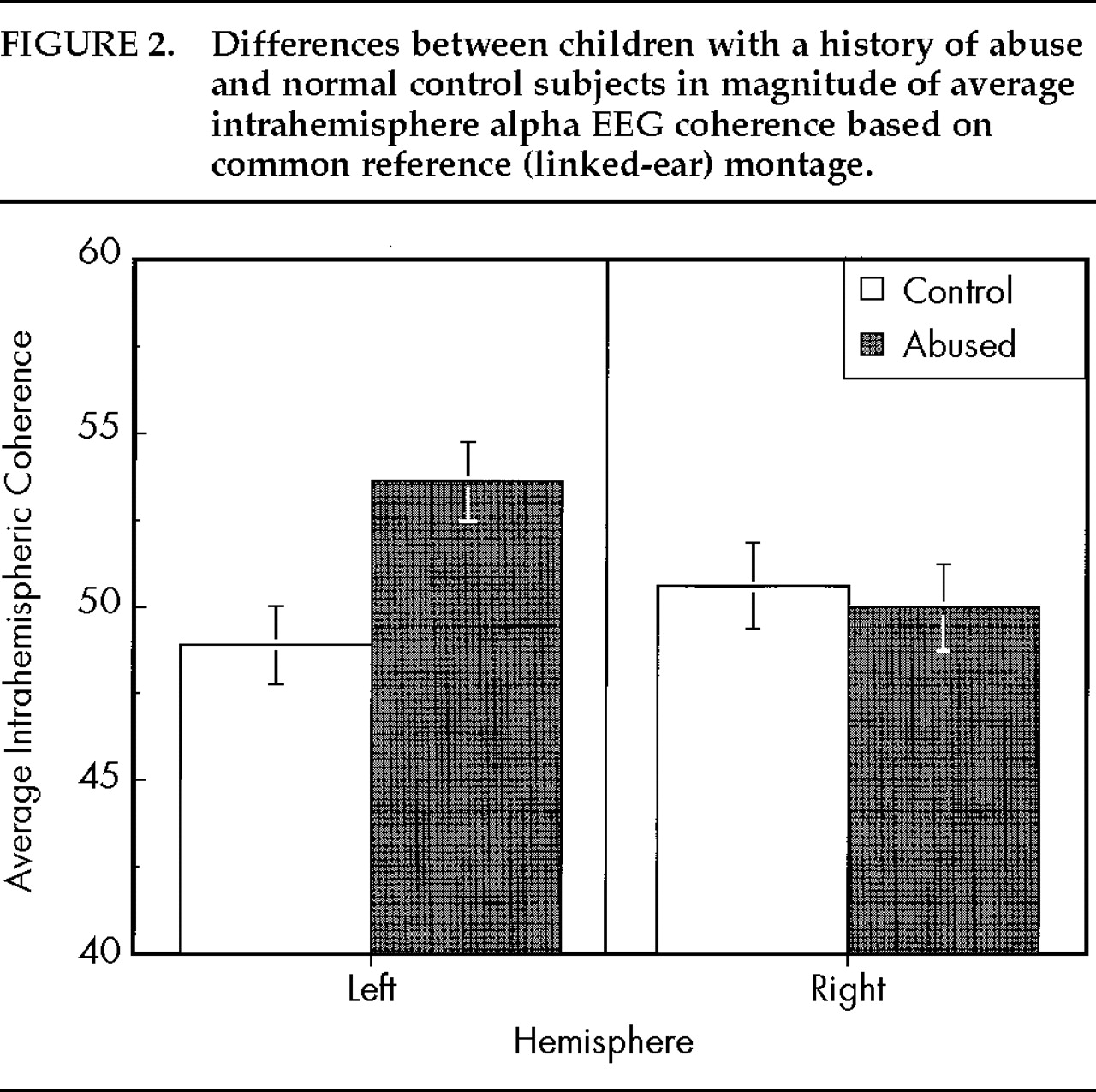
The first question was whether there were significant group differences in overall left hemisphere versus right hemisphere coherence. As illustrated in
Figure 2, there was a significant interaction between hemisphere and group (
F=7.76, df=1,27,
P<0.01), which was influenced by age (
F=8.39, df=1,27,
P=0.007) but not by gender (
F=1.45, df=1,26,
P>0.2). Abused children had greater average left hemisphere coherence than normal children (
F=8.56, df=1,27,
P=0.007) but a comparable degree of right hemisphere coherence (
F=0.11, df=1,27,
P>0.7). In control subjects, the average age-covaried, within-subject laterality index was –3.21% (
t=1.19, df=14,
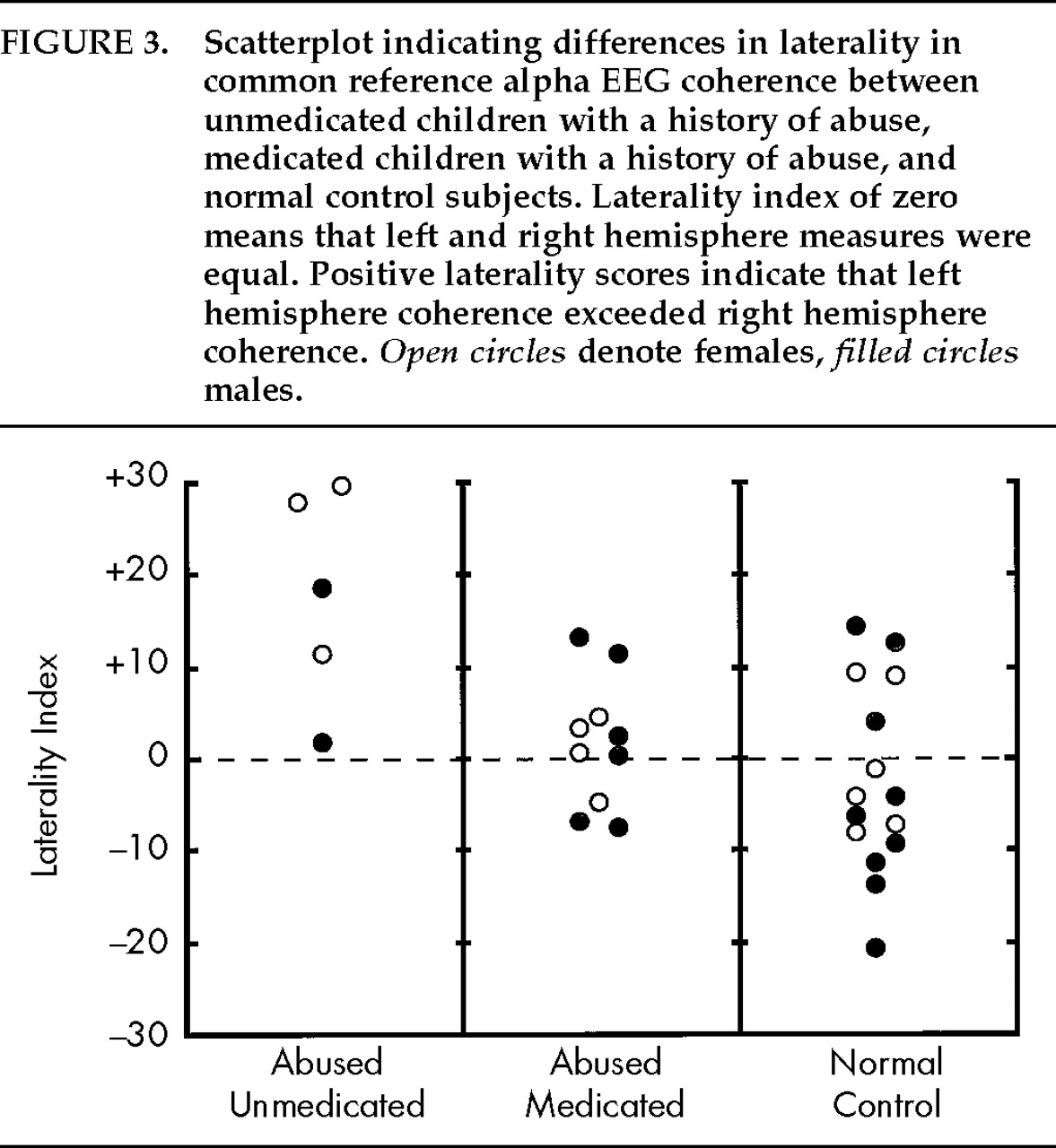
P>0.20), indicating a nonsignificantly lower level of left hemisphere versus right hemisphere coherence. In contrast, abused children had an average laterality index of +7.21% (
t=2.67, df=14,
P<0.02), indicating significantly greater left versus right coherence. The prominent difference between groups in the degree and direction of the laterality index is indicative of a reversed cerebral asymmetry (
F=7.41, df=1,27,
P=0.01). Within the abused group, medication use appeared to have a prominent effect on the degree of asymmetry (
F=11.47, df=1,12,
P=0.005;
Figure 3). Unmedicated abused patients had a much greater (and more abnormal) laterality index than abused patients receiving pharmacotherapy (unmedicated: +17.7%; medicated: +1.4%).
There was no apparent relationship between degree of asymmetry and diagnosis. Abused children meeting DSM-III-R criteria for major depression on either discharge or structured interview (n=6) had about the same laterality index as abused children who did not meet criteria (+6.0±4.9 vs. +7.3±4.0; F=0.04, df=1,13, not significant). There were also no asymmetry differences between abused children who did (n=6) and did not meet criteria for PTSD (+9.2±4.8 vs. +5.2±3.9; F=0.53, df=1,13, not significant), or who met (n=7) or did not meet criteria for conduct or oppositional defiant disorder (+10.2±4.3 vs. +3.9±4.1; F=1.12, df=1,13, P>0.3).
Differences between abused and nonabused subjects were also not an artifact of inclusion of the 3 patients with low IQ. Reanalysis excluding these 3 subjects resulted in comparable if not greater statistical differences between groups (left hemisphere coherence: F=11.02, df=1,24, P=0.003).
The association between abuse and EEG coherence also emerged in a subgroup of 7 children subjected only to sexual abuse without any concomitant physical abuse. Age-covaried L–R laterality index was +10.9 in the abused children and –3.6 in control subjects (F=12.48, df=1,19, P=0.002). This finding lends support to the notion that the coherence abnormalities are not a consequence of direct physical injury.
Differences in intrahemispheric coherence were confirmed by using bipolar montage analysis, which yielded a lower estimate of coherence but comparable group differences. There was a significant group by hemisphere interaction (F=6.33, df=1,26, P=0.02), which was not significantly influenced by age (F=1.63, df=1,25, P>0.2). Children with a history of abuse had an average laterality index of +4.5% (L>R), whereas normal control subjects had a laterality index of –7.2% (R>L), indicative of a significantly reversed asymmetry (F=5.97, df=1,26, P=0.02). Overall, abused children had significantly higher measures of left hemisphere coherence than control subjects (F=4.29, df=1,26, P<0.05) but did not differ in measures of right hemisphere coherence (F=1.25, df=1,26, P>0.2). With the bipolar measure, there were no discernible effects of medication use in the abused group (F=0.01, df=1,11, P>0.9), and the degree of left/right hemisphere asymmetry was nearly identical in medicated and unmedicated abused subjects (Laterality Index: abused-unmedicated +4.7%; abused-medicated +4.1%). Thus, both common reference and bipolar EEG coherence procedures revealed significant differences between abused children and control subjects in their overall degree of left hemisphere coherence.
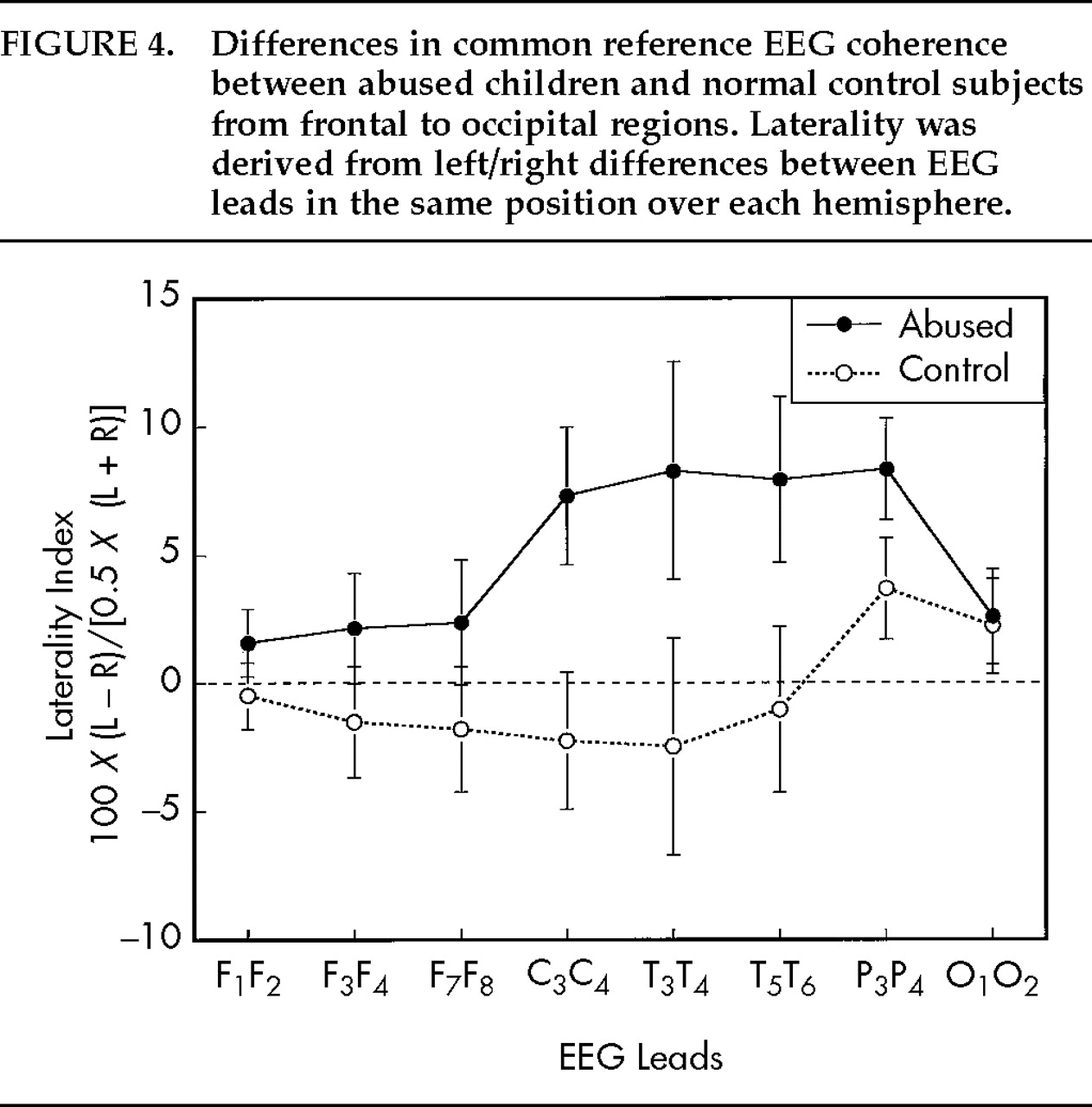
Regional Coherence Asymmetries
Neighboring electrode pairs were averaged in order to ascertain the most significant regions of common reference alpha hemispheric asymmetry. In abused subjects, significant left>right asymmetries (based on log-transformed values) were observed in central (C
3–C
4;
F=4.96, df=1,14,
P<0.05), posterior temporal (T
5–T
6;
F=6.84,
P<0.02). and parietal regions (P
3–P
4;
F=17.60,
P<0.001). No significant regional asymmetry was found in normal subjects (
Figure 4). Abused subjects differed from normal subjects in degree of asymmetry in central (C
3–C
4;
F=6.03, df=1,27,
P=0.02), temporal (T
3–T
4;
F=2.97,
P<0.10; T
5–T
6;
F=5.67,
P<0.03), and parietal regions (P
3–P
4:
F=4.02,
P<0.055).
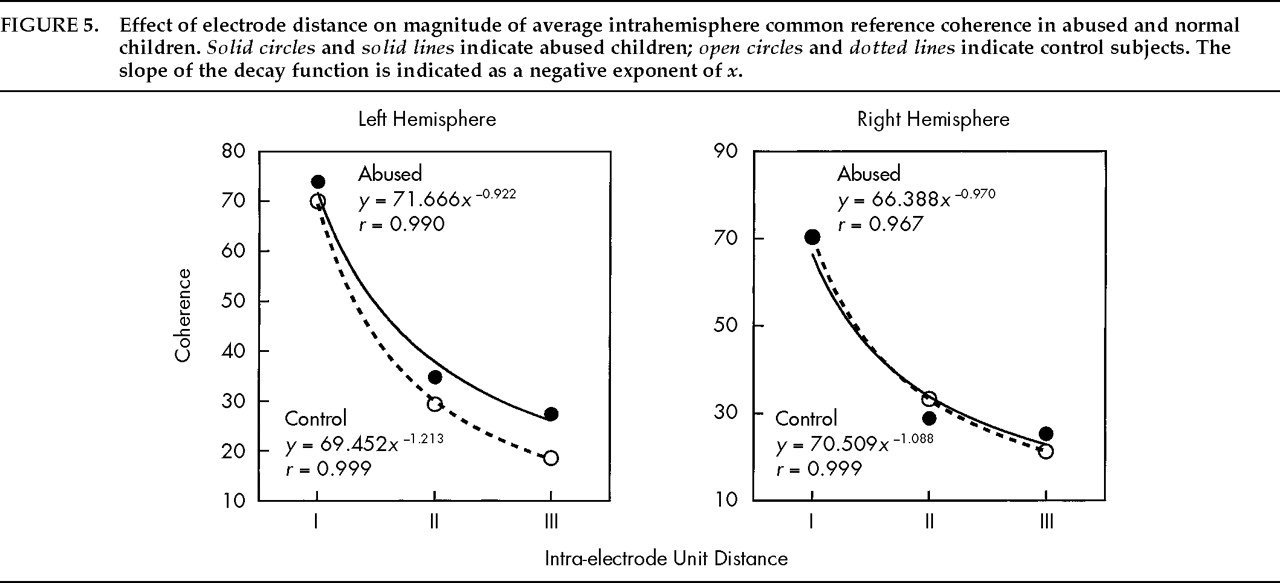
Decay in EEG Coherence as Index of Cortical Differentiation
As seen in
Figure 5, common reference alpha EEG coherence decayed markedly over distance, and the rate of decay was well fit by a power function. In normal control subjects, coherence decayed at a numerically more rapid rate in the left hemisphere (composite group slope =–1.213) than in the right hemisphere (group slope =–1.088), which is consistent with anatomical studies that indicate greater fissuring and higher cell density in the left hemisphere of normal subjects. In contrast, pediatric patients with a history of severe abuse had a lower rate of decay in the left hemisphere than the right hemisphere (composite group slope =–0.922 vs. –0.970; group×hemisphere interaction,
F=4.53, df=1,27,
P<0.05). Overall, normal control subjects had, on average, a 16.3% greater rate of coherence decay (age-corrected) in the left versus the right hemisphere, and abused subjects had a 6.8% lower rate of coherence decay in the left versus the right hemisphere (
F=4.59, df=1,27,
P<0.04). Differences between abused and control patients did not appear to be an artifact of medication use, since average decay rates over the left hemisphere were not significantly affected by medication use (
F=0.40, df=1,12,
P>0.5). Numerically, decay slopes were even lower in the unmedicated abused sample than in the medicated abused sample (decay slope: unmedicated-abused, –0.933; medicated-abused, –1.068).
DISCUSSION
EEG alpha coherence was used to test the hypothesis that childhood physical or sexual abuse may be associated with abnormalities in cortical development. Abused children and control subjects differed significantly in their degree of left versus right hemisphere coherence. Normal children had numerically, but not significantly, lower levels of left hemisphere coherence than right hemisphere coherence. Statistically significant coherence asymmetries of this magnitude have been reported in previous studies using large sample sizes.
22,39,40 It is believed that this normal left<right coherence asymmetry is due to the higher gray to white matter ratio and greater degree of differentiation of the left hemisphere.
22,41 Children with a history of documented abuse had a significant reversal of this natural asymmetry. Differences between abused patients and control subjects were robust and topographically widespread and were more statistically significant than coherence abnormalities previously reported in schizophrenic subjects.
26–31 Abnormalities in abused children were apparent when both common reference and bipolar montage techniques were used, suggesting that this was not an artifact of power of phase differences. Abused children also differed from normal children in the rate of decay of left hemisphere coherence over electrode distance. Left hemisphere coherence decayed over distance with a steeper slope in normal children, suggesting that normal control subjects have a greater degree of left hemisphere cortical differentiation than abused children.
Because EEG coherence is strongly influenced by brain maturation, it is logical to suspect that the left hemisphere differences between abused patients and control subjects arose as a consequence of different rates of maturation. Briefly, regression analyses across age showed that right hemisphere coherence measures in abused patients and control subjects started at nearly the same point at age 6 and rose with parallel slopes through age 15. Regression analyses of composite left hemisphere coherence measures across age also indicated that the regression lines for abused patients and control subjects were virtually identical at age 6. However, these lines markedly diverged thereafter, and they were quite disparate by age 15. Coherence increased much more significantly over age in the abused subjects. The most parsimonious explanation is that during this period a comparable degree of myelination occurred in the left hemispheres of abused subjects and control subjects, increasing EEG coherence, but that this process was offset and attenuated to a more significant extent in control subjects by a greater progression of cortical differentiation.
Medication use appeared to exert a significant effect on common reference coherence measures, but it did not exert a significant effect on bipolar coherence measures or on calculations of coherence decay rates over distance. With common reference measures, the reversed asymmetry was significantly more prominent in the unmedicated abused sample than in the abused patients receiving psychotropic drugs. This result suggests that observed differences in coherence asymmetry between abused and control subjects were not an artifact of medication; indeed, medication effects may have partially masked and obscured group differences. Regional analysis suggested that the most prominent group differences in asymmetry were in central, temporal, and parietal regions rather than frontal regions.
One possible concern is that all of the abused patients were hospitalized and the normal control subjects resided at home. Is it possible that the coherence differences were an artifact of hospitalization? Both groups were tested in the same laboratory under the same test conditions. Unlike conventional EEG measures, coherence largely reflects brain structure, which should not be affected by hospital admission. We found no differences in right hemisphere coherence, but large differences in left hemisphere coherence, indicative of diminished left hemisphere cortical differentiation. It would be neurobiologically implausible to postulate that the abused patients had normal left hemispheres that de-differentiated as a consequence of hospital admission. We have previously reported that hospitalized children with a history of abuse had a much greater prevalence of left hemisphere EEG abnormalities than nonabused hospitalized psychiatric control subjects,
18 indicating that EEG disturbances were associated with abuse rather than hospitalization. The present study sought to ascertain the nature of the left hemisphere abnormality. Finally, we have collected alpha EEG coherence data from adult outpatients with a history of childhood abuse (
n=14) and normal adult control subjects (
n=10). Like the abused children, adults with childhood abuse histories had highly significant reversed asymmetries in their EEG coherence. Hence, the present findings seem to be enduring, and do not appear to be an artifact of hospital status.
Overall, this study represents one of the first experimental attempts to test the hypothesis that early childhood abuse may have a significant impact on cortical development. The present findings of reversed hemispheric asymmetry and greater left hemisphere coherence in abused subjects support this hypothesis. This study, however, is correlational in nature and cannot prove the hypothesis. Alternative explanations can also be entertained. For instance, it is certainly possible that the observed coherence abnormalities were not a consequence of abuse, but rather were a risk factor for being abused. A more complex alternative is that these abnormalities were inherited and were associated with increased risk of abusive behavior on the part of parents or relatives. Designing ethical studies to tease apart these alternative hypotheses will be challenging. However, animal research provides some support for the primary hypothesis by showing that early experience can exert marked effects on hemispheric laterality.
42The most interesting findings to emerge from this program of research are the consistent evidence that early abuse appears to be associated with left hemisphere abnormalities and a reversed left/right hemisphere asymmetry. Thus, the present findings of increased left hemisphere coherence fit with prior observations that early abuse is associated with an increased incidence of left hemisphere EEG abnormalities (nonabused, 3.8%; abused, 22.1%;
P=0.036), and left>right abnormalities on neuropsychological testing.
18 The lack of discernible effect of early abuse on right hemisphere EEG coherence is compatible with our previous finding that early abuse is not associated with an increased incidence of right hemisphere EEG abnormalities (nonabused, 7.7%; abused, 8.8%
18).
From these observations, one can hypothesize that early abuse exerts a more deleterious effect on left cortical development and may impede hemispheric integration and establishment of normal left cortical dominance.
19 Muller
43 theorized that borderline personality disorder may be the result of deficient hemispheric integration. Other theorists have speculated that a dissociation of hemispheric function may be present in alexithymia
44 and PTSD.
45,46Research on hemispheric function strongly suggests that the right hemisphere plays a pivotal role in the perception and expression of emotion,
47 particularly negative emotion.
48–51 Deficient right and left hemisphere integration could result in the misperception of affect and a state of internal confusion or inconsistency.
43,52If it is true that early abuse affects brain development, why should the left hemisphere be more vulnerable than the right? There are a number of possible reasons. The most trivial explanation is that left-sided abnormalities are secondary to physical injury resulting from head trauma. Right-handed adults may be more likely to strike a child on the left side of the head. None of the subjects in the study was known to have sustained traumatic head injury, but we cannot be certain that they did not experience lesser injury. Coherence abnormalities were also present in the subset of patients subject only to sexual abuse, making this hypothesis less likely. The second possible explanation is sampling bias. It is conceivable that early abuse could affect the development of either hemisphere. However, individuals presenting with serious psychiatric disturbances requiring hospitalization may be those with the most pronounced left hemisphere pathology. The third hypothesis is that abnormalities in left hemisphere development stem from concomitant verbal abuse, which conceivably could suppress the development of left hemisphere linguistic centers. The fourth hypothesis is that the more rapidly developing hemisphere would be more vulnerable to the consequences of stress. During the first few months, the right hemisphere develops more rapidly than the left, with more advanced dendritic outgrowth in Broca's area and motor cortex.
53 However, by 5 to 6 months of age dendritic growth in the left hemisphere surpasses that in the right, and it continues at a rapid pace for the next few years. Between 3 and 6 years of age the right hemisphere begins to accelerate in its development, although the left hemisphere remains more highly differentiated. Hence, abuse from 6 months until 3 to 6 years of age may have the greatest differential effect on the left hemisphere. The final hypothesis is that early stress may activate neurotransmitter systems that are asymmetrically distributed, such as norepinephrine,
54 serotonin,
55,56 or dopamine systems.
57 Aside from their transmitter functions, these monoamines strongly influence several facets of brain development.
58–61 Thus, overactivating these systems may produce lateralized developmental effects. Further research will be required to verify these observations and test these hypotheses.
ACKNOWLEDGMENTS
This work was supported in part by National Institute of Mental Health Grant R01 MH53636. The findings were presented at the American Psychiatric Association annual meeting, Philadelphia, PA, May 21–26, 1994; the American Electroencephalographic Society annual meeting, New Orleans, LA, October 10–15, 1993; and the New York Academy of Science, New York, NY, September 9–10, 1996.