Klüver-Bucy Syndrome After Bilateral Selective Damage of Amygdala and Its Cortical Connections
Abstract
CASE REPORT
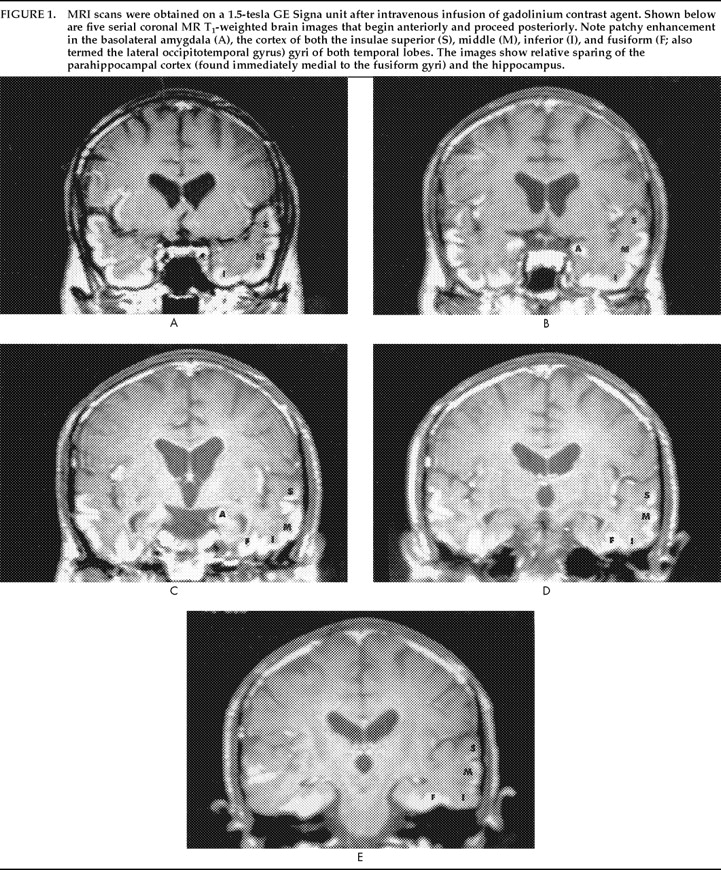
A.B. was a 43-year-old white man. He was married and had a 4-year-old son. A.B. had attended college for 2 years and was employed as an operator at a water plant. His past medical and psychiatric histories were unremarkable.A.B. originally consulted his physician in early January 199 with complaints of sharp pain in his upper chest. He also complained of progressive weakness, sore throat, anorexia, and mild fevers. An ultrasound scan of his gall bladder revealed an enlarged liver and spleen. A liver biopsy was performed, and in February a diagnosis of metastatic malignant melanoma was made. Prior to the pathological confirmation of his disease, A.B. began intra-arterial therapy for presumed hepatocellular carcinoma. This treatment included 5-fluorouracil, doxorubicin, and cisplatin. Following the diagnosis of melanoma, this treatment was discontinued, and he was treated with dacarbazine and interferon alpha. He was subsequently treated with two more courses of chemotherapy as an outpatient. A.B.'s response to this chemotherapy was marked by a reduction in liver size and improvement of his symptoms until early April, when he noted a rapid return of symptoms. A.B. was admitted to the hospital for another course of intra-arterial chemotherapy with doxorubicin, cisplatin, and dacarbazine in mid-April.On April 22 A.B. was taken to the emergency room and was admitted to the hospital after experiencing a generalized seizure. Laboratory test results revealed a low sodium level (102 mEq/l) and pancytopenia (white blood cell count of 700/mm3, hemoglobin level of 8.4 gm/dl, and platelet count of 58,000/mm3). Slightly elevated protein levels (74 mg/dl) in the spinal fluid of the patient were also noted. A.B. was treated with granulocyte colony–stimulating factor (G-CSF), imipenem, and phenytoin. The hyponatremia was corrected over 48 hours to 134 mEq/l. Other medications included corticosteroids, lorazepam (for sedation), and chloral hydrate (for sleep). The patient was also given acyclovir as an antiviral agent pending the results of additional spinal fluid studies.The patient's mental status and orientation gradually improved from the time of his admission until the afternoon of April 24, at which time he became progressively more confused and lethargic. His mental status remained impaired throughout the remainder of his hospitalization. For this condition, he was treated with haloperidol for 2 days (10 mg q 6 hrs) and was then switched to chlorpromazine (50 mg im). During this time (late April and early May), A.B.'s speech did not usually make sense, and many neologisms were present. He uncharacteristically used obscene language and did not recognize his mother, wife, or son. He could not follow commands and did not respond appropriately to questions or other input. He often put objects in his mouth and was observed eating polystyrene containers. On occasion, his behavior was inappropriate and violent: spitting at his son, using foul language, biting people, and trying to kiss his nurse. He sometimes talked of going to a place that he had visited as a child, and he would occasionally pick up the phone and talk as if someone were on the line. His mental state did not appear to be due to a delirium in that it was not transient and was not associated with disturbed arousal, disruption of his sleep–wake cycle, psychomotor agitation, or outright illusions or hallucinations.17MRI scan performed on April 29 was normal. EEG obtained on the same day revealed marked slowing of waves over the entire brain and especially in the frontal regions. However, another MRI scan 9 days later revealed abnormal signal in the amygdalae, hippocampi, and posterior parahippocampal gyri. Damage to the blood–brain barrier, evidenced by gadolinium enhancement, was seen in the amygdala, insular, and temporal gyri, with relative sparing of the parahippocampus and hippocampus structures (Figure 1). Analysis of spinal fluid on April 30 was unremarkable. A brain biopsy specimen was not obtained.The patient was transferred to an inpatient hospice unit on May 13. At the time of his discharge from the hospital, A.B.'s laboratory values had improved (white blood cell count, 11,900/mm3; platelet count, 279,000/mm3; hemoglobin, 11.5 gm/dl).On May 20, a behavioral assessment was attempted. However, A.B. had received lorazepam 2 hours previously and was difficult to arouse. He was unresponsive to commands and appeared unable to comprehend speech. When asked to squeeze the examiner's hand, he attempted to kiss it. His responses to questions were fluent but made no sense. His spontaneous writing was also fluent but contained word substitutions, perseverations, and nonsense words. A second behavioral examination was conducted on the following day with the lorazepam withheld. A.B. was more alert and talkative and was found to be feeding himself appropriately. His Wernicke's aphasia persisted; he could not follow one-step commands or name even simple objects. When he was given a comb, he called it a “saw,” smelled it, wiped it off with his napkin, and set it down. When he was given an apple and a ball, he smelled them, set them down, and said that they smelled good. A.B. did not appear to recognize a cup when it was handed to him, although he was observed to drink coffee appropriately from another cup. When he was asked to write his name, he wrote a phone number (with extra numbers). When he was asked to copy a square, he drew one contiguous with the model and perseverated several other squares. A.B. did not repeat words and did not respond to a ringing phone. He shook the examiner's hand when she offered it at the end of the interview.A.B.'s fluent nonsensical speech, word substitutions, and lack of comprehension indicated a Wernicke's-type aphasia. A.B. could not read, write, or repeat words during the examination. The neurobehavioral evaluation suggested that A.B. was experiencing visual agnosia, meaning that he did not recognize objects (such as the comb and cup) and therefore did not use them appropriately. Although he was observed to be mildly apraxic, he did intermittently demonstrate adequate motor sequencing for object usage, such as picking up the phone and shaking the examiner's hand, suggesting that apraxia could not fully account for his inability to visually recognize and distinguish familiar objects. He had a tendency to examine objects orally; during the first assessment he put everything in his mouth and had been observed eating nonfood objects. During the second assessment he smelled all the objects he was given. According to caregiver reports, his conduct varied between placidity and inappropriately violent or sexual behaviors. This constellation of symptoms (visual agnosia, Wernicke's aphasia, oral exploratory behavior, and altered emotional status), combined with MRI scan results that revealed bilateral mesiotemporal lobe lesions, was consistent with Klüver-Bucy syndrome. Although anecdotal reports of A.B.'s behavior and the presence of bilateral temporal lesions suggest the likelihood of memory deficits, the severity of his language and visual disturbances precluded a formal assessment of memory. Similarly, in light of A.B.'s other cognitive impairments, it was difficult to establish the presence of hypermetamorphosis.Over the next 3 months A.B.'s condition continued to worsen, and he died quietly in August.
DISCUSSION
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).