Corticobasal Ganglionic Degeneration With Balint's Syndrome
Abstract
CASE REPORT
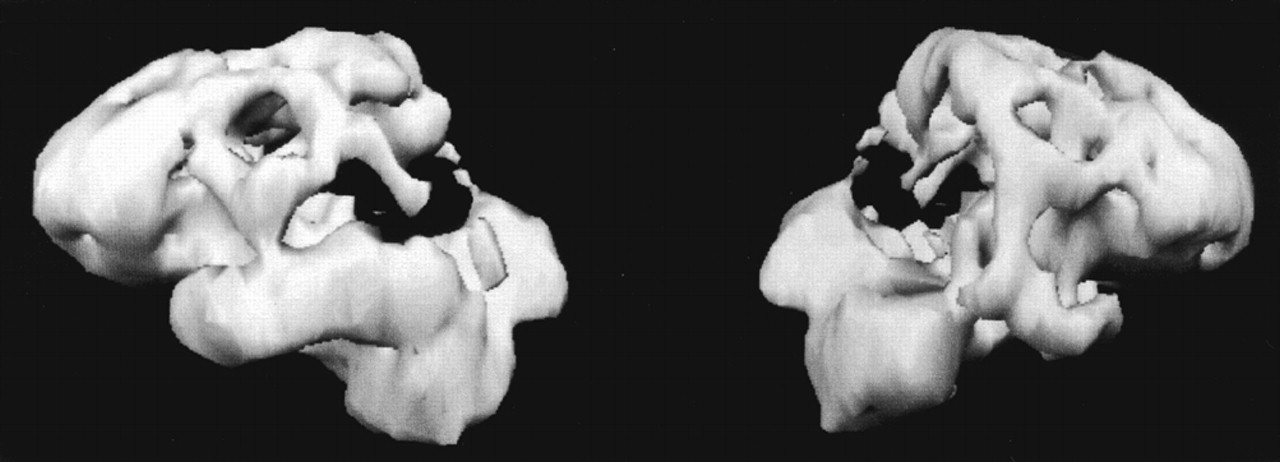
A 65 year-old right-handed man developed “inability to see.” He had difficulty in performing visual tasks such as locating items or orienting himself in familiar surroundings. The patient behaved as if blind, unable to either look at or reach for objects in his environment.The patient had an insidiously progressive disease of 8 years' duration. His illness began with a slow, rigid gait, abnormal posturing of his right hand, and retrocollis. As his disease progressed, he developed difficulty performing manual tasks, particularly with his left hand, such as manipulating his carpenter tools. For a period of time his left arm felt foreign, as if it “did not belong” to him, and it would sometimes elevate on its own (the “alien hand phenomenon”).5 Subsequently, the patient progressed to memory and word-finding difficulty. His past medical and family histories were otherwise unremarkable, and he was on no medications.The patient had prominent visuospatial deficits. He was tested at his best refraction (20/70 OU), and visuospatial tasks were administered untimed. He had difficulty copying drawings such as intersecting pentagons or a cube. When presented with complex scenes such as the Cookie Theft Picture,6 he could not recognize more than one item at a time. He could not identify two adjacent but unlinked drawings (pairs of circles) or large letters made up of smaller ones.4,6 Visuospatial organization was tested with the Hooper Visual Organization Test (30 visual fragments requiring mental reconstruction for identification).6 His responses were based on a single visual fragment, and his scores did not improve even when all of the individual fragments were viewed.The patient could not locate items in his visual field, such as the buttons on his clothes or utensils for eating. He had full extraocular movements on directional command (voluntary saccades), on pursuit, and on oculocephalic reflex stimulation; however, when commanded to move his eyes to specific visual objects in his peripheral fields, he could not do so (“oculomotor apraxia”). When attempting to reach out and touch objects in his peripheral fields with either arm, he would entirely miss them (“optic ataxia”). Infrequently, the patient experienced oculogyric crisis with a locking of his eyes in the upward direction.On further testing, he was alert and attentive but disoriented as to place and date. His language was fluent, and he had intact auditory comprehension for simple pointing and yes-no tasks. Confrontational naming was impaired for common objects, and recent memory was 0 for 4 words at 5 minutes. Despite the absence of motor weakness, he had difficulty performing learned movements with his left arm. He was unable to brush his teeth or wave goodbye with his left upper extremity on verbal command. His attempts at performing these praxis tasks resulted in grotesque motor movements of his left upper extremity. Despite dystonic posturing of his right hand, the patient was able to perform these movements with his right arm. He did not manifest an alien hand phenomenon at the time of examination.The rest of his neurological examination disclosed movement disturbances. He had dystonic posturing of his right hand with spread of his fingers in an athetotic fashion and retrocollic deviation of his head with elevation of his right shoulder. Spontaneous myoclonic jerks occurred in his extremities. The gait was stiff and broad-based, and tone was increased in a leadpipe rigidity. His reflexes were symmetrically brisk, and his toes were upgoing bilaterally.The patient underwent an extensive series of investigations. Magnetic resonance imaging showed cerebral atrophy, and SPECT imaging showed prominent decreased perfusion in posterior parietal regions and, to a lesser degree, in the dorsal frontal regions (Figure 1). After the patient was started on trihexyphenidyl 1 mg bid, the oculogyric crisis resolved and the dystonia and retrocollis decreased, but he continued to show signs of Balint's syndrome.
DISCUSSION
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).