Lyme disease (LYD) is a multisystemic illness caused by the tick-borne spirochete
Borrelia burgdorferi (Bb). LYD, the most common tick-borne illness in the United States,
1 may manifest in a variety of ways: dermatologic, arthritic, ophthalmologic, cardiac, and neuropsychiatric.
2 The incidence and spread of the disease increased during the 1980s,
3 stabilizing somewhat in the late 1990s. Children below the age of 9 are at a high risk for Bb infection,
4 with many new cases of Lyme occurring among persons younger than 14 years.
5The neuropsychiatric symptoms of LYD in adults have been described,
6,7 but little has been published about the neuropsychiatric effect of the disease in children and adolescents. In adults, deficits in attention and memory have been reported.
8,9 In children, a controlled study of cognitive symptoms investigated a sample of all children and adolescents who presented to a LYD clinic, most of whom presented with rheumatological symptoms, had been diagnosed early, and had been treated appropriately for LD.
10 These children were found to have an excellent prognosis for unimpaired functioning. However, this sample may not be representative of all children diagnosed with LYD, especially those who present initially with neurocognitive problems and/or those who were not treated until many months after the initial infection. Our preliminary data using symptom-driven reports suggest that children who develop chronic LYD have psychiatric and cognitive difficulties in the area of attention and memory.
11 However, subjective reports of cognitive dysfunction are not often correlated with objective findings. In a case series,
12 12 of 86 children (14%) developed neurocognitive symptoms associated with chronic LYD. If a subgroup of children develop cognitive problems associated with LYD, then teachers, parents, and physicians should be aware of this possibility. In addition, if our preliminary findings are replicated in a controlled study, then in Lyme-endemic areas it may be reasonable for LYD to be considered in the differential diagnosis of new-onset neurocognitive disorders in children and adolescents.
This study examined the question of whether a subgroup of children with a history of LYD and persistent cognitive complaints have objective cognitive deficits, independent of psychiatric comorbidity.
METHODS
Subjects
Children between 8 and 16 years of age were recruited. Twenty children with chronic LYD and 20 healthy control subjects were enrolled.
Children with a history of LYD who were symptomatic for 6 months to 3 years, with persistent cognitive complaints including memory problems, distractibility, and school decline, were referred by their pediatricians. The diagnosis of LYD was confirmed based on a) history of exposure to a Lyme-endemic area, b) an illness course distinguished by symptoms characteristic of LYD, and c) either 1) history of a physician-documented erythema migrans (EM) rash or unambiguous EM described by a parent, or 2) history of a positive whole-blood polymerase chain reaction (PCR) test for Bb or a positive Western blot meeting explicit current Centers for Disease Control and Prevention (CDC) criteria. The CDC criteria for the immunoglobulin G Western blot (IgG WB) were broadened to recognize that the 31-kD and 34-kD bands represent the highly specific Osp A and B bands. Children were accepted into the study only if LYD infection occurred after completion of a marking period in school. This helped to establish good academic performance prior to the onset of LYD.
Twenty healthy control subjects with no history of LYD were included. An attempt was made to match the groups on gender, age, grade, and socioeconomic status determined by using Hollingshead occupational codes.
13 Healthy children were solicited through the families of children with LYD, including siblings, friends, and relatives. In addition, control subjects were recruited from flyers posted at Columbia Presbyterian Medical Center, although many of these self-referred children were not eligible because they were not fluent in English. Negative enzyme-linked immunosorbent assay and Western blot tests were required for control subjects.
Eligibility for both groups was determined by an extensive phone screen with a physician (B.F.) and by documentation of a positive Western blot assay for the LYD group. No children were accepted into the study if there was a preexisting or pre-Lyme history of significant diagnosed medical, neurologic, psychiatric, or learning problems (including, but not limited to, seizure disorder, head trauma, attention deficit disorders, learning disability, and conduct disorder). Healthy control subjects were not included if they presented with a significant history of any of the following symptoms: arthralgias/arthritis, recurrent neck pain or headache, marked fatigue, EM rash, or cranial/radicular neuropathies. Control subjects were not selected as “super-normals,” since we included all children unless there were marked medical or psychiatric problems.
All procedures were conducted at the New York State Psychiatric Institute, where parents and children gave signed informed consent and were asked to avoid disclosing the diagnostic group of the child.
Cognitive Evaluation
All subjects were administered a neuropsychological battery selected in part to replicate a previous pediatric LYD study.
10 Tests were administered in a standardized manner and in a systematic order. The cognitive domains assessed included 1) general intelligence, using the Wechsler Intelligence Scale for Children III (WISC-III);
14 2) short-term memory for visual and verbal material, using subtests of the Wide Range Assessment of Memory and Learning (WRAML);
15 3) learning of new verbal and nonverbal material, using subtests of the WRAML; 4) attention, using the Conners' Continuous Performance Test (CPT);
16 5) executive functioning, using the Wisconsin Card Sorting Test (WCST)
17; and 6) language, using the word association subtest of the Clinical Evaluation of Language Fundamentals.
18Prior to testing, all children completed a Likert-type scale for physical symptoms, assessing fatigue, joint pain, previous night's sleep, appetite, headache, and other pain, as well as the Children's Depression Inventory (CDI)
19 and the Youth Self-Report (YSR).
20Parents completed a general information questionnaire and a physical symptom checklist (rating symptom severity and frequency over the past year). Parents rated learning and attention problems on the Conners' Parent Rating Scale (CPRS-48)
21 and psychopathology on the Child Behavior Checklist (CBCL).
20Because the present study is not a longitudinal one, the children had no pre-Lyme cognitive assessment. Given that limitation, school grades and standardized achievement test scores were used as an indirect way to assess premorbid cognitive functioning. School records were obtained for the current year and all years starting from the disease onset. Premorbid standardized achievement test scores were also obtained.
Statistical Methods
Statistical analyses were conducted by using SPSS 7.5. The continuous demographic variable of age was contrasted between the two groups by independent-sample t-tests. Demographic variables of socioeconomic class and sex were analyzed between the groups by t-test and chi-square analysis. The neuropsychological test results as well as the self- and parent-report questionnaires were compared by using independent-sample t-tests for the various indices and subtests. Test performance between the groups was also analyzed by analysis of covariance to control separately for differences in Verbal Comprehension, depression, anxiety, and fatigue. Bonferroni correction was applied separately to groups of indices and subtests of the measures to correct for multiple comparisons. Results before and after Bonferroni correction are presented for the reader's information. The CPT's overall assessment of the presence, absence, or possibility of attentional problems was compared between the groups by chi-square analysis. When available, analyses were done using standardized scores procured from published age-corrected normative data. All hypothesis-testing was two-tailed. A P-value of <0.05 was applied for significance.
RESULTS
Patient Characteristics
Twenty children were eligible for the study, and all agreed to participate. There were 13 females and 7 males (mean age 13.83±2.41 years; mean±SD reported throughout). All children were Caucasian, fluent in English, and, consistent with the demographics of Lyme disease, all but one came from middle- or upper-class families. The mean age at diagnosis was 11.90±2.85 years. The mean number of physicians consulted before the diagnosis of LYD was 3.80±4.48. The mean time since diagnosis was 74.95±68.04 weeks; from parent-reported symptom onset until diagnosis, 47.28±44.41 weeks; and from diagnosis to treatment, less than 1 week (0.30±0.92). Thus, these children were symptomatic for many months before being diagnosed and treated.
Of the 20 children with LYD, 16 (80%) had a fully reactive WB and 6 (30%) had a history of an unambiguous EM rash. Of the 4 without a reactive WB, 3 had both well-documented EM rashes and 4/5 bands on an IgG WB, and 1 had a positive whole-blood PCR for Bb DNA and frank arthritis.
All of the children had received oral antibiotics (mean=23.21±21.99 weeks), and 11 had received intravenous antibiotics (8.79±16.10 weeks). All initially benefited from antibiotic therapy, but improvement was sustained in only 10% (2/20) after oral antibiotics and in 36% (4/11) after IV antibiotics. At the time of testing, 7 children (35%) were being treated with oral antibiotics and 2 (10%) were being treated with IV antibiotics.
Based on physician assessment, the most common symptoms during LYD were marked fatigue (100%), arthralgias (100%), frequent and severe headaches (100%), irritability/depression (94%), short-term memory problems (94%), schoolwork deterioration (94%), myalgias (88%), brain fog (88%), neck pain (88%), insomnia (82%), distractibility (82%), word-finding problems (82%), and severe flu (80%). Arthritis was noted in only 38% of the sample. On the more extensive parent-rated questionnaire, children were rated as having moderate to severe sensory hyperacusis to sound (58%) and/or light (74%); insomnia (77%); word-finding problems (79%); and radicular pains (56%).
Thirteen females and 7 males (mean age=13.53±2.67 years) were entered into the study as healthy control subjects. Nine of these children were siblings of children in the LYD group, 6 were friends of children in the LYD group, and 5 were recruited independently. All children were Caucasian and English-speaking. No significant age, sex, or socioeconomic differences were found between the two groups.
Outcome Measures
Neuropsychological Testing:
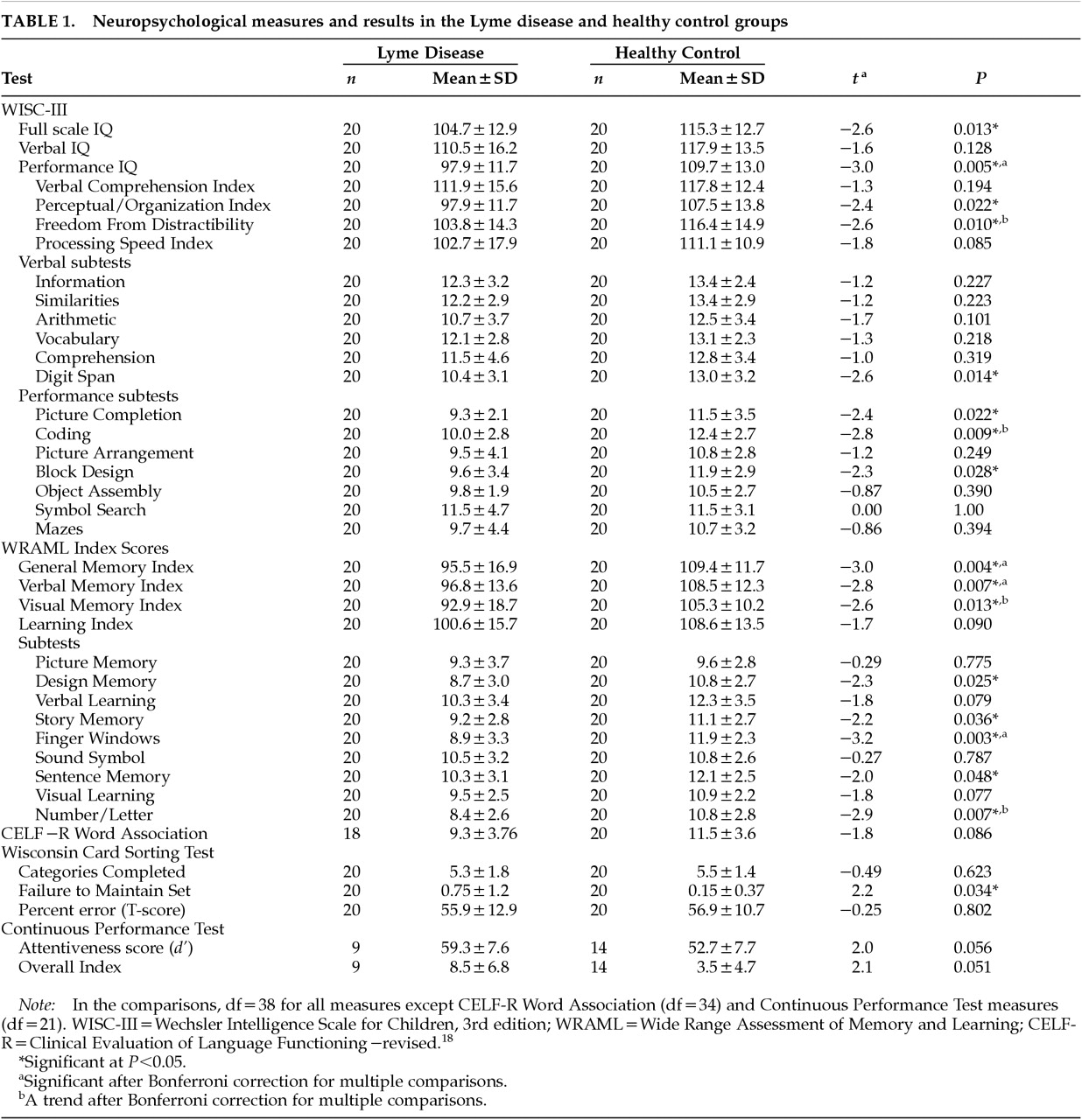
Performance of the groups on the neuropsychological measures was compared (see
Table 1). On two generally accepted measures of preserved premorbid intellectual functioning (Vocabulary and Verbal Comprehension Index), the two groups were not significantly different. On other indices, however, the LYD group had significantly lower scores: Full Scale IQ; Performance IQ; the Perceptual/Organization and Freedom from Distractibility indices of the WISC-III; and the General Memory, Verbal Memory, and Visual Memory indices of the WRAML. The LYD group had significantly lower scores on the digit span, picture completion, coding, and block design subtests of the WISC-III. They had significantly lower scores on the design memory, story memory, finger windows, sentence memory, and number/letter subtests of the WRAML. The LYD group had significantly greater difficulty maintaining set on the WCST. The CPT data are available only for a subset of the subjects because this version of the test was added mid-study. Despite the small
n (9 LYD, 14 Healthy), there was a strong trend for the LYD group to have greater attentional difficulties. There was a significantly greater frequency of definite attention problems in the LYD group than in the control subjects (9:1;
P=0.007). After correction for multiple comparisons, Performance IQ, General Memory Index, Verbal Memory Index, and finger windows remained significant.
Premorbid Academic Achievement:
School grades indicated children in the control group were functioning in the above-average range.
Pre-LYD school grades indicated children in the LYD group had been functioning in the above-average range. Premorbid standardized achievement test scores were available for 14 children (70%) in the LYD group. Eight of 14 children (57%) had scores greater than 90%, 3 (22%) in the 80%–89% range, 1 (7%) in the 70%–79% range, 1 (7%) in the 60%–69% range, and 1 (7%) in the 50%–59% range. For the 6 who were missing standardized tests, pre-Lyme report card grades of A's and B's indicated above-average functioning in school.
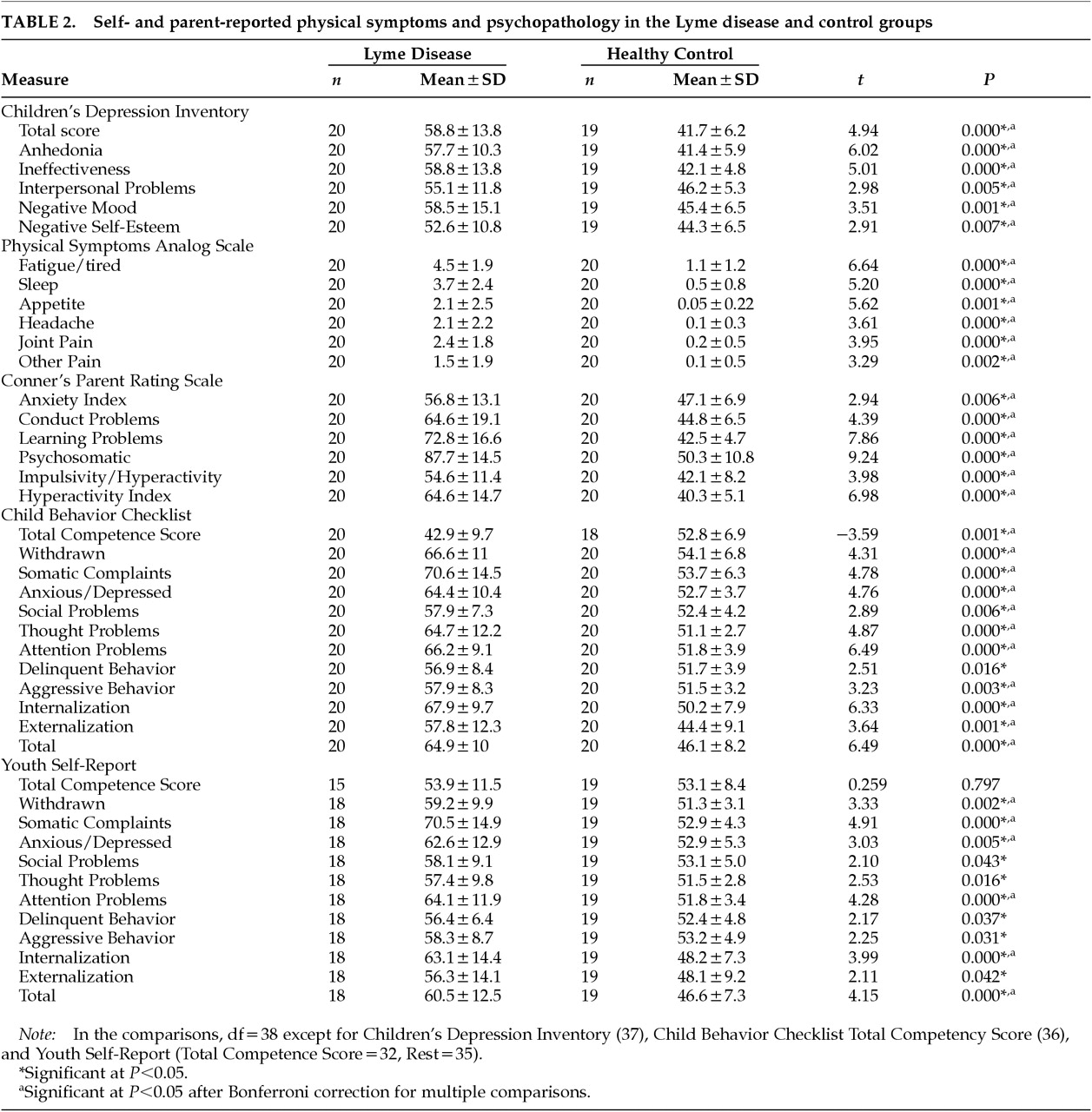
Physical Symptoms and Psychopathology:
The LYD group had significantly elevated scores on all measures of physical distress and parent/child-reported psychopathology. After controlling for multiple comparisons, most scales remained significantly different (
Table 2). Regarding depression, parents indicated that 41% (7/17) of children with LYD had suicidal thoughts and 11% (2/18) had made a suicide gesture. On the child rating (CDI), 40% (8/20) had suicidal thoughts. The LYD group scored far worse on measures of learning problems and hyperactivity: almost 7 SD above the control subjects' mean on the CPRS Learning Problems scale, and 5 SD above the controls' mean on the Hyperactivity Index scale.
Because affective disorders influence cognitive performance, the data were analyzed in an attempt to control these potentially confounding variables. Depression did not account for group differences in Perceptual/Organizational Index (P=0.050), General Memory Index (P=0.045), Verbal Memory Index (P=0.021), digit span (P=0.045), coding (P=0.002), design memory (P=0.034), finger windows (P=0.011), or number/letter (P=0.003). Parent-rated anxiety did not account for differences in Performance IQ (P=0.027), Visual Memory Index (P=0.049), coding (P=0.038), finger windows (P=0.005), or number/letter (P=0.038). Self-ratings of fatigue did not account for differences in digit span (P=0.038), finger windows (P=0.016), or number/letter (P=0.024). When we attempted to statistically control for depression, anxiety, and fatigue together, three non-independent variables, group comparisons for many index and subtest scores failed to attain statistical significance. However, finger windows (P=0.022) and number/letter (P=0.010), two important tests of visual and auditory processing, continued to be significantly different between the groups.
DISCUSSION
In adults, LYD can cause significant cognitive deficits, specifically in the domain of memory. This is one of the few controlled studies of the cognitive sequelae of LYD in children. We did not attempt to study the prevalence of cognitive deficits in children with LYD. Rather, we have described a subgroup of children who developed persistent neuropsychiatric complaints subsequent to the onset of LYD, despite having been premorbidly neuropsychiatrically healthy. Thus, our LYD group was defined by their cognitive complaints. We were interested to see if these children would have objective cognitive deficits as well. The LYD group was compared with healthy control subjects and was found to have comparable premorbid intellectual functioning. The groups were compared on multiple neuropsychologic, self-report, and parent-report measures. Our results indicated that compared with control subjects, the Lyme sample had significantly more psychopathology and more objective cognitive deficits.
Our prior work
11 indicated that children with chronic LYD had higher rates of anxiety, mood, and behavioral disorders than children without LYD. Our current study specifically recruited patients with cognitive complaints, not psychiatric ones, and hence may be less likely to suffer from a referral bias in the area of psychopathology. Yet the children with LYD had significantly higher rates of psychopathology than control subjects across various domains.
Both children and parents agreed that these children had difficulty with learning and focusing attention. The self-report forms indicated that learning and attention problems, feelings of ineffectiveness, and mood problems were significantly greater for the LYD group compared with the control group. These findings are important because children with LYD who present with psychiatric problems may be misdiagnosed as having a primary psychiatric problem such as an affective disorder, oppositional defiant disorder, or attention deficit disorder.
In order to assess the meaning of our findings, we examined whether our children with LYD had premorbid cognitive abilities comparable to the control subjects. On the available standardized tests and school grades, the two groups appeared comparable. The groups did not differ on the particular neuropsychological measures that tend to be least affected by brain injury (measures of vocabulary and verbal abstract reasoning). Thus, the two groups appeared to have similar cognitive endowments.
On the neuropsychological measures of cognitive functioning, children with LYD had significantly lower scores on certain measures. As with the self-report measures, the particular areas of deficits fell within a pattern. On the standardized measure of intellectual functioning (WISC-III), the deficit in Performance IQ suggests a problem in overall perceptual and organizational abilities, and the lower Freedom from Distractibility score suggests a problem with attention and concentration. Visual and auditory tracking or scanning difficulties could account for these results.
On standardized tests of memory, deficits were noted in both visual and auditory primary processing as well as visual memory. These deficits might mislead one to think that these children have primary memory problems. However, the two groups did not differ on the Learning Index, indicating intact ability to learn and recall/recognize both visual and auditory material over trials. In other words, children when presented with complex information may initially “miss” some of it, but with repetition they can both learn and remember.
The data from the Continuous Performance Test are more difficult to interpret because of the small sample size. However, the groups significantly differed on the percentage in each group who had attention problems based on an overall categorical rating. The trend seen for the Lyme group to have higher scores on Attentiveness (d') and Overall Index indicated that these children had difficulties in perceptual sensitivity—that is, in discriminating the perceptual features of signals from non-signals.
Taken as a whole, our study demonstrated that a group of children with LYD had a pattern of cognitive deficits, as defined by both objective measures of cognitive functioning and self-report measures. Since these children were included because of their cognitive complaints and we do not have any premorbid objective cognitive assessments on the children with LYD, we cannot say for certain whether these cognitive deficits are caused by LYD. However, the objective neuropsychological findings and the subjective parent and child report measures all point to deficits in visual and auditory attention, or in working memory and mental tracking, in children with cognitive problems associated with LYD. These particular functions tend to be very sensitive to brain injury and disease. As noted above, these types of deficits may be incorrectly perceived by the patients and others as memory impairments, since the new information is not attended to and processed and therefore will not be recalled. Consistent with this possibility are the reports by children and parents that the children with LYD had increased short-term memory problems, such as forgetting homework assignments.
Our findings were consistent with the cases reported by Bloom et al.
12 but differed from the findings of Adams et al.
10 An important difference between the two studies is that Adams and colleagues' sample was taken from a clinic population of all LYD cases, in which only approximately 22% of the population presented with mental status changes and neurological involvement. Their sample may be more reflective of a rheumatological LYD population than a neurological LYD population.
This study has several limitations. First, because of the small sample size, only large differences can be detected between groups. Second, it would be useful to know whether the control subjects and the patients were premorbidly comparable on cognition. This would have been possible only if all children had been given identical standardized testing at a similar age. Such was not the case. Premorbid standardized achievement test scores were available for only some of the Lyme group, and quantitative school grades were not available for all children. Given the information available to us, however, it does appear that the two groups were premorbidly comparable on academic performance. Third, it would be useful to know whether the cognitive performance of our Lyme patients differed from that of other chronically ill children who do not have a disease that affects the central nervous system, or of children who have LYD without neurologic involvement. Only with such a comparison group can we be certain that the cognitive profile of our patients reflects a disease process that actually affects the brain, as opposed to the nonspecific effects of a chronic illness.
CONCLUSION
Our study highlights the presence of attentional problems in a sample of children who develop persistent cognitive symptoms after LYD. Published pediatric studies on LYD often include only children with either early localized or early disseminated LYD. These children tend not to develop long-term problems, perhaps because treatment was initiated early. In contrast, our study demonstrates that children whose diagnosis and treatment are delayed may suffer considerable impairment. The present study, comparable to Belman et al.
22 and Bloom et al.,
12 indicates that children with chronic neurologic LYD can have significant neuropsychiatric problems. Our study raises the question of whether a repeated course of antibiotics would be helpful. Only a placebo-controlled treatment study can answer this question and determine whether neuropsychiatric problems are due to past damage or secondary to persistent infection.
Our findings have relevance to mental health professionals as well as educators working in Lyme-endemic areas, who may be the first to recognize the possible underlying infectious origin of the neuropsychiatric disorder. Recognizing that LYD may present with neuropsychiatric symptoms can lead to timely diagnosis and treatment. Furthermore, identification of children with persistent neuroborreliosis is imperative so that these children can receive the most appropriate medical, psychological, and educational assistance.
ACKNOWLEDGMENTS
This research was supported in part by a New York State Psychiatric Institute Research Support Grant to Dr. Tager and by a grant from the Lyme Disease Association of New Jersey to Dr. Fallon. Portions of this work were presented at the annual meetings of the Academy of Child and Adolescent Psychiatry (Anaheim, CA, October 1998), the International Neuropsychological Society (Boston, February 1999), the American Psychiatric Association (Washington, DC, May 1999), and the International Conference on Lyme Borreliosis (Munich, Germany, June 1999).