Psychiatric Features and Disturbance of Circadian Rhythm of Temperature, Pulse, and Blood Pressure in Wilson's Disease
Abstract
METHODS
RESULTS
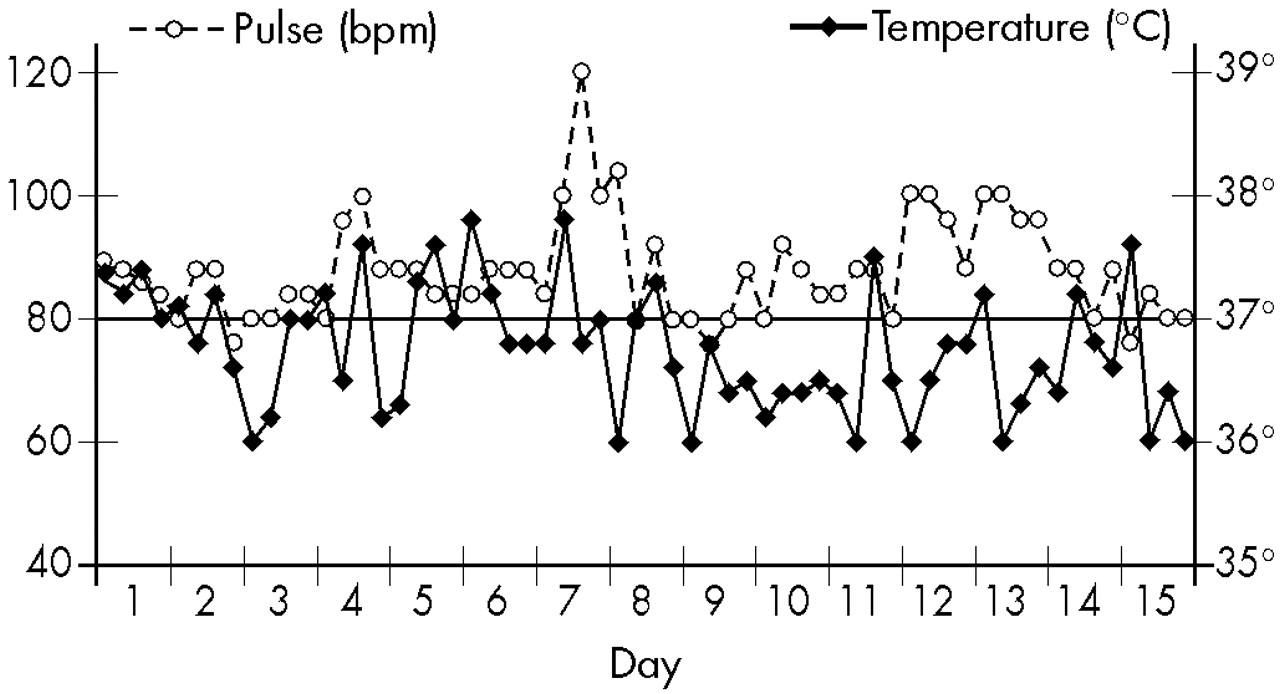
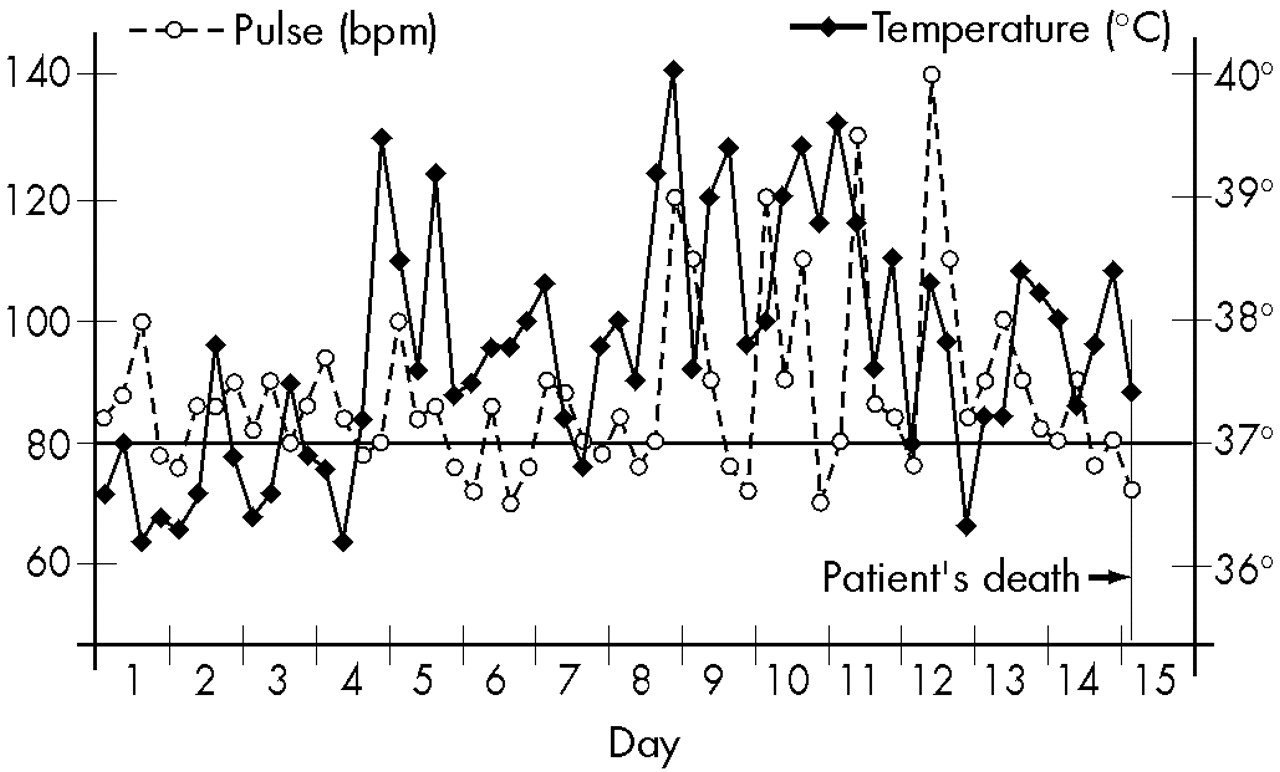
Case 1. A., 15 years old, had a normal development and behavior until the age of 15, when, after an emotionally traumatic experience, she manifested quick involuntary movements, first of the right arm and progressively extending to other parts of the body, which disappeared spontaneously after 2 months. About 3 months later, she started avoiding social contact, had no spontaneous speech, and often reported auditory hallucinations. The diagnosis of schizophrenia was made and she was treated with chlorpromazine by a psychiatrist, with slight improvement in the first months, but later the symptoms reappeared. Eight months after the beginning of the disease, she was examined in CAPS and was hospitalized in April 1963. In the ward, she maintained the clinical picture described above. However, the intensity of the symptoms was reduced when she was alone and increased significantly in the presence of members of CAPS' staff. In addition to the involuntary movements, neurological examination revealed only a mild generalized hypertonia, and these symptoms were attributed to the recent use of neuroleptic. Even so, A. was administered some laboratory examinations, including EEG and cerebrospinal fluid (CSF), and the results were normal. The daily temperature, recorded only in the morning, remained in the range of 36.4° to 37.8° Celsius; P ranged from 80 to 100 per minute, and BP remained between 120/70 and 140/80. On the basis of these results, the characteristics of her behavior, and the fact that the disease had appeared after an emotional trauma, diagnosis of hysterical conversion was made. She was treated with psychotherapy and tranquilizers and showed great improvement. Involuntary movements seldom appeared in the arms; she had normal behavior, no longer reported hallucinations, seemed happy, and was discharged after 2 months of hospitalization.In October 1964, A. returned to CAPS outpatient service, and her parents reported that she had been well until the preceding week, when the symptoms had reappeared. Once again she was hospitalized. On this occasion, she was dysarthric, had involuntary movements in the upper and lower limbs, and walked with difficulty, tracking to the left side; she exhibited hypertonia alternating with normal tonus in several muscular groups, and Babinski sign in the right foot. A discrete cognitive impairment in comparison with the preceding examination was detected. No hallucinations were then reported. Autonomic functions were recorded every 6 hours and revealed abnormal changes: BP oscillated between 100/60 and 150/100; T and P changes are shown in Figure 1.Pneumoencephalography of the brain was then performed, revealing a ventricular dilatation and cortical atrophy. This time, EEG showed diffuse slow-wave discharges. The total serum copper level was low (30 μg/dl, vs. normal 70–160 μg/dl), and the ophthalmologic examination detected the presence of Kayser-Fleischer rings. The diagnosis of Wilson's disease was now evident, but her physical condition quickly deteriorated; she became semicomatose and died a few days later, in December 1964. During the days preceding death, BP oscillated between 140/100 and 180/120. Even though no infectious focus was detected, she had almost continuous high fever that did not cease with antipyretics, and the changes in T and P also increased, as shown in Figure 2.
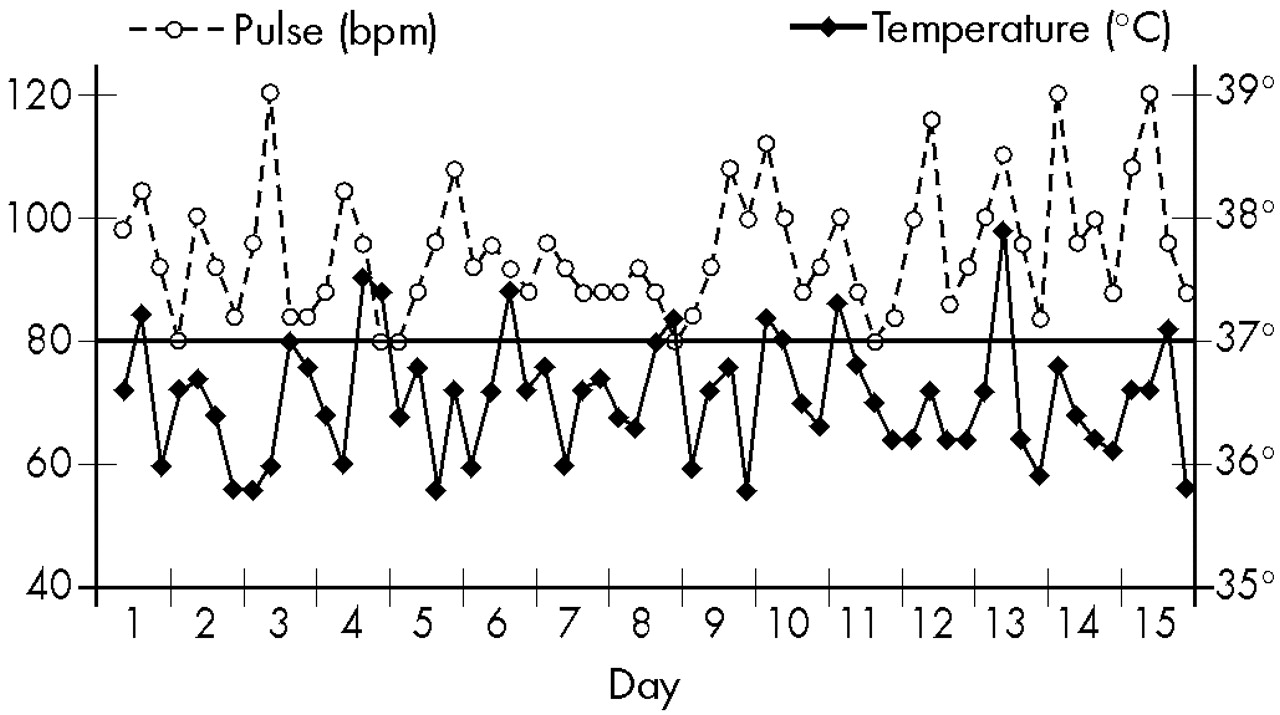
Case 2. B. had normal behavior, was healthy, and was a good student until the beginning of her illness. When she was 13 years old, there appeared a slow and progressive change of behavior: she became very quiet, stopped speaking spontaneously, gave laconic answers in a very low voice, had unmotivated crises of laughing, crying, or aggressiveness, was inattentive, and had almost no initiative. Four months later she was examined by a psychiatrist, who diagnosed schizophrenia and prescribed chlorpromazine. A few days later B. developed difficulty swallowing and tremors in the extremities, which were attributed to a side effect of the neuroleptic.As she did not improve with treatment, she was brought to CAPS in 1969 and hospitalized 10 months after the beginning of the disease. In the ward, she maintained the same behavior described above. On clinical and neurological examination the only abnormalities were a discrete hypertonia of the extremities and slight reduction of the stretch reflexes, which could be attributed to the recent use of neuroleptic. However, BP, recorded every 6 hours, oscillated between 100/60 and 140/100; T and P also showed abnormal changes, and febrile peaks appeared in absence of infection, as shown in Figure 3.These abnormalities suggested a hypothalamic dysfunction and the need of a broader laboratory investigation. A hemogram demonstrated eosinophilia. All other results, including EEG, CSF with protein electrophoresis, urine and feces analyses, glycemia, and levels of bilirubin, antistreptolisin, and immunoglobulin (IgG, IgA, IgM), were normal. However, an ophthalmic examination detected the presence of Kayser-Fleischer rings, the total serum copper level was low (50 μg/dl), and a diagnosis of Wilson's disease was made. For this reason, she was transferred to the Neurologic Clinic for treatment.
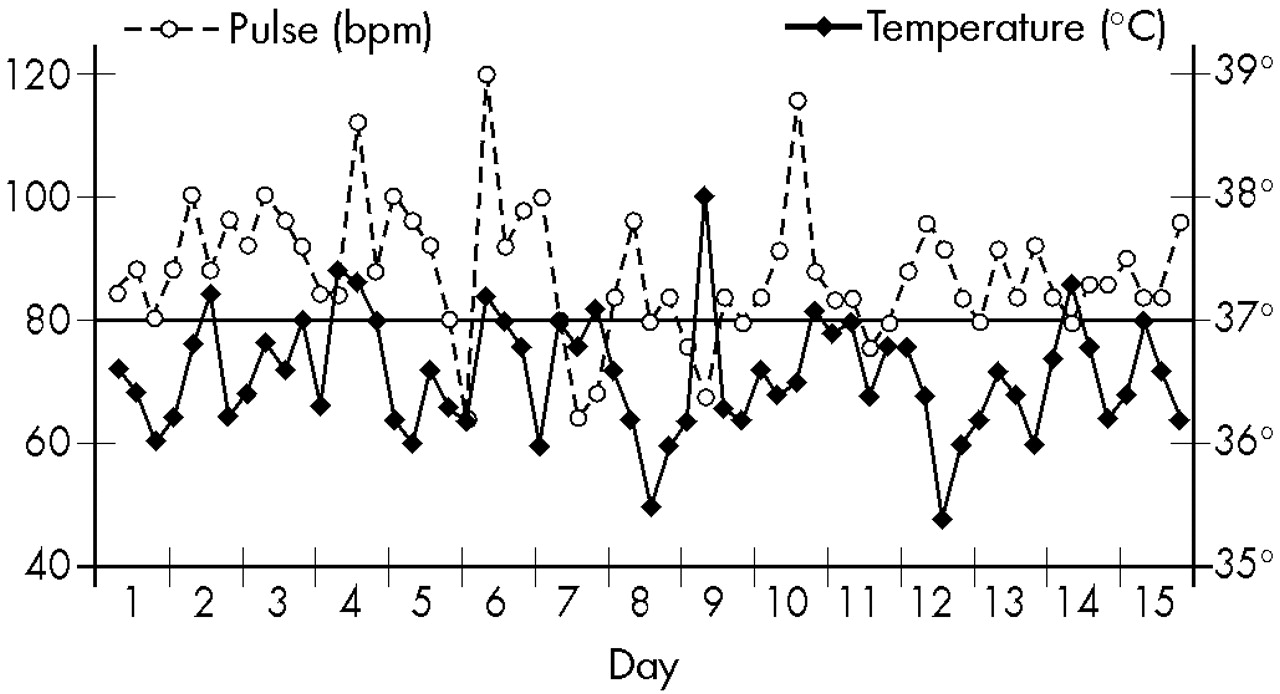
Case 3. C. had a normal development, was calm and sociable, and was a good student. When she was 12 years old, her behavior changed, with a progressive reduction of initiative, daily activity, and verbal communication, in addition to crises of aggressiveness. Two months later, she experienced difficulty in swallowing and developed hand tremors. She was examined by a clinician who prescribed glutamic acid and phosphate. According to the parents' information, dysphagia and tremors disappeared but psychiatric symptoms persisted. For this reason, she was brought to CAPS 10 months after the beginning of the disease. The psychiatric examination indicated reduced attention, slow movements with tendency to immobility, and inexpressive mimicry. She did not speak spontaneously and gave laconic answers to some questions, in a very low voice. Sometimes she cried without tears, but this ceased abruptly. No delusions or hallucinations were reported. Her nutritional condition was good, and neurological examination detected only slight intentional tremors of both hands.In 1975, C. was hospitalized and maintained the same behavior described above, which was compatible with the diagnosis of schizophrenia. However, during her first days of hospitalization, and without any treatment, instability of autonomic functions was detected: BP oscillated between 90/60 and 160/120; changes in T and P were also abnormal, as shown in Figure 4.Because of a hypothesized hypothalamic dysfunction, laboratory examinations were then done: the hemogram revealed eosinophilia. Feces, urine, EEG, and CSF examinations gave normal results. However, computed tomography showed a cortical atrophy and enlarged ventricular system. The total serum copper level was below normal (30 μg/dl), and the ophthalmologic examination detected the presence of Kayser-Fleischer rings. While lab results were pending, the patient developed dysphagia and involuntary tremors of the extremities. The diagnosis of Wilson's disease was made, and the patient was transferred to the Neurologic Clinic for treatment.
DISCUSSION
ACKNOWLEDGMENTS
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).