Many studies show that hypofrontality, hypometabolism or hypoperfusion in the frontal lobe, is indicated in affective disorders
1–3as well as schizophrenia.
4–8 Although the biological mechanism of hypofrontality is unclear, several studies suggest a possible involvement of vascular factors.
9–12 Therefore, we hypothesize that functional hypofrontality, that is hypofrontality during cognitive activation, is partly caused by dysfunction between cerebral neuronal activation and cerebrovascular response. Conventional functional brain imaging techniques, such as positron emission tomography or single-photon emission tomography, are not suitable to assess our hypothesis because repeated and continuous measurement is restricted due to radiation exposure and motion artifacts, and it is difficult to observe dynamic time-dependent cerebrovascular response due to limited time resolution. Although, functional MRI can help solve these problems, it is difficult to measure cerebrovascular response to hyperventilation or respiration of carbon dioxide because of motion artifacts, especially refid="RD4661in psychiatric patients. Therefore, there has been little information about cerebrovascular response to physiological stimulation in schizophrenia and affective disorders.
Near-infrared spectroscopy (NIRS) is a new, noninvasive optical method that measures the change in oxygenated hemoglobin (oxyHb) and deoxygenated hemoglobin (deoxyHb). Several studies show that NIRS can measure cerebral blood volume and cerebral oxygenation during cognitive activation in healthy subjects repeatedly, conventionally, and safely in high time resolution
13–15 without being influenced by minor motions of the body. Therefore, NIRS is suitable to assess the relation between cerebral neuronal activation and cerebrovascular response.
Studies with one-channel NIRS showing that patients with senile depression had functional hypofrontality in the left frontal lobe
16 and that cerebrovascular response to hyperventilation differs from controls
17 suggest that the basis of hypofrontality may be associated with cerebrovascular dysfunction. However, it is necessary to measure the bilateral frontal lobes since affective disorders and schizophrenia had altered cerebral lateralization in several studies.
18–22 Recently, multichannel NIRS was developed, and we can now measure cerebrovascular response bilaterally. In the present study, we preliminarily applied 24-channel NIRS to healthy subjects during cognitive tasks and hyperventilation, which caused cerebral vasoconstriction with hypocapnia
23, and we assessed the test-retest reliability.
METHODS
Subjects
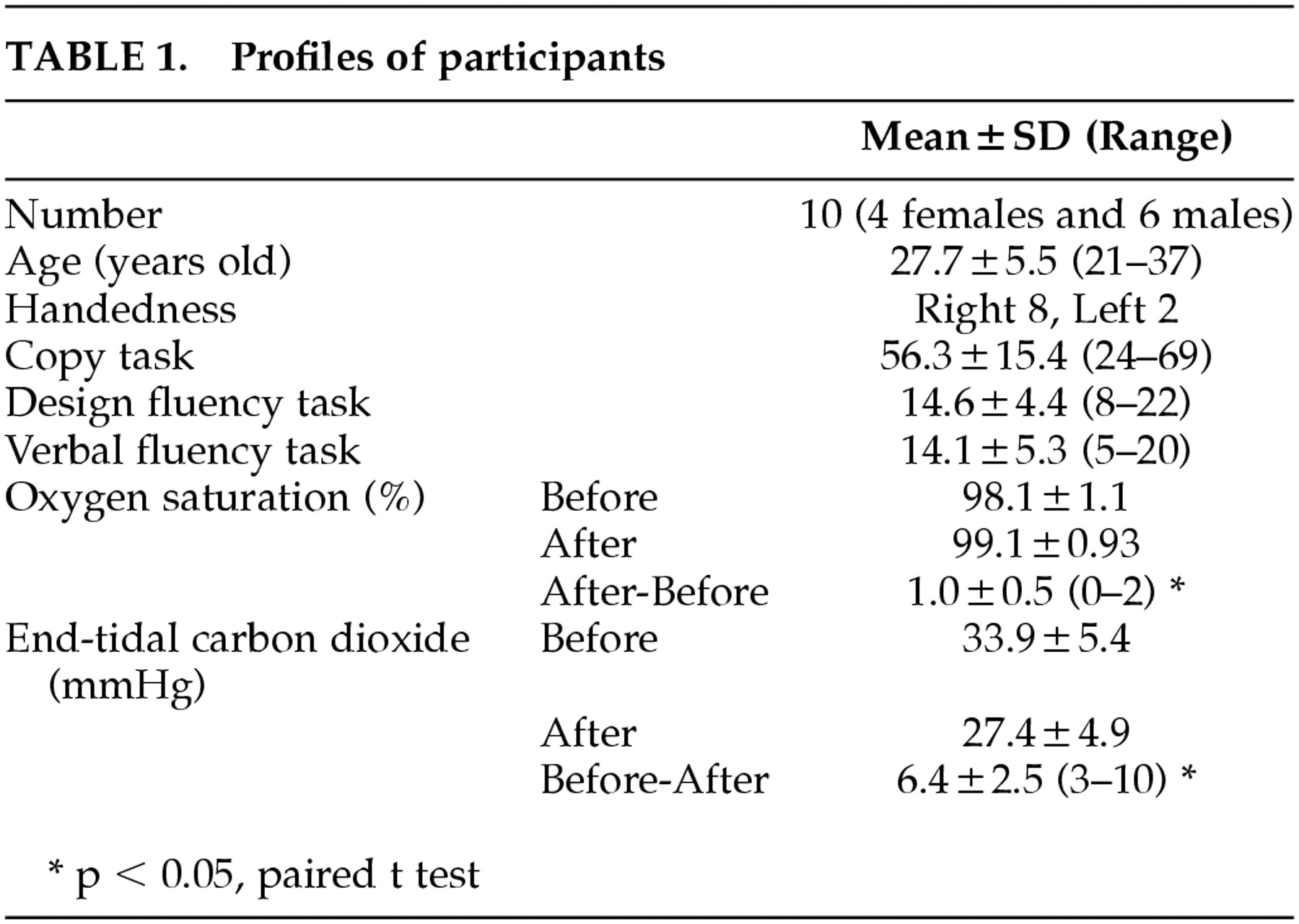
Ten healthy subjects (4 females and 6 males) participated in this study. Their mean age was 27.7 +/−5.5 (mean +/−SD) years old (from 21 to 37 years old). Eight were right-handed, and two were left-handed according to the result of the Annett's scale (cut off < 0.8).
24 Their profile is shown in
Table 1. The subjects were interviewed by a psychiatrist (T.K. or A.W.) to exclude patients with psychiatric illnesses, and they were screened using a questionnaire on medication and physical condition to exclude general medical diseases (hypertension, hyperlipidemia, and diabetes mellitus etc). All participants gave written informed consent before participating in this study. The experiment was repeated on a different day to evaluate the test-retest reliability in five of 10 subjects, and the mean interval was 205±218 days (13–462). This study was approved by the ethical committees of the University of Tokyo and Brain Science Institute.
Tasks
We applied the design fluency task and verbal fluency task as cognitive tasks, which have been reported to activate the frontal lobe,25 and the copy task and word repetition as control tasks to exclude the effect of writing and speaking, respectively. We applied the hyperventilation as physiological stimulation, which causes cerebral vasoconstriction due to hypocapnia. After the procedure was described to the subjects before the test, they were seated in comfortable chairs and asked to follow the audiotaped instructions. The procedure of the test is below.
Rest 2 minutes.
Copy task (CP) 1 minute-The subjects were asked to repeatedly copy the triangle shape. This was the control task for the design fluency task. After this task, subjects had a 2-minute rest.
Design fluency task (DF) 1 minute-The subjects were asked to invent novel figures, as many as possible: Figures of actual objects (i.e., house), identifiable forms (i.e., star shape), and mere scribbling were not allowed. Three correct examples and three inadequate examples were shown on the paper. The score was the number of novel figures. After this task, subjects had a 4-minute rest.
Word repetition (WR) 1 minute-The subjects were asked to repeat the letters spoken by the tester. This was the control task for the verbal fluency task. After this task, subjects had a 2-minute rest.
Verbal fluency task (VF) 1 minute-The subjects were asked to generate and speak as many words as possible beginning with a specified letter. The score was the number of words generated in 1 minute. After this task, subjects had a 2-minute rest.
Hyperventilation (HV) 3 minutes-The subjects were asked to hyperventilate as deeply as possible, following the tester's instruction. Each subject wore face mask, and a pulse oximeter (Nippon Kohden, Japan, OGS-2001) was attached on a finger during hyperventilation to check whether the subject properly performed hyperventilation by measuring oxygen saturation, heart rate, end-tidal carbon dioxide, and respiration rate. This task evaluates cerebral vasoconstriction caused by hypocapnia. After this task, subjects had 2-minute rest.
Near-Infrared Spectroscopy (NIRS)
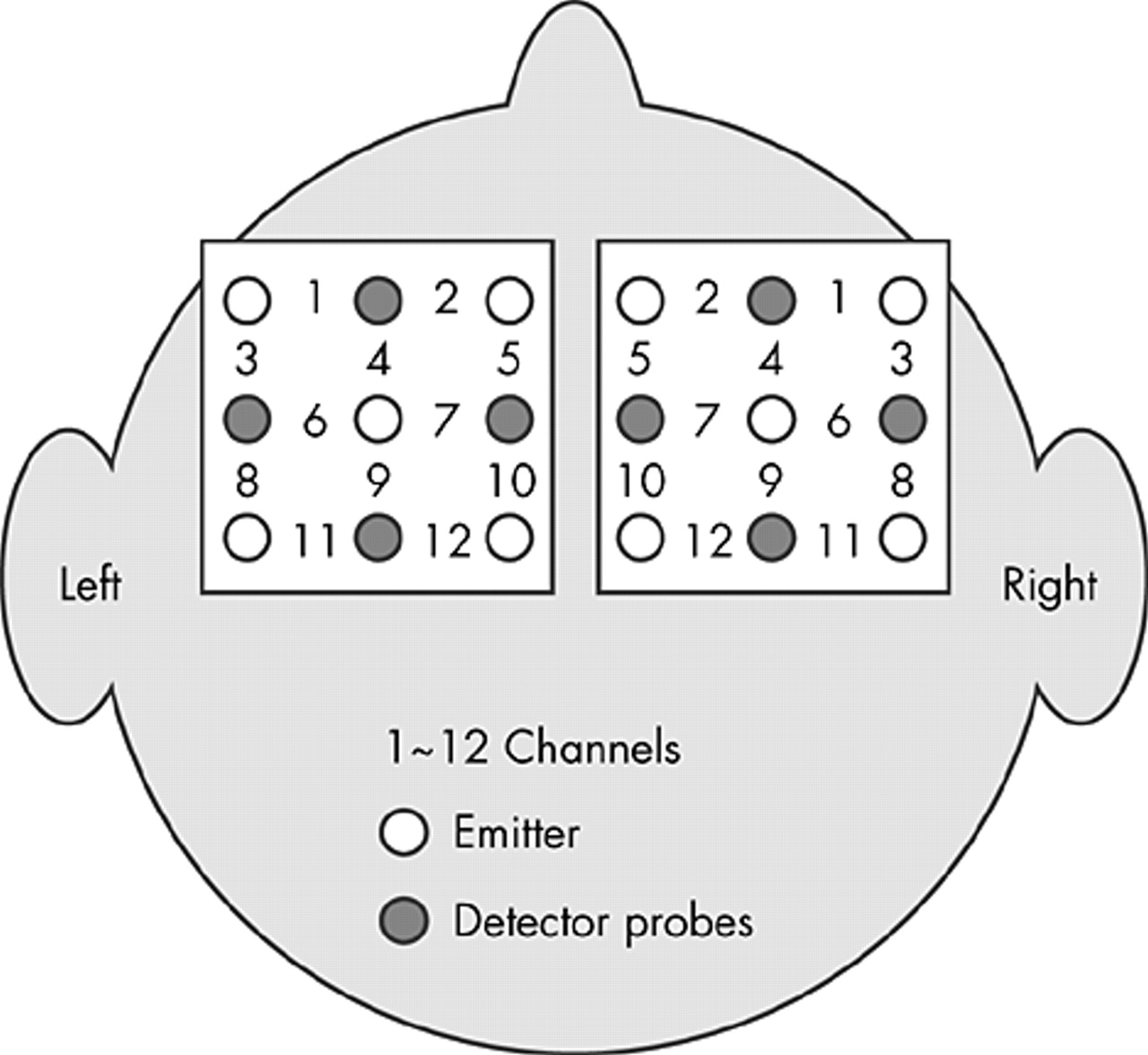
For the NIRS measurement, a 24-channel NIRS system, ETG-100 (HITACHI Medical, Tokyo, Japan) was used. Nine probes (5 emitter and 4 detector probes) each were attached to the left and right frontal area in the formula of 3×3 square (
Figure 1). The distance between an emitter probe and detector probe was set at 3.0 cm, and the most central and frontal probe was set at 1.0 cm from the supraorbital margin. The time resolution was set at 1 sec. We obtained three parameters, oxyHb, deoxyHb, and totalHb (the sum of oxyHb and deoxyHb), respectively, from all 24 channels.
Statistics and Analysis
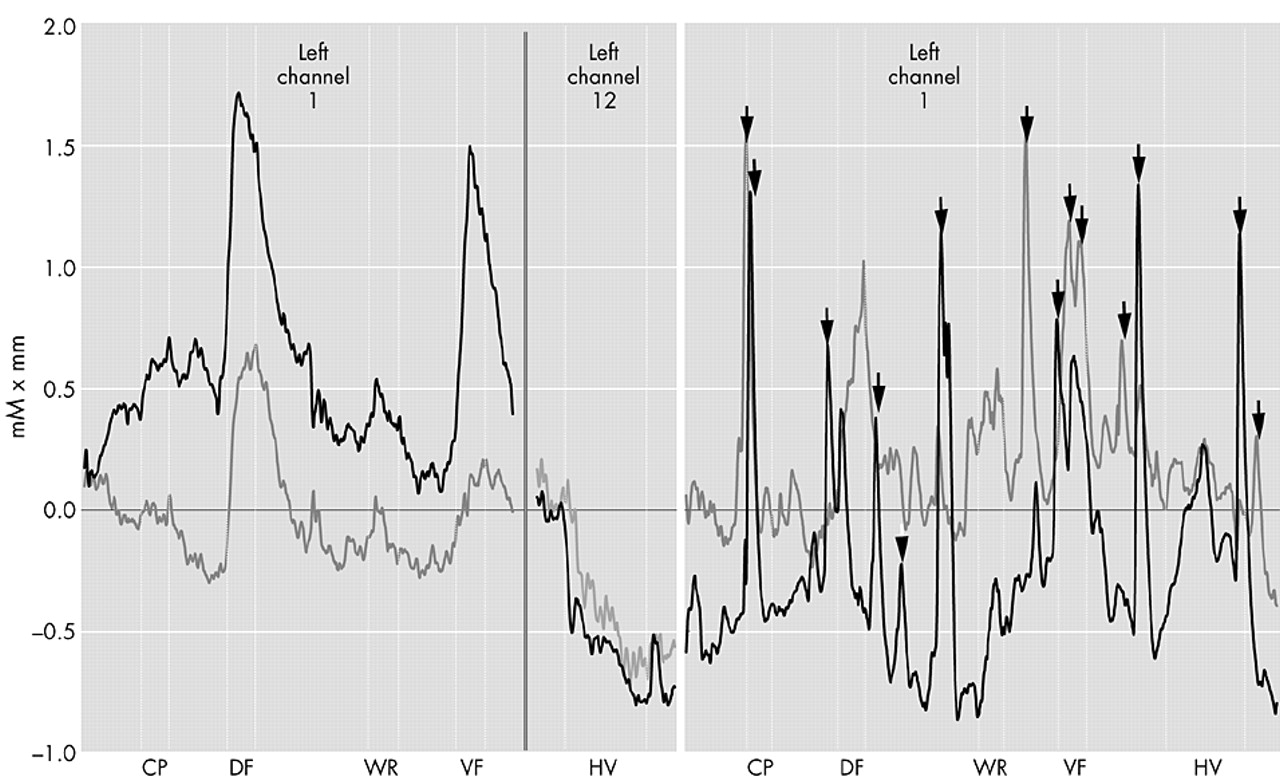
We adopted the average oxyHb, deoxyHb, or totalHb values during the task (1 minute), subtracted from the average value before the task (1 minute) as the averaged value in each task. We performed repeated measures ANOVA (2 hemispheres×12 channels×5 tasks). Three main effects (hemisphere, channel, and task), two 2-way interactions (hemisphere×task and channel×task), and one 3-way interaction (hemisphere×channel×task) were considered in the model. When there was a significant main effect or interaction, we performed repeated measures ANOVA (2 hemispheres×12 channels×2 tasks) in each pair of controls and target tasks (CP versus DF, WR versus VF, and before HV versus HV) with a similar model, and Student's t test between the control and target task was applied to highlight the channel that was activated by a task.
DISCUSSION
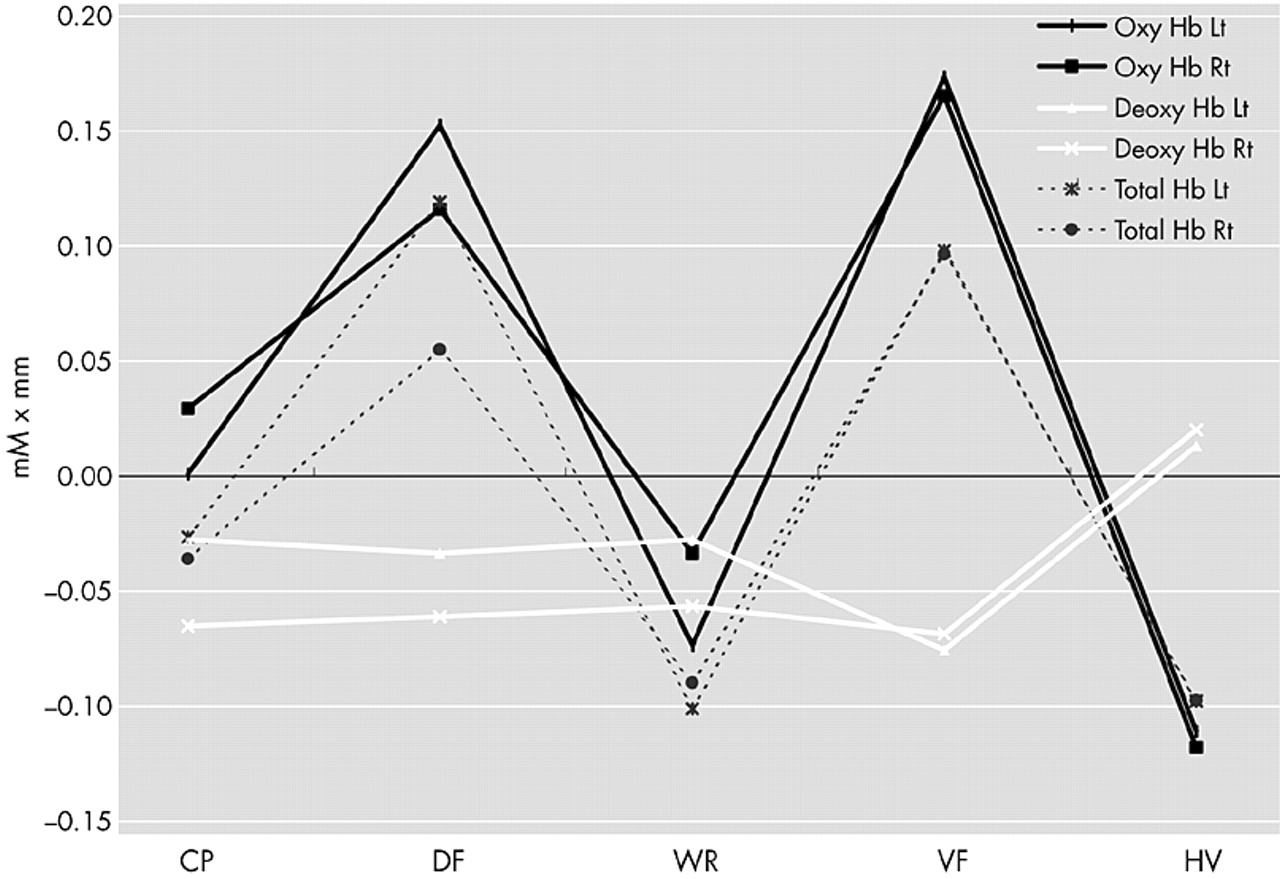
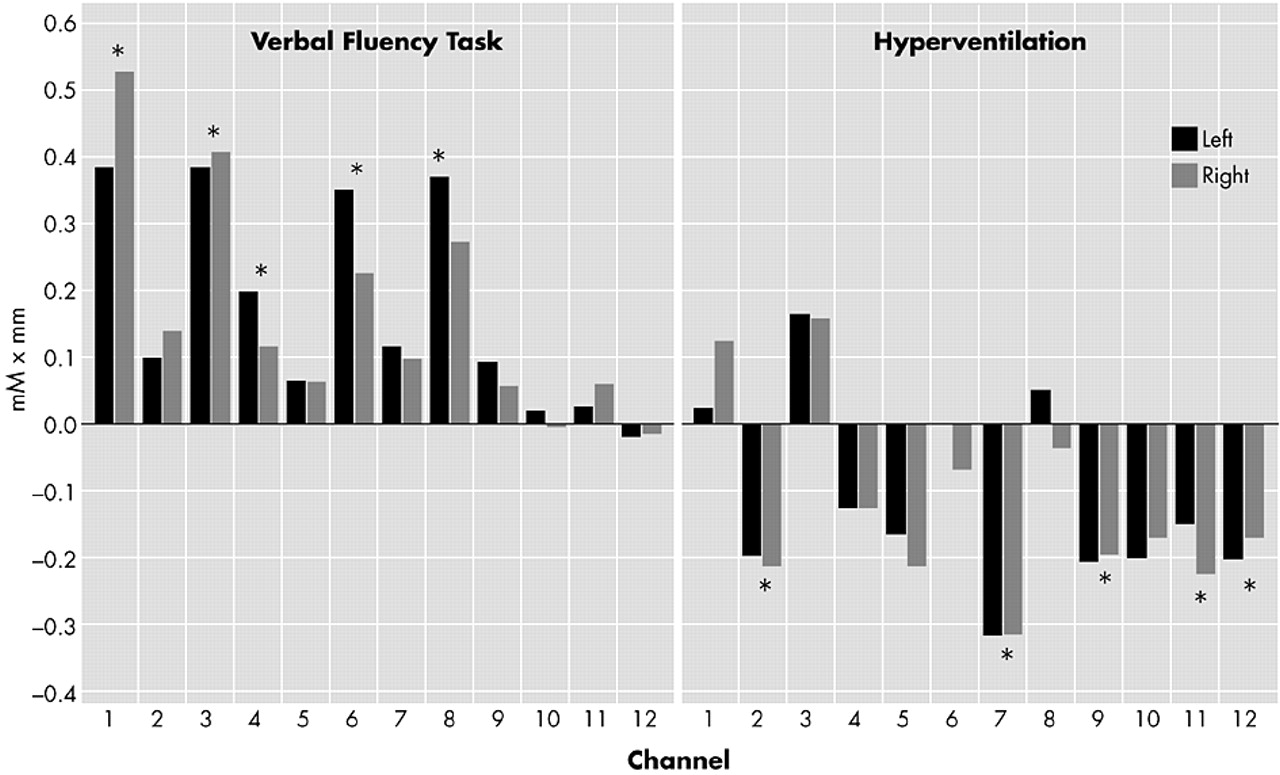
In this study, the oxyHb and totalHb increased during DF and VF and decreased during HV, and deoxyHb did not change. In addition, the test-retest reliability in DF, VF, and HV was acceptable to be used for clinical studies. This study shows that oxyHb and totalHb significantly increased mainly lateral part of the frontal lobe (channels 1, 3, 4, 6, and 8) during VF and significantly decreased mainly medial part of the frontal lobe (channels 2, 7, 9, 11, and 12) during HV. CP and WR have limitations as control tasks in that they did not match DF and VF in terms of the effort required or the speed of response.
In this study, DF and VF significantly activated the bilateral frontal lobes. Studies of neuropsychological tests in patients with focal cerebral lesions suggest that the left frontal lobe is involved in VF and the right or bilateral frontal lobe is involved in DF.
26,27 In several brain imaging studies, VF activated the left frontal lobe.
25,28,29 In another study, however, category VF activated the right frontal lobe but letter VF did not.
30 On the other hand, little information is available about DF. Elfgren and Risberg
25 reported bilateral frontal activation during DF. The region in the frontal lobe activated by VF has been controversial. In some studies, VF activated the left dorsolateral prefrontal cortex
31 or left inferior prefrontal cortex.
32 The present study suggests that VF activates lateral part of the frontal lobe, which corresponds to the dorsolateral prefrontal cortex according to our preliminary study of superposition of MRI and NIRS probes in two subjects. Further studies are necessary in order to clarify the liberalization and activated position of VF and DF.
In the present study, oxyHb and totalHb decreased during HV mainly medial part of the frontal lobe. The reason why oxyHb and totalHb did not change lateral part of the frontal lobe is unclear. Ishii et al.
33 reported that cerebral blood flow during HV decreased in general but increased in the primary motor and premotor regions. This nonuniform distribution of HV-induced change may be due to the difference in vascular distribution. For example, the prefrontal cortex mainly flows via the anterior cerebral artery, while the motor cortex flows via the middle cerebral artery.
The findings of the present study reveal that test-retest reliability was high in VF and HV and reasonable in DF and that NIRS was suitable to measure the cerebrovascular response. The possibility that cerebrovascular response differs from the strategy of the task
25 and that DF has various strategies may explain the lower reliability in DF compared with that in VF and HV.
Spontaneous oscillations were frequently observed and they influenced the test-retest reliability. These phenomena were recently observed in NIRS,
34 functional MRI
35 and transcranial doppler sonography.
36Obrig et al.
34 categorized the spontaneous oscillations into three types; low frequency oscillations (0.1 Hz), very low frequency oscillations (0.04 Hz), and high frequency oscillations (0.2–0.3 Hz). Of the three types, low frequency oscillations were attenuated by hypercapnia. These spontaneous oscillations may have been due to autoregulation of the vessel. However, the biological mechanism of the spontaneous oscillations is unclear and needs to be investigated.
The relation between cerebral neuronal activation and oxyHb, deoxyHb, and totalHb is complex. Cerebral neuronal activation causes an increase in oxyHb consumption and deoxyHb production, subsequently, cerebral vasodilatation occurs, and cerebral blood volume starts to increase. Fox and Raichle
37 reported that cerebral blood flow far exceeds the concomitant local increase in tissue metabolic rate. Therefore, the most typical response pattern of cerebral neuronal activation is an increase in oxyHb and a decrease in deoxyHb.
22 However, this is debatable since Hoshi et al.
39 reported that some healthy subjects showed a decrease in focal cerebral blood volume in the dominant frontal lobe during problem solving and mental arithmetic when NIRS and positron emission tomography were used.
There are several studies on cerebral blood volume that is measured with one- or two-channel NIRS during cognitive tasks in healthy subjects and patients with psychiatric illness.
15,20–22,38 To our knowledge, this is the first study in which the cerebrovascular responses during both cognitive tasks and HV were evaluated using multi-channel NIRS. This method can be applied to clinical studies in neuropsychiatric disorders, including affective disorders and schizophrenia, to assess cerebrovascular response to cognitive activations and physiological stimulation such as HV.