At this point, we still do not have a uniform definition of psychosis in PD or a universally accepted rating scale to gauge treatment response. In the PD literature, the term psychosis has been used to describe different behaviors by different authors. This lack of uniform classification is bound to generate controversy in the interpretation of study outcomes. There are some aspects of psychosis in PD that are universally accepted among those caring for patients with this illness. For example, unlike auditory hallucinations that are seen in primary psychiatric disorders (e.g. schizophrenia), the hallucinations in PD-associated psychosis are mainly visual. Other aspects of PD psychosis are subject to debate. For example, some would consider vivid dreams an early manifestation of psychosis whereas others would not.
In this article, we raise and begin to answer some fundamental questions regarding psychosis in PD. We conducted Medline searches using terms such as Parkinson’s disease and psychosis, then chose relevant articles from the references of our initial search. Subsequently, we reviewed literature related to some other conditions (e.g. DLB, sleep disorders) as their importance to the understanding of PD psychosis became evident. We review and integrate data obtained and theories proposed by others with our own experience. Based on this synthesis, we propose (where relevant) approaches to clinical care and future research. We focus on the following issues related to psychosis in PD: 1) prevalence, 2) possible etiologies and risk factors and 3) treatment.
WHAT IS THE PREVALENCE OF PSYCHOSIS IN PD?
Prevalence estimates of psychosis in PD have ranged from 3% for delusions
4 to 30% for visual hallucinations.
5–7 These rates are higher (5–62%) in studies that have included unselected parkinsonian patients with varied “psychotic phenomena” such as agitated confusion, reversible psychosis, and hallucinosis in addition to hallucinations and delusions.
5,8,9In prevalence studies, few authors have stratified their samples based on psychopathology, comorbid diagnoses, or types of medications. In a review of psychiatric side effects in 908 patients receiving levodopa, Goodwin found rates of 3.6% for both agitation and for psychosis.
10 Another review reported that the prevalence of visual hallucinations (in the context of a clear sensorium) in PD patients receiving chronic antiparkinsonian therapy ranged from 9–32%.
11 A recent prospective study evaluated prevalence of visual hallucinations in patients with PD. In this study of 98 patients, 26 had visual hallucinations. Among these, one patient also had delusions and two had auditory hallucinations.
12 Another study
6 attempted to stratify patients based on severity of psychosis using the Unified Parkinson’s Disease Rating Scale (UPDRS).
13 Among 235 patients from the community, 24% of patients had vivid dreams believed to represent early stages of perceptual and thought disturbance, 10% had hallucinations with retained insight, and 6% had severe, persistent hallucinations without insight and/or delusions. The authors had excluded patients with previous histories of psychosis, but not those with dementia or depression.
A study
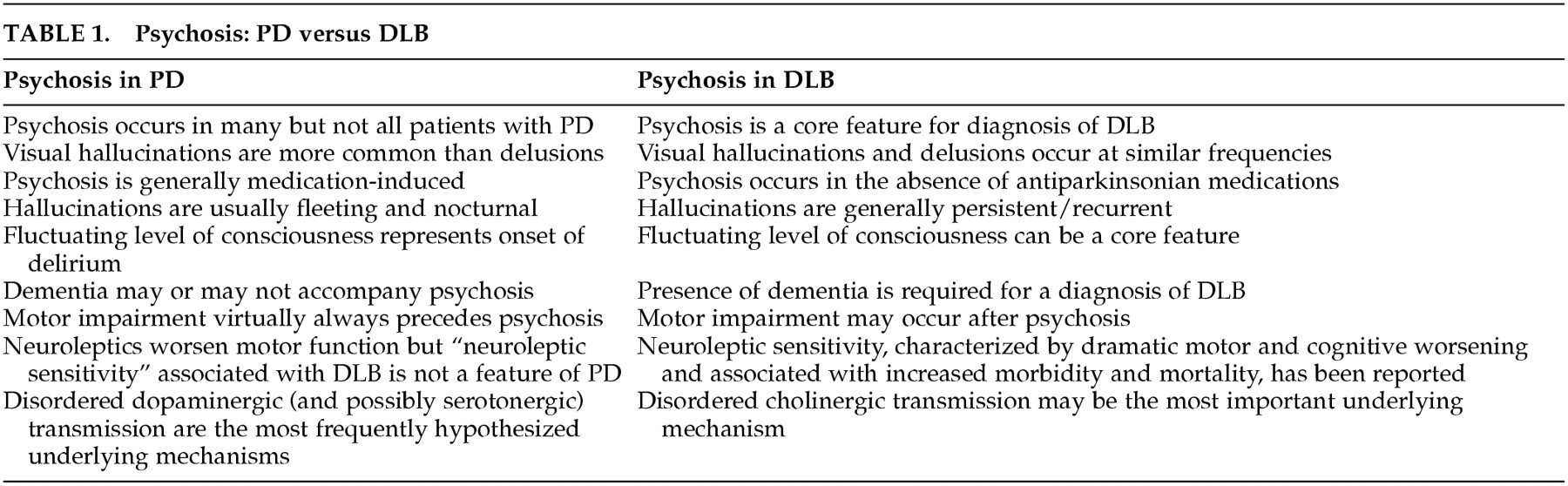
14 of 172 consecutive patients with 5-year histories of PD demonstrated a psychosis prevalence rate of 27%. In this case, the authors specifically excluded patients who developed dementia within one year of motor impairment and those in whom dementia predated the onset of motor symptoms, thereby making the inclusion of patients who had Dementia with Lewy bodies (DLB) less likely. This is important since the clinical similarities between patients who have PD complicated by dementia and psychosis and those with DLB can sometimes make diagnosis difficult. Various criteria have been proposed for DLB, in response to ongoing controversies.
15,16 In practice, DLB is part of the differential diagnosis of Alzheimer's disease (AD) when the initial symptoms are cognitive and of PD when the initial symptoms are motor. Based on our review of the literature and our own experiences we have summarized some distinctions between psychosis in PD and DLB in
Table 1.
17,18In summary, it is difficult to establish precise prevalence rates for “psychosis” in PD, given the varying interpretations of this term among investigators conducting studies thus far. Suffice it to say that studies to date support the notion that hallucinations are significantly more common than delusions and that psychotic phenomenon occur in at least 20% of medication-treated PD patients. Developing and implementing uniform diagnostic criteria (that are careful to exclude patients with DLB as best we can) will help us achieve a more accurate estimate of prevalence.
WHAT ARE THE POSSIBLE ETIOLOGIES AND RISK FACTORS FOR PSYCHOSIS IN PD?
The etiological basis of psychosis in PD remains an unsettled issue. Although there is some controversial evidence that psychosis was observed in PD patients before the advent of levodopa therapy,
19,20 it is generally accepted that psychosis in PD is a drug-induced phenomenon. Many clinicians and researchers (including ourselves) believe that diagnoses other than idiopathic PD (e.g. DLB) should be considered in patients who develop psychosis early in the treatment with medications or those who develop psychosis without the use of implicated medications.
21,22However, the precise relationship between dopaminergic medications and psychosis has not been clearly delineated. The dose and duration of dopaminergic therapy are not considered consistent risk factors for hallucinations. Goetz et al.
23 studied PD patients with a history of chronic hallucinations, noting that intravenous infusions of high-dose levodopa did not precipitate hallucinations. These observations suggest that the dopaminergic system is involved in the pathophysiologic process of hallucinations in PD, but that hallucinations themselves are not directly related to plasma (and presumably brain) levodopa levels.
The mechanisms that underlie PD psychosis remain to be determined. The most frequently proposed hypothesis is that, in some patients, denervation hypersensitivity of mesolimbic and mesocortical dopamine receptors may occur and that dopaminergic medications may stimulate these receptors to cause psychosis.
9,24More recently, it has been hypothesized that a combination or combinations of neurotransmitter systems play a role in the development of PD psychosis. Birkmayer and Riederer
25 have suggested that a serotonergic/dopaminergic imbalance may be most important. In support of this notion are postmortem studies revealing variable degrees and distributions of serotonin loss among patients with PD
26 and reports that pharmacological agents that exert their effects on serotonin receptors (e.g., atypical antipsychotics, ondansetron) appear to have some efficacy against PD-related visual hallucinations.
27,28Although deficiencies in cholinergic transmission are linked more closely to AD, there has been some suggestion that the ratio of serotonin to acetylcholine may be important for the development of psychosis in DLB.
29,30 Profound depletion of cholinergic markers and relative preservation of serotonergic markers in the temporal or parietal cortex have been suggested as a possible neurochemical explanation for psychosis in DLB.
29 This would be in keeping with the finding that acetylcholinesterase inhibitors might have some antipsychotic efficacy in these illnesses. Whether or not this is relevant to patients with PD and drug-induced psychosis remains to be determined.
An important question is why, when exposed to the same dopaminergic medications, do some PD patients develop psychosis while others do not? Based on established links in AD between psychosis and dopamine receptor genetic variants and APOE alleles, Goetz et al
31 conducted a case-control study in PD patients with and without visual hallucinations. They determined, however, that visual hallucinations in PD are not associated with the genetic pattern seen for patients with AD and psychosis. The authors noted that comparison of serotonergic receptor polymorphisms in cases and controls remains an area for future research.
Whether or not specific antiparkinsonian agents are associated with different degrees or forms of psychosis is not clear. Some have reported that patients being treated with anticholinergics are likely to present with confusion and that hallucinations in these cases are less formed than with dopaminergic-induced psychosis.
5,32 A recent 5-year study comparing the incidence of dyskinesia in PD patients treated with the dopamine agonist ropinirole or levodopa
33 revealed that the incidence of hallucinations was higher in the ropinirole group (17% versus 6%). Similarly, dopamine agonist bromocriptine treatment was associated with more hallucinations
34 in an open-label randomized trial comparing bromocriptine with the catechol-o-methyl-transferase (COMT) inhibitor tolcapone. In a smaller study involving 40 PD patients
35 a switch from tolcapone as an adjunctive therapy to another COMT-inhibitor (entacapone) failed in 6 patients due to increase in dyskinesia and hallucinations.
Thus, it appears that while all antiparkinsonian medications may play a role in PD psychosis, some classes of medications (e.g., dopamine agonists) may do so more often. Additionally, clinicians need to consider the fact that many patients use other offending agents to control associated conditions (e.g., anticholinergic agents for bladder dysfunction).
Proposed risk factors for the development of psychosis in PD have included age, stage and severity of PD, depression, sleep disturbances, and cognitive impairment.
6,12,14Among the proposed risk factor for psychosis in PD, dementia emerges in the majority of studies.
6,7,36 The precise relationship between dementia and psychosis is not clear. Does cognitive impairment contribute to symptoms of psychosis? (e.g., Do memory disturbances lead demented patients to believe that someone must have “stolen” from them?). Do dementia and psychosis stem from similar neuropathological and pathophysiological disease states, rendering the same patients vulnerable to both? (e.g. combined deficiencies of dopamine and acetylcholine, extension of Lewy body pathology beyond the brainstem).
Studies exploring the relationship between cognition and psychosis in similar neurodegenerative disorders (e.g. DLB) may help us understand the relationship between cognitive impairment and psychosis in PD.
29,37 In a recent study
37 neuropsychiatric symptoms were assessed in PD patients with dementia (PDD), PD patients without dementia (PDND) and in those with DLB (confirmed by autopsy in one-third). Delusions and hallucinations occurred with increasing frequency in PDND (7% and 14%), PDD (29% and 54%), and DLB (57% and 76%). The types of hallucinations and delusions were similar across the three groups. The authors commented that these findings add support to the hypothesis that psychiatric symptoms may be associated with cortical Lewy bodies or cholinergic deficits in both PD and DLB.
Our ability to understand the relationship between psychosis and dementia in patients with PD is further complicated by the relationship between dementia and delirium. Advanced age, pre-existing dementia and “organic brain disease” are all risk factors for delirium
38,39 with up to 40% of delirious patients having dementia.
40 It has been estimated that hallucinations occur in 30–77% of patients with delirium.
41 We suggest that psychosis occurring in demented PD patients during delirium (“confusional psychosis”) may be different (both in pathophysiology and approach to treatment) than psychosis occurring in cognitively intact PD patients in the setting of a clear sensorium.
There appears to be a strong relationship between sleep disturbances and psychosis in PD. Whether sleep disturbances are a risk factor for psychosis in PD or if sleep disturbances represent one end of the “psychosis spectrum” in PD continues to be debated.
Moskovitz et al.
9 applied the model of pharmacological kindling in an attempt to understand progressively abnormal behavioral alterations in patients receiving levodopa therapy for PD. In their sample of 88 PD patients, all psychotic states were associated with preexistent or concurrent vivid dreams and/or hallucinations. In another study,
42 the majority of patients who had psychiatric side effects from levodopa also had sleep disturbances in the form of excessive daytime sleepiness, parasomnias (e.g., sleep walking, sleep talking) and nocturnal myoclonus. Among patients with sleep alteration, 39% were hallucinating compared to only 4% who did not have sleep disruption.
Although many forms of sleep disturbances are described in PD, rapid-eye movement (REM)-related sleep disorders appear most closely related to psychosis. Altered dream activity in PD patients can include vivid dreams, nightmares and other REM behavior disorders, such as nocturnal vocalization and movements.
43 Several lines of evidence suggest a fundamental link between the processes underlying REM sleep disturbances and those responsible for psychosis in PD. Reduced REM sleep is observed more often in patients who hallucinate than in those who do not.
44 Some have suggested that psychosis in PD may reflect a narcolepsy-like REM sleep disorder.
45 In one study, polysomnographic (PSG) recordings were obtained on 20 patients with PD (half experienced levodopa-induced hallucinations and half did not). The patients with a history of hallucinations had narcolepsy-like REM sleep episodes that coincided with hallucinations during the day and post-REM delusions at night.
In summary, psychosis in PD appears to be a drug-induced phenomenon. Antiparkinsonian medications alone, however, are not sufficient to cause psychosis (given the fact that only some medicated PD patients develop psychosis). There are likely to be neuropathological and pathophysiological differences among patients that result in the development of psychosis in some but not others. Supersensivity of mesolimbic and mesocortical dopaminergic systems are likely to be involved but nondopaminergic systems (and serotonin in particular) are probably important as well. Further elucidation of the close relationships between psychosis and what are currently viewed as its biggest risk factors (dementia and sleep disorders) may provide insights into underlying mechanisms.
CONCLUSION
Psychosis in PD affects at least 20% of medicated patients and appears to be due to an interaction between PD-related pathophysiology and dopaminergic medications. Visual hallucinations are the most frequent form of psychosis in PD but delusions are not uncommon. Psychosis can occur in the setting of a clear or clouded sensorium. Classification of psychotic behavior is difficult within the constructs currently available. Further research to define diagnostic criteria for psychosis and its course and treatment outcomes in PD is needed.
The frequent coexistence of parkinsonism, dementia, and psychosis can make diagnosis difficult, and it is important to consider DLB in the differential diagnosis. The relative time of onset of motor and cognitive features may help with diagnosis. The nature of the psychosis and whether or not it was provoked by antiparkinsonian medications may also provide clues. However, it should be noted that the lines dividing these neurodegenerative conditions can prove indistinct, both from the clinical and pathological perspectives.
It has been hypothesized that, in some patients, denervation hypersensitivity of mesolimbic dopamine receptors may occur and that dopaminergic medications may stimulate these hypersensitive receptors to cause psychosis. The exact neurochemical link to the dopaminergic system, however, is not clearly delineated and the interplay among several neurotransmitters (including serotonin and acetylcholine) may be important. Proposed risk factors for the development of psychosis in PD have included age, stage and severity of PD, depression, sleep disturbances, and cognitive impairment,
8,14,16 with the last two emerging as the strongest ones.
The availability of atypical antipsychotic medications such as clozapine, that can reduce psychosis while preserving motor function, have launched us into a new era of treatment for psychosis in PD. We await the results of well-controlled clinical trials involving other potential antipsychotic agents. The fact that effective treatments for psychosis in PD are now becoming a “reality” may “test” our resolve to genuinely understand this complex phenomenon. Further exploration of psychosis in PD may enable us to develop more focused approaches to its treatment and perhaps its prevention. In addition, by furthering our understanding of PD psychosis, we will undoubtedly learn more about other aspects of PD (e.g., dementia), related neurodegenerative diseases, (e.g. DLB) and primary psychotic disorders (e.g., schizophrenia).