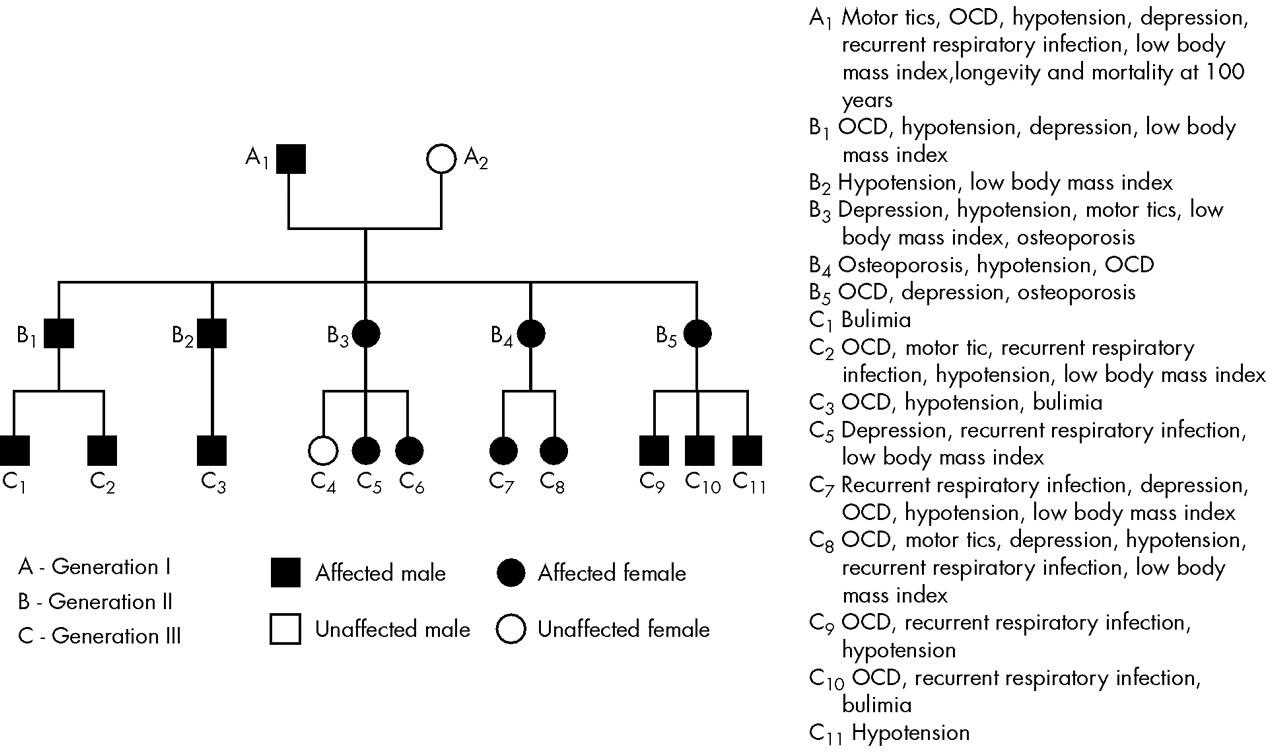
A family with coexistent hypotension, recurrent respiratory infection owing to immune deficiency, motor tics, obsessive-compulsive disorder, major depressive disorder, early onset osteoporosis, low body mass index, bulimia nervosa, and healthy aging is described. The family members had the following behavioral patterns: hyposexual, nonspiritual, noncreative, somnolent tendency, increased bonding and affectionate behavior and nonaddictive tendency. All members in the family were right-handed left hemispheric dominant. The human hypothalamus synthesizes an endogenous membrane Na
+K
+ ATPase inhibitor: digoxin. This has been extensively documented in the literature.
1,2,3,4,5 Structurally, digoxin is a steroidal glycoside and is synthesized in the human hypothalamus by the isoprenoid pathway.
3,4,5 From our laboratory,
14C labeled acetate studies have demonstrated that endogenous digoxin is synthesized by the isoprenoid pathway. Alteration in the endogenous membrane Na
+K
+ ATPase inhibitor, digoxin has been documented in depression, essential hypertension, and syndrome X.
1,2 Digoxin can function as a modulator of synaptic transmission in multiple neurotransmitter systems.
4 Digoxin and alterations in membrane Na
+K
+ ATPase activity can modify intracellular calcium/magnesium ratios and may also function as a immunomodulator.
3 Therefore, it was hypothesized that endogenous digoxin would play a role in the pathogenesis of the disorders described in the indexed family (e.g, hypotension, major depressive disorder, osteoporosis, recurrent respiratory infection, low body mass index). Other isoprenoidal metabolites of significance are ubiquinone (regulate mitochondrial function), cholesterol (component of cellular membranes), and dolichol (regulate N-glycosylation of proteins). The isoprenoidal pathway, glycoconjugate metabolism, neurotransmitter patterns, free radical metabolism, and membrane composition were studied in the indexed family. Glycoconjugates, sialoligands and fucoligands are involved in immunomodulation and function as acute phase reactants in infections. Free radicals mediate the phagocytic killing of bacteria and viruses. They could, therefore, be of significance in the pathogenesis of recurrent respiratory infection. Digoxin can modulate the neutral amino acid-tryptophan/tyrosine transport, and hence regulate their cellular metabolism. Tryptophan and tyrosine catabolic patterns were studied in order to delineate the neurotransmitter patterns involved in the psychiatric/psychological disorders in the family, as clinical treatment of these disorders is dependent on modulation of neurotransmitter function. Alterations in neuronal membrane structure/function have been described in depressive illness and drugs such as lithium, which is used to treat bipolar mood disorder and can alter membrane function. The isoprenoid pathway metabolites, ubiquinone and dolichol, can regulate membrane composition and structure. Red blood cell membrane composition was studied as a marker for such parameters. Since digoxin and changes in membrane Na
+K
+ ATPase activity was the only common possible etiopathogenetic factor underlining hypotension, major depressive disorder, osteoporosis and recurrent infection, alteration in the digoxin status, and the isoprenoid pathway cascade were hypothesized as the primary dysfunctions in the family. Thus, the data on digoxin status and isoprenoid pathway related cascade, as well as possible modulation of both biochemical parameters, are of clinical significance in the treatment of the disorders noted in the indexed family. Since digoxin can regulate synaptic transmission in multiple neurotransmitter systems and, possibly, hemispheric dominance, the isoprenoid pathway was also compared in right hemispheric and left hemispheric dominance in order to find whether hemispheric dominance plays a role in the genesis of the disorder.
MATERIALS and METHODS
The indexed family was studied over three generations for motor tics, obsessive-compulsive disorder (OCD), major depressive disorder, bulimia nervosa, recurrent respiratory infections, early-onset osteoporosis, hypotension, and low body mass index. OCD, major depressive disorder, and bulimia nervosa were diagnosed by the DSM-IV criteria. Recurrent respiratory infections were diagnosed when there were more than 3 significant respiratory infections in 1 month that warranted treatment. Low body mass index was defined as a body mass index less than 18.5 kg/m
2. The family members were screened for the following behavioral patterns: 1) the criteria given in the handbook for the 16 PF—16 personality factors questionnaire was chosen after modification for defining spirituality, creativity, and bonding/affection
6 and 2) the criteria for insomnia and somnolence, sexual behavior, addiction, and eating behavior were chosen from the DSM IV criteria. All of the 15 living, affected members of the indexed family were chosen for the study except one (A
1), who died. Each patient also had an age and sex matched right-handed/left hemispheric dominant control. Additionally, 15 normal, left-handed individuals between 20 to 30 years of age, who were right hemisphere dominant, and 15 right-handed individual between 20 to 30 years of age, who were left hemisphere dominant, were chosen by the dichotic listening test and for comparison of the same parameters. Informed consent was obtained from all patients. Each patient and control subject was nonsmoking (passive or active), and they were all free from consumption of addictive drugs such morphine. Detailed history taking and interviews were conducted to rule out morphine/opiate usage. The blood samples were collected from the patients before starting treatment. Biochemicals used in this study were obtained from M/s.Sigma Chemicals, USA. Activity of HMG-CoA reductase of the plasma was assayed using the method of Rao and Ramakrishnan in determining the ratio of HMG CoA to mevalonate.
7 The procedure described by Wallach and Kamat was used to determine the RBC Na
+K
+ ATPase activity of the erythrocytre membrane.
8 Digoxin in the plasma was assayed using the procedure described by Arun et al.
9. For estimation of ubiquinone and dolichol in the plasma, the procedure described by Palmer et al. was employed.
10 Magnesium in the plasma was estimated by atomic absorption.
11 Tryptophan, tyrosine, serotonin, and catecholamines were estimated by the procedures described in Methods of Biochemical Analysis.
12 Quinolinic acid content of plasma was estimated by HPLC (C
18 column micro Bondapak™ 4.6 × 150mm), solvent system 0.01 M acetate buffer (pH 3.0) and methanol (6:4), flow rate 1.0 ml/minute and detection UV 250 nm). Morphine, strychnine, and nicotine were determined by the method described by Arun et al.
13. Details of the procedures used for the estimation of total and individual GAG fractions, carbohydrate components of glycoproteins, activity of GAG degrading enzymes, and glycohydrolases were previously described.
14 Serum glycolipids were estimated by utilizing the procedure presented in
Methods in Enzymology.8 Cholesterol was assessed using commercial kits supplied by Sigma Chemicals, USA. Superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase were determined by the procedures described in
Methods of Enzymatic Analysis.15 Malondialdehyde (MDA), conjugated dienes, hydroperoxides, and reduced glutathione, iron binding capacity, and ceruloplasmin were assayed using procedures described in
Methods of Biochemical Analysis.12 Nitric oxide was estimated in the plasma by the method of Gabor and Allon.
16 Statistical analysis was conducted by Students t test with modified degrees of freedom.
DISCUSSION
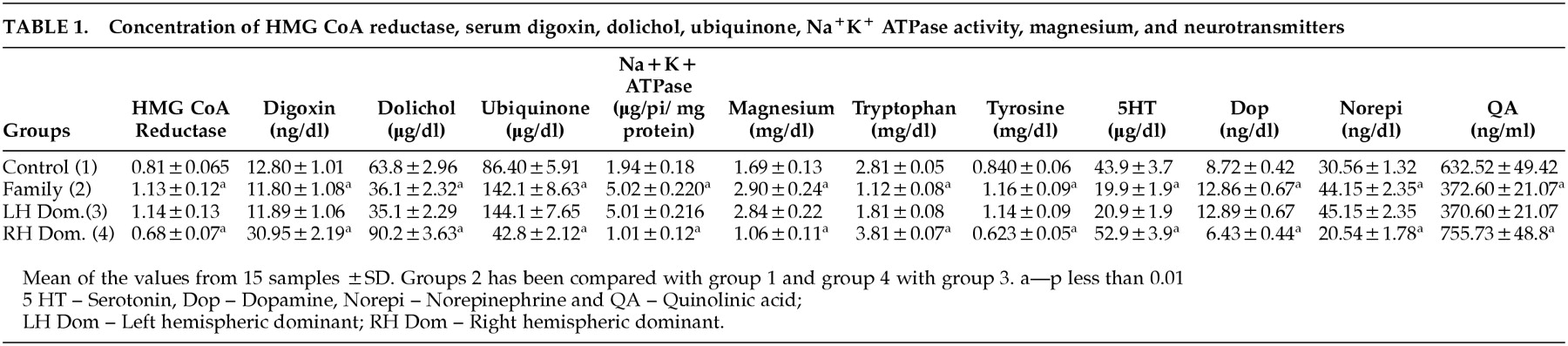
The decrease in the activity of HMG-CoA reductase in familial cases suggests a downregulation of the isoprenoid pathway. There is a marked decrease in plasma digoxin and dolichol, and this decrease may be a consequence of decreased channelling of intermediates of the isoprenoid pathway for their biosynthesis. The decrease in endogenous digoxin, a potent inhibitor of membrane Na
+K
+ ATPase, can increase this enzyme activity. The stimulation of Na
+K
+ ATPase by digoxin is known to cause a decrease in intracellular calcium and an increase in intracellular magnesium.
17 Serum magnesium was assessed in familial cases and was found to be increased. Decrease in bone calcium load can lead to osteoporosis. The results showed that the concentration of tryptophan, quinolinic acid, serotonin, strychnine, and nicotine was found to be lower in the plasma of patients with familial cases while that of tyrosine, dopamine, norepinephrine, and morphine was higher. Nicotine and strychnine are synthesised from tryptophan and morphine from tyrosine.
13,18 Thus, there is a decrease in tryptophan and its catabolites and increase in tyrosine and its catabolites in the patients' serum. This could be due to the fact digoxin can regulate neutral aminoacid transport system with a preferential promotion of tryptophan transport over tyrosine and that digoxin levels are low in familial cases.
4 The increase in membrane Na
+K
+ ATPase activity in familial cases could be due to the fact that the hyperpolarising neurotransmitters (dopamine, morphine, and noradrenaline) are increased and the depolarising neuroactive compounds (serotonin, strychnine, nicotine, and quinolinic acid are decreased. The low level of quinolinic acid, serotonin and strychnine can contribute to reduced excitatory glutamatergic transmission as they are all positive modulators of the N-methyl-D-aspartate (NMDA) receptor.
19 In the presence of hypermagnesemia, the magnesium block on the NMDA receptor is strengthened leading to reduced NMDA transmission.
19 Reduced glutamatergic transmission can lead to healthy aging and protect the brain from neuronal degeneration.
19 The depressive syndrome noted in the family could be due to low serotonin. Decreased serotoninergic transmission has been related to depression. The presence of OCD syndrome in the family could also be related to serotonin depletion.
20 Serotonin depletion has been related to obsessive psychopathology. The presence of motor tics could be related to increased dopaminergic transmission in the brain.
20 Deficiency of serotonin may lead to increased appetite and eating behavior with bulimia in the family members.
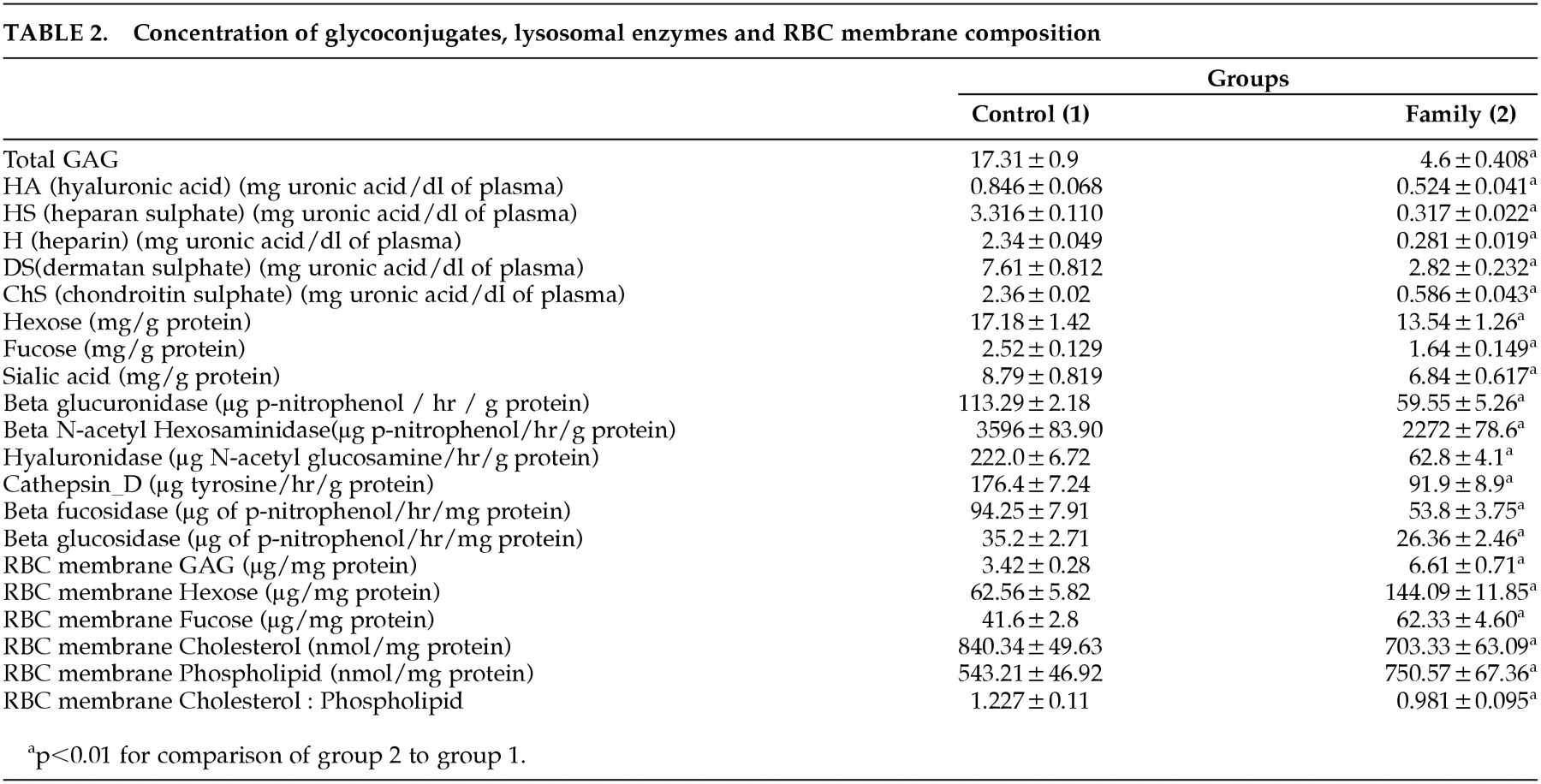
20Hypermagnesemia and decreased dolichol (required for N-glycosylation) levels can inhibit GAG and glycoprotein biosynthesis.
21 The activity of GAG degrading enzymes and glycohydrolases decreased in the serum suggesting increased lysosomal stability. Intracellular hypermagnesemia also results in increased ubiquitin dependent proteolytic processing of glycoconjugates, as it requires magnesium for its function. Defective/reduced lysosomal stability and defective degradation of glycoprotein—GAG complexes as in the case of tau protein / amyloid—HS proteoglycan complexes in Alzheimer’s Disease can lead to brain aging.
22 Membrane Na
+K
+ ATPase stimulation could, therefore, protect against neuronal aging and degeneration. A number of fucose and sialic acid containing natural ligands have been implicated in inflammatory responses and neoplastic transformation.
23 The decrease in fucose and sialic acid noted in these cases could result in an immunosuppressive state, with recurrent respiratory infection and prevent malignant transformation. Decrease in bone structural glycosaminoglycans could contribute to osteoporosis. The downregulation of isoprenoid pathway may result in decreased cholesterol synthesis and magnesium excess can stimulate phospholipid synthesis leading on to a decreased membrane cholesterol: phospholipid ratio. The concentration of total GAG and carbohydrate residues of glycoprotein increased in the RBC membrane and decreased in the serum suggesting their increased incorporation into the membrane. Hypermagnesemia can stimulate the activity of membrane trafficking enzymes—GTPases and lipid kinases. The change in membrane structure produced by alteration in glycoconjugates and cholesterol: phospholipid ratio can produce changes in the conformation of Na
+K
+ ATPase, leading to further membrane Na
+K
+ ATPase stimulation. The same changes can affect the lysosomal membrane increasing its stability.
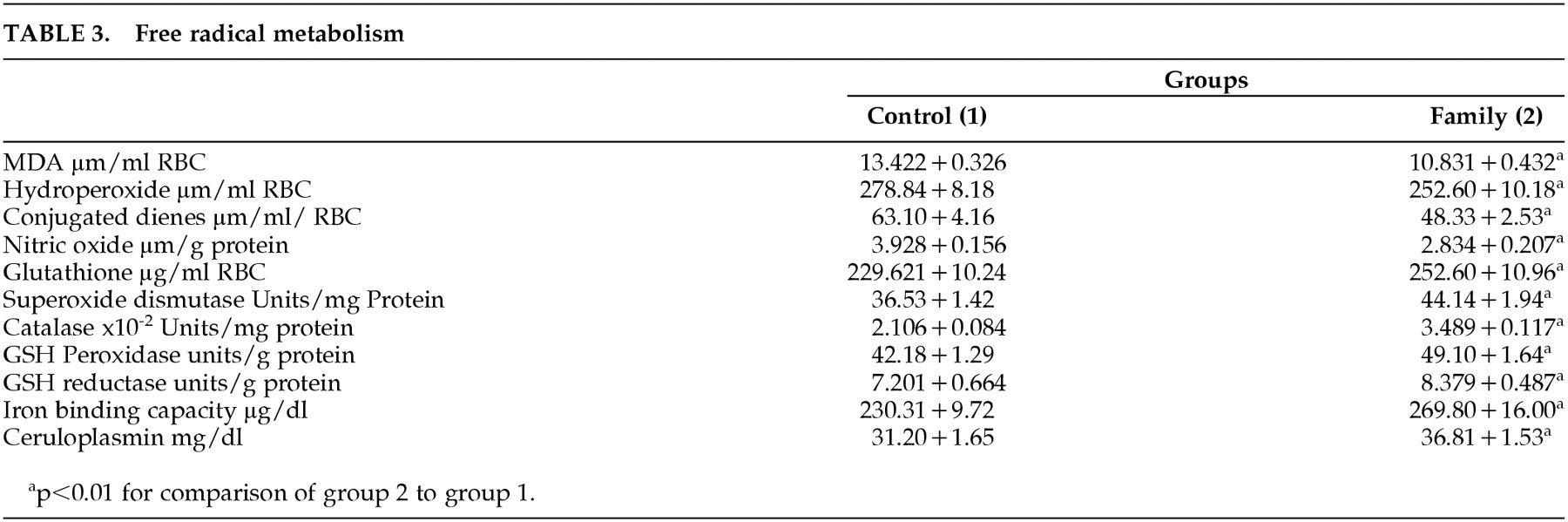
The concentration of ubiquinone (free radical scavenger and component of mitochondrial electron transport chain) increased significantly in familial cases, which may be the result of increased tyrosine levels, consequent to digoxin deficiency promoting tyrosine transport over tryptophan.
4 The aromatic ring portion of ubiquinone is derived from tyrosine. The decrease in intracellular calcium can stabilise the mitochondrial permeability transmission (PT) pore and improve mitochondrial function.
24 Intracellular hypermagnesemia can lead to increased ATP synthase activity. All this leads to improved efficiency of mitochondrial oxidative phosphorylation and reduced free radical generation. Decreased intracellular calcium also results in decreased generation of NO by inhibiting the enzyme nitric oxide synthase and reduced peroxynitrite formation. The free radical scavenging enzyme activity, the concentration of antioxidants (ubiquinone, reduced glutathione, ceruloplasmin), and iron binding capacity increased significantly in familial cases suggesting increased free radical scavenging. The peroxisomal membrane is stabilised owing to membrane Na
+K
+ ATPase stimulation related upregulation in membrane formation and leads to increased catalase activity. Hypermagnesemia leads to increased glutathione synthetase, glutathione peroxidase, and glutathione reductase function. The stabilisation of the mitochondrial PT pore consequent to reduced intracellular calcium produces increased efficiency of superoxide dismutase activity. Mitochondrial dysfunction related free radical generation has been implicated in the pathogenesis of neuronal degeneration such as PD, oncogenesis, and inflammatory diseases. The reduced generation of free radicals leads to decreased incidence of neuronal degeneration and oncogenesis in the index family. Free radicals are required for lymphocyte activation and this leads to a hypoimmune response and increased respiratory infection owing to immunodeficiency. The decreased intracellular calcium and ceramide-related stabilization of the mitochondrial PT pore inhibits cytochrome C release and the caspase cascade.
24 Apoptosis has been implicated in neuronal degeneration, and its inhibition protects against neuronal aging.
There is a decreased oncogenic tendency in the indexed family. Decreased intracellular calcium inactivates phospholipase C beta, which results in decreased production of diacyglycerol (DAG) with resultant inactivation of protein kinase C and the MAP kinase cascade.
25 The intracellular hypermagnesemia can produce increase in the GTPase activity of the alpha-subunit of G protein resulting in ras-oncogene inactivation, as more of the ras is bound to GDP rather than GTP. Tumour suppressor gene P
53 activation is increased due to intracellular hypermagnesemia producing greater phosphorylation.
25 Decreased intracellular calcium inactivates the calcium dependent calcineurin signal transduction pathway involved in T cell activation and reduces the secretion of Interleukin 3, 4, 5, 6 and TNF alpha.
26 TNF alpha can also bring about apoptosis of the cell and this is inhibited. TNF alpha binds to its receptor TNFRI and activates the transcription factors NF-kB and AP-1 leading to induction of proinflammatory and immunomodulatory genes.
24 Low levels of TNF alpha can lead to immunosuppression in the family.
Hypermagnesemia can upregulate glucose transport as magnesium is required as a co-factor for cell membrane glucose transport. Intracellular hypermagnesemia can activate the phosphorylation reactions involved in protein tyrosine kinase receptor activity leading to increased insulin receptor activity. Intracellular hypermagnesemia can lead to stimulation of glycolysis. Decreases in intracellular calcium can stabilize the mitochondrial PT pore and stimulate mitochondrial oxidative phosphorylation. Intracellular hypermagnesemia can also lead to a ATP synthase hyperactivity. This leads to increased glucose utilisation. Decreases in beta cell calcium and increase in magnesium may contribute to decreased insulin release from beta cells and hypoinsulinemia. Increased intracellular magnesium can produce hyperactivity of lipoprotein lipase producing increased catabolism of triglycerides rich lipoproteins and hypotriglyceridemia. In hypermagnesemia, Lecithin cholesterol acyl transferase (LCAT) is increased, and there is increased formation of cholesterol esters in HDL. This results in increased HDL cholesterol. Magnesium excess has been reported to decrease LDL cholesterol levels also. Low insulin levels and increased triglyceride catabolism can be correlated with low body mass index noted in the family. Decreases in intracellular calcium can inactivate G-protein coupled angiotensin receptor producing hypotension and G protein coupled thrombin receptor and platelet activating factor producing decreased thrombosis observed in the family. Increased intracellular magnesium can lead to decreased thrombin and ADP/collagen induced platelet aggregation. Na
+K
+ ATPase stimulation related decreased smooth muscle calcium and increased magnesium can contribute to vasodilatation and protect the family from ischaemia due to stroke and CAD. The family has a endogenous morphine excess syndrome. Morphine has been reported to have an effect on glucose metabolism.
18 Intrathecal administration of morphine in the lumbar region causes a dose-dependent hypoglycemia. In addition to having an immunosuppressive action, morphine may also regulate insulin release from the beta cells with an inhibitory effect reported in some cases. This could contribute to increased incidence of respiratory infections. Morphine excess may also lead to the lack of addiction, which has been noticed in the family membrane.
18The biochemical pattern obtained in the family correlated with the left hemispheric dominant state. In the left hemispheric dominant state, there is a downregulated isoprenoid pathway, hypodigoxinemia, membrane Na+K+ ATPase stimulation, decreased dolichol synthesis, and elevated ubiquinone synthesis. There is an upregulated morphinergic, dopaminergic and noradrenergic transmission with a downregulated glutamatergic, cholinergic/nicotinic, and serotoninergic transmission. There are no previous reports on a hypodigoxinemic syndrome or studies on biochemical differences between right and left hemispheric dominance in the literature.
Thus, digoxin can function as a modulator of synaptic transmission in multiple neurotransmitter systems. Diogoxin may also alter intracellular calcium/magnesium ratios and function as an immunomodulator. Endogenous digoxin deficiency plays a crucial role in the pathogenesis of the disorders described in the indexed family—hypotension, major depressive disorder, osteoporosis, recurrent respiratory infection, and low body mass index. Glycoconjugates, sialoligands and fucoligands are involved in immunomodulation and function as acute phase reactants in infections. Free radicals mediate the phagocytic killing of bacteria and viruses. Decrease in levels of fucoligands/sialoligands and free radicals therefore are significant in the pathogenesis of the immunodeficient state leading to recurrent respiratory infection. The finding of digoxin deficiency mediated upregulated tyrosine catabolism and down regulated tryptophan catabolism is important in the pathogenesis as well as useful in the clinical treatment of psychiatric/psychological disorders in the family by modulating neurotransmitter function. The changes in RBC membrane structure/function reflects changes in the neuronal membrane. Since digoxin deficiency and membrane Na+K+ ATPase stimulation was the only common etiopathogenetic factor underlining hypotension, major depressive disorders, osteoporosis and recurrent infection, alteration in the digoxin status, and the isoprenoid pathway cascade are determined as primary dysfunctions in the indexed family. Thus, data on digoxin status and isoprenoid pathway related cascade, as well as possible modulation of both biochemical parameters, are of clinical significance in the treatment of the disorders noted in the indexed family. The clinical treatment of these disorders would involve possibly inhibiting membrane Na+K+ ATPase activity by using exogenous digoxin or lithium. Membrane Na+K+ ATPase inhibition would correct all the abnormalities in the isoprenoid pathway cascade. Intracellular calcium depletion and magnesium excess is important in the pathogenesis of these disorders. Calcium supplementation would play a role in the treatment. Treatment with drugs upregulating serotoninergic and glutamatergic transmission would also be of benefit in the treatment of these psychiatric/psychological states noted in the indexed family. The data are also useful in planning treatment strategies for osteoporosis. This would involve supplementation with the glycosaminoglycan fractions, which are low in the indexed family. Digoxin, lithium, serotoninenergic/glutamatergic drugs, and glycoconjugates are already used to treat medical and psychiatric disorders. Clinical trials on this pharmacological basis are already in progress.