C atatonia is a movement disorder defined primarily by a cluster of symptoms, including immobility, mutism, and withdrawal or refusal of food and water,
1 and its presence can lead to rapid medical decompensation necessitating rapid and effective treatment for this condition. Catatonia may arise from low GABA-A receptor binding, dopamine hypoactivity, and possibly glutamate (NMDA receptor) hyperactivity.
2 It is a common neuropsychiatric syndrome that can occur in schizophrenia, bipolar disorder, major depression and general medical illnesses.
3 In a recent study, van der Heijden et al.
4 highlighted that catatonia was diagnosed clinically in only 1.3% of acute psychiatric inpatients. However, closer scrutiny showed that 18% exhibited two or more catatonic signs, emphasizing the frequent underdiagnosis of catatonia in routine clinical settings.
4 Northoff et al.
5 noted marked similarities between catatonia and the akinesia demonstrated by Parkinson’s disease patients, which often improves with the addition of amantadine to the drug regimen. The resolution of catatonia with amantadine would imply glutamatergic hyperactivity; however, this observation is complicated by the fact that catatonia has been associated with both schizophrenic and affective states, in which glutamatergic hypofunction involving the prefrontal cortex and anterior cingulated region has been noted.
6 –
8The treatment of catatonia has been well established with trials of lorazepam and electroconvulsive therapy (ECT),
3 and recent treatment guidelines list these as effective in both acute and chronic catatonia.
9,
10 However, if patients do not respond to these primary treatments, clinicians have little evidence on which to base treatment for benzodiazepine and ECT refractory catatonia. Hawkins et al.
11 identified only one case in which amantadine was used, noting that it was ineffective. However, this was followed by two cases of patients in whom amantadine was markedly effective in improving febrile catatonia, which spurred an interest in the role of the glutamate system in addressing this disorder.
5Because of its NMDA antagonist properties, Northoff et al.
2 list amantadine as a therapeutic agent that potentially leads to a down-regulation of glutamatergic-mediated excitation that is therapeutically effective in catatonia. Amantadine may indirectly compensate for the lack of GABA-ergic mediated neuronal inhibition. Specifically, amantadine has been shown to be beneficial in lorazepam refractory catatonia.
5,
12 It has been recommended that amantadine be initiated prior to ECT in refractory catatonia.
5 Memantine, a derivative of amantadine, has also been reported to be effective in catatonia.
13 Though there is no satisfactory animal model for catatonia, Loizzo et al.
14 used amantadine to reverse bulbocapnine-induced catalepsy in animals.
2We felt that clinicians might benefit from a review of catatonia patients treated with the glutamate antagonists amantadine and memantine. Such a review may be especially helpful in cases where catatonia proves resistant to treatment with lorazepam or ECT. We conclude our review by offering a treatment paradigm for patients with catatonia who are resistant to treatment with benzodiazepines or ECT.
METHOD
We completed a PubMed search using the following Medical Subject Headings (MESH) terms, without “exploding” them further: “amantadine,” “N-Methylaspartate” “N-Methyl-D-Aspartate” (and its variations suggested by MESH search on PubMed), “amantadine-N-mustard,” “MR 708,” “catatonia,” “schizophrenia, catatonic,” “catalepsy,” “glutamate,” “topiramate” and “memantine,” and limited the search results to human subjects. In addition, we searched MEDLINE, EMBASE and PsycINFO using the terms ”cataton*,” “amantadine,” “NMDA,” “glutamat*,” “topiramate” and “memantine.” We also searched other publications by lead authors in the field of catatonia research, and included papers in which catatonia was well documented as the focus of treatment and included a treatment response. We attempted to contact authors by e-mail to see if other unreported cases existed to be included in the review. Cases were limited to English language descriptions.
Each case was examined for age, sex, diagnosis, medications used, dose of glutamate antagonist, and route of administration. Amantadine and memantine were administered orally, except in the cases reported by Northoff et al.
5,
12 Time to response was determined as less than 1 day, 1 to 7 days, or more than 7 days. Northoff indicated that the time to response for amantadine was delayed as compared to lorazepam.
2 The pattern of response was listed by the rating scale or clinical signs used.
RESULTS
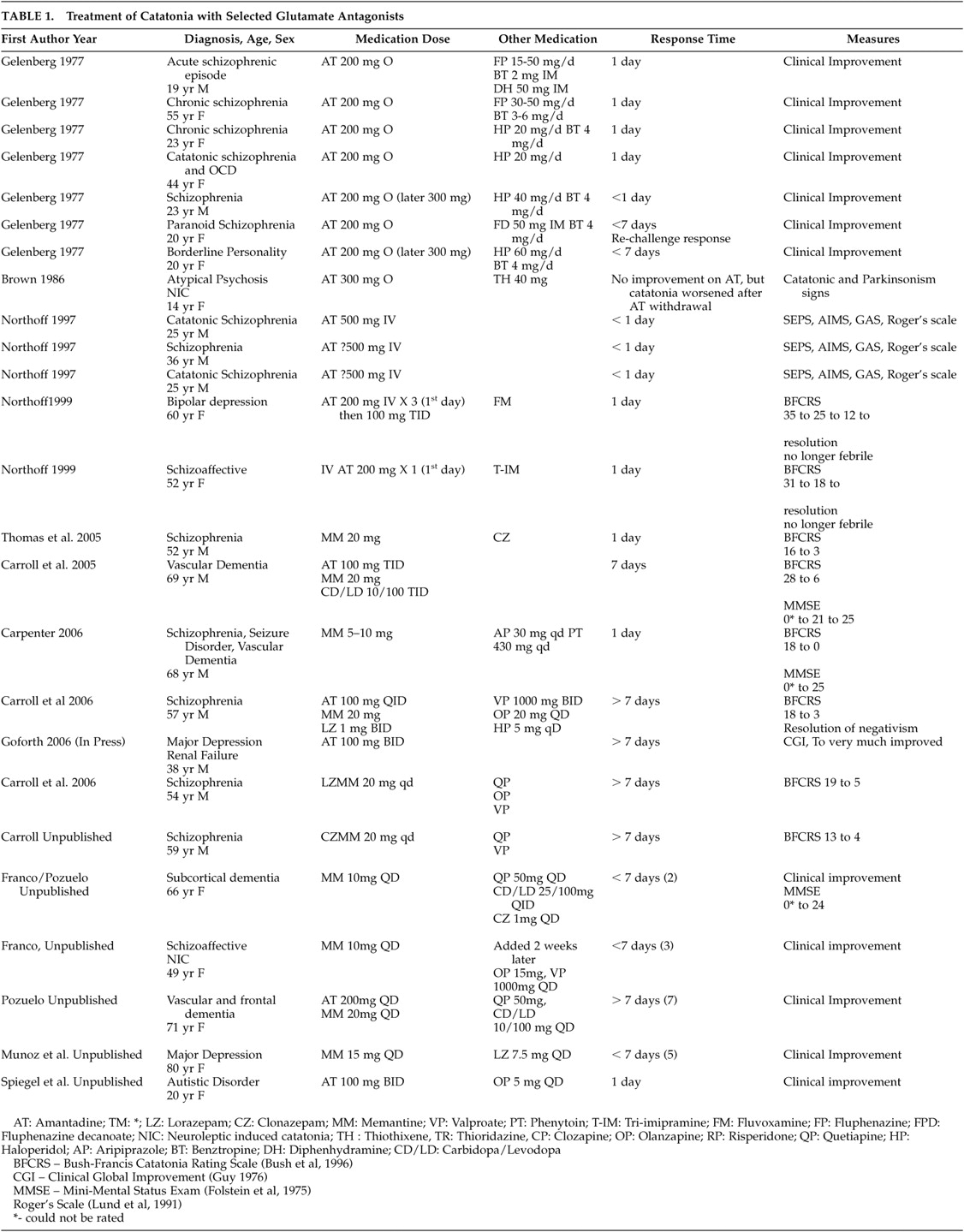
Twenty-five cases were identified of amantadine and memantine use in the treatment of catatonia (
Table 1 ). The response time generally ranged from 1 to 7 days after obtaining a therapeutic dose of any selected agent, although there was no standardized assessment for follow-up in most cases. The criteria for response were based upon clinical reduction of catatonic signs as described in the case reports or through the use of varied clinical outcome scales including the Bush-Francis Catatonia Rating Scale (BFCRS),
15 Modified Rogers Scale,
16 and the Clinical Global Impression (CGI).
17 All described cases in the literature and unpublished reports submitted for this review were characterized by substantial improvement after addition of a glutamate antagonist to the treatment regimen, which may reflect a bias of ascertainment in the literature, as negative cases are less likely to be reported for publication.
DISCUSSION
The established treatments of catatonia with benzodiazepines (i.e., lorazepam) and ECT remain as the modalities with the strongest evidence base to date, and the nature of treatments for catatonia make placebo-controlled, double-blind trials difficult to design. Catatonia is a neuropsychiatric illness that may respond to one treatment, even after failure to other standard treatments, if treated for a sufficient duration. This was demonstrated best in a double-blind placebo trial of amobarbital in catatonia. Subjects’ responses to amobarbital did not predict overall treatment response, as those who failed to improve initially with amobarbital eventually responded to other treatments, including ECT.
18The NMDA receptor is hypothesized to be dysfunctional in catatonia in the striato-cortical pathway or the cortico-cortical pathways, and NMDA hyperactivity appears to correspond to a loss of GABA-A and dopamine activity in these regions, which may clinically present as a lorazepam-resistant catatonic syndrome.
2 Thus, use of NMDA antagonism to attenuate glutamatergic hyperactivity most likely acts to improve catatonia and correspondingly may increase GABA-A and dopamine in previously deficient areas.
2,
13,
19 Similar findings of glutamate hyperactivity have been noted in treatment refractory mood disorders,
20 and overlap between catatonia and refractory mood disorders would be expected in a portion of the cases where the catatonia was secondary to either depressive illness or bipolar disorder. It is difficult to identify the precise mechanism of glutamate hyperactivity in catatonia. It is possible that there may be elevated extracellular glutamate in catatonia. However, we prefer to focus on the NMDA receptor, which may be allosterically open in catatonia, leading to increased glutamate activity. Amantadine and memantine are noncompetitive antagonists that would down-regulate the NMDA receptor.
Amantadine was originally approved for antiviral use in the 1960s, and was later noted to be effective in the treatment of parkinsonism.
21,
22 It is approved only for oral use in the United States, but other reports from Europe have included its intravenous administration.
2 It is well absorbed orally, and has an intermediate half-life of 12 to 18 hours in healthy individuals. Amantadine has mixed pharmacological effects and facilitates both central dopamine release, as well as delays central dopamine reuptake. It has also been speculated that amantadine may exert a direct, postsynaptic effect by increasing the number of or altering the configuration of postsynaptic dopaminergic receptors. Importantly, however, for the issue of treating refractory catatonia, it also exhibits moderate, reversible NMDA glutamate receptor antagonism.
23,
24 Thus, its effect upon refractory catatonia is likely a combination of both direct and indirect actions upon both the dopamine and glutaminergeric systems.
Alternatively, memantine is a low-to-moderate affinity, voltage-dependent, noncompetitive, NMDA receptor antagonist related structurally to amantadine and approved for use in moderate to severe Alzheimer disease. It is similar to amantadine in that it is well absorbed orally, with peak serum levels achieved in approximately 6 hours. However, it has a markedly longer half-life of approximately 60 to 80 hours in Phase I pharmacokinetic studies (Namenda prescribing information, 2006). Memantine’s potential efficacy in catatonia is likely secondary to its direct NMDA antagonism and consequent reduction in glutamine excitotoxicity. Memantine does not appear to affect dopamine transmission directly.
McDaniel et al.
25 presented a case series of four subjects with catatonia who failed treatment with commonly used modalities, such as lorazepam and divalproex, but who eventually responded when treated with adjunctive topiramate. This lends further support to the role of glutamate hyperactivity in treatment refractory catatonia.
Topiramate is a novel anticonvulsant agent approved for use in partial onset or generalized tonic-clonic epilepsy and migraines; however, its exact mechanism of action in vivo is ill understood. Three different effects upon cultured neurons have been identified and include blockade of state-dependent sodium channels, as well as a GABA-ergic mechanism that appears to increase the frequency at which GABA activates GABA-A channels, and increases the ability of GABA to induce an influx of Cl ions into the neuron. This increased GABA activity is not blocked by the administration of flumazenil and appears distinct from the effect of barbiturates. Third, topiramate antagonizes the ability of kainate to activate AMPA receptors, which are a distinct, nonNMDA glutamate receptor without direct NMDA receptor effects; however, given that AMPA/kainate receptors are often co-localized with NMDA receptors, one cannot rule out indirect antagonism on NMDA receptors.
26Miyoaka et al.
27 reported two patients with acute schizophrenia with catatonic stupor that responded to minocycline. Minocycline was used as an adjunctive treatment to antipsychotics at a dose of 150 mg per day in the absence of infection. The response noted with this agent is pertinent in that minocycline may act as an NMDA antagonist, as it has demonstrated protection against NMDA excitotoxicity in some preclinical studies, however, its precise mechanism of action in the CNS is not well understood.
27,
28The two glutamate antagonists examined in this review, amantadine and memantine, share similar mechanisms of action and the capacity to diminish glutamatergic hyperactivity. These clinical data suggest there could be an emerging role for glutamate antagonists in the treatment of patients with refractory catatonic syndromes.
CONCLUSIONS
Catatonia remains a common neuropsychiatric illness with increasing evidence of a glutamatergic component. The glutamatergic role does not appear to be dependent upon the primary psychiatric diagnosis producing catatonia. Lorazepam and ECT have been clearly shown to be first-line choices for the treatment of catatonia by available evidence; however, these agents may be insufficient to clinically improve this movement disorder in selected cases. Antiglutamate agents, such as amantadine, memantine, and others, may offer effective treatment by either direct glutamate antagonism or indirect GABA and dopamine effects.
Though there are no studies comparing the efficacy or effectiveness of amantadine versus memantine, it should be noted that some patients may develop psychosis from addition of amantadine,
29 while others may fail to respond to amantadine, or may suffer diminishing response after a period of time. In these cases, memantine may offer more selective and increased NMDA antagonism with a lower risk of psychosis due to its negligible effect upon the dopamine system.
30 Similarly, topiramate may offer effective glutamate antagonism via AMPA receptors combined with GABA-ergic effects, with a negligible risk of psychosis.
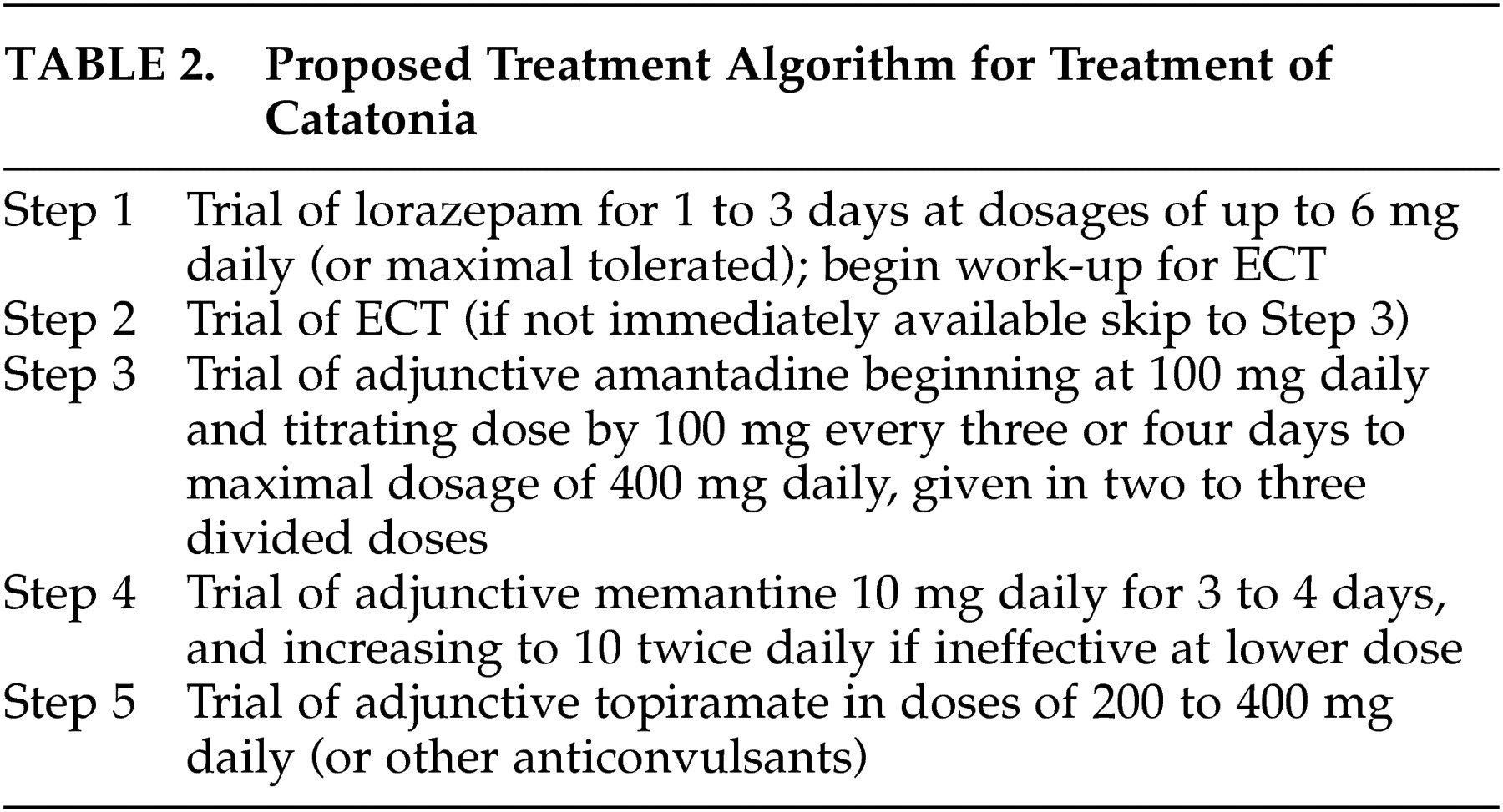
Based on this case series, we suggest a treatment algorithm for patients presenting with a catatonic syndrome, regardless of the underlying etiology (
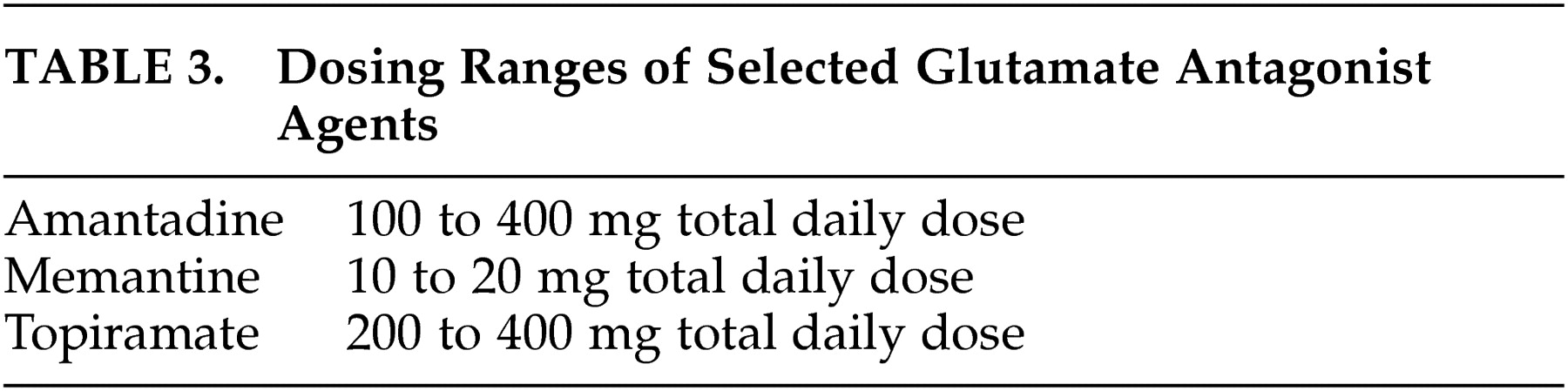
Table 2 ). We formulated this treatment algorithm based upon multiple considerations, including the available data regarding efficacy, safety, and cost. We also included dosages based on this review. We cannot comment on the use of higher dosages, but recognize that clinicians may select higher doses based upon clinical response and judgment (
Table 3 ). Further studies are required to better delineate the role of the glutamate system in catatonic presentations and to better understand the role of glutamate antagonists in the treatment of catatonic presentations.
Acknowledgments
Dr. Carroll is a speaker for Forest Pharmaceuticals, Inc. Labs. We also wish to thank Francisco Appiani M.D., Chairman, Department of Psychiatry, “Campo de Mayo” Military Hospital, Buenos Aires, Argentina, Victoria Achaval, M.D. and Natalia Yulan, M.D., Residents, Department of Psychiatry, Campo de Mayo Military Hospital, Buenos Aires, Argentina, who assisted Dr. Muñoz with one case. The authors thank Tina Fore, Librarian, VA Medical Center, Chillicothe, Ohio, for her assistance in obtaining articles for this review.