N eurological soft signs are considered useful clinical indicators of subtle brain dysfunction.
1,
2 Previous studies have suggested that these neurological abnormalities reflect a genetic vulnerability
3,
4 or perinatal trauma.
5 Neurological soft signs have been reported in offenders
6 –
8 and in patients with different psychiatric disorders, including schizophrenia and other psychotic disorders,
1 –
5,
9 mood disorders,
10 –
12 substance use disorders,
13,
14 anxiety disorders,
15 –
17 and antisocial and borderline personality disorders.
6,
18,
19 In addition, there is evidence that neurological soft signs are specifically associated with impulsivity, aggression, and violence in psychiatric patients.
20 –
22 The main purposes of this study were to compare neurological soft signs between offenders and healthy comparison subjects and to examine the relationship between neurological soft signs and major psychiatric disorders among prisoners. To our knowledge, this is the first study to assess neurological soft signs in such a large, representative sample of offenders (N=351), and the first one to examine the association between almost all major psychiatric categories and neurological soft signs at the same time.
METHOD
Three hundred fifty-one prisoners and 80 healthy comparison subjects participated in the study. The details of recruitment were described previously.
24 Briefly, prisoners were recruited using stratified random sampling from Qasr Prison, one of the largest male prisons in Iran. The sample was stratified by type of index offense to ensure adequate representation of all five official crime categories. According to official Iranian statistics, offenses are classified into five categories including felonies (e.g., murder, kidnapping, and armed robbery), misdemeanors (e.g., pickpocketing, purse-snatching, and other petty larcenies), drug-related offenses (e.g., drug use, possession, or trafficking), “immoral” acts (e.g., fornication and prostitution), and financial crimes (e.g., bounced checks). The study was designed to recruit 80 prisoners from each offense category to reach a total sample size of 400. However, 49 individuals (12%) refused to participate. The individuals who refused did not differ from those who participated in terms of age, level of education, and number of previous prison sentences.
24 Healthy volunteers were recruited from hospital staff, university students, and their relatives. They matched the prisoners group with respect to gender, age, and education. They were interviewed before recruitment to make sure that they had no history of crime, substantial medical or neurological conditions, and personal or family history of psychiatric disorders.
Participants were informed that the study was confidential, anonymous, and voluntary. All participants gave informed consent after complete description of the study. The project was conducted in accordance with the Declaration of Helsinki, Finland, and was approved by the ethical committee at Tehran University of Medical Sciences.
Assessment
All assessments were conducted by four third-year psychiatric trainees (M.P., O.Y., S.A., and S.V.S.) who went through a 5-day study-specific training program. Assessments were regularly supervised by board-certified psychiatrist (S.M.A.) and neurologist (M.N.) who were trained in the use of instruments.
Prisoners were interviewed using the clinical version of the Structured Clinical Interview for DSM-IV Axis I disorders (SCID-CV)
24,
25 and the Hare Psychopathy Checklist: Screening Version (PCL:SV).
26,
27 Prisoners were interviewed alone by one of four interviewers. Each interview took about 90 minutes on average. The SCID-CV allows assessment of both current and lifetime diagnoses. Current disorders were diagnosed if the full criteria were met at any time during the current month, and lifetime disorders were diagnosed if the full criteria had been ever met during patients’ lives. We used four major Axis I diagnostic categories (i.e., psychotic disorders, mood disorders, anxiety disorders, and substance use disorders) for data analysis. Other diagnostic categories (e.g., somatoform disorders) were not prevalent
24 and were not included in the analyses. For categorical diagnosis of psychopathy, we used the recommended cutoff score of 18 on the PCL-SV.
26All participants underwent neurological examination using the Neurological Evaluation Scale (NES).
28 The scale consists of 26 items designed to assess three functional domains: sensory integration, motor coordination, and the sequencing of complex motor acts. Miscellaneous items, including abnormalities in eye movements, frontal release signs, and short-term memory, are not part of the above subscales but are included in the overall score. Total scores on each of the three domains mentioned above, total score for miscellaneous tests, and overall score were calculated. We did not include cerebral dominance in calculating the overall or miscellaneous scores. Neurological examination was conducted by the psychiatric trainees who had not interviewed the participant and were blind to psychiatric diagnosis and offense category.
Statistical Analysis
Data were analyzed using SPSS, version 11.5 (SPSS Inc, Chicago). Differences between offenders and normal comparisons were tested using chi-square or Fisher’s exact tests for categorical measures and unpaired t test or analysis of variance (ANOVA) for continuous measures. We used four multivariate analyses of covariance (MANCOVAs) with conservative Pillai’s criterion to examine the study hypotheses. In all four analyses, the dependent variables were the four NES subscale scores. The overall NES score was assessed using main effect in MANCOVA and, therefore, was not entered as a separate variable. Age and education were entered as covariates to control for their potentially confounding effects. The first MANCOVA was conducted to examine the difference between offenders and healthy comparison subjects on the NES. The independent variable was the dichotomous grouping variable indicating whether a participant was an offender or a comparison subject. The second MANCOVA examined the relation of neurological soft signs with current psychiatric diagnoses and offense type. The independent variables were four current axis I diagnostic categories (i.e., psychotic disorders, mood disorders, anxiety disorders, and substance use disorders), psychopathy, and offense type. The third MANCOVA was conducted to evaluate the relation of neurological soft signs with lifetime psychiatric diagnoses and offense type. The independent variables were similar to the second MANCOVA, except that lifetime psychiatric diagnoses were used instead of current diagnoses. Finally, the last MANCOVA assessed the difference in the NES scores between felony and misdemeanor offenders. We specifically compared these two offense groups because they represented the two extremes of criminal behavior. Prisoners in the felony group were typically convicted of a single, severely violent felony while those in the misdemeanor group usually had repeated convictions for mildly abusive crimes.
24 In addition, these offenders, in contrast to other offense groups, were well comparable with offenders in other legal systems. The independent variables were similar to the third MANCOVA, except that the two offense types were used instead of all offense groups. Inequality of variances did not appear to be a problem because Levene’s tests were generally nonsignificant. All statistical tests were two-tailed and were considered significant at p<0.05.
RESULTS
Table 1 shows demographic data. There were no significant differences in age and education between offenders and comparison subjects. Offenders had a lower rate of marriage. In addition, the majority were born in large cities, in contrast to the comparison group. Comparison of demographic variables in inmates showed that they were not a homogenous group. Prisoners with financial crimes were older and more educated, had higher rates of marriage, and were born mostly in the metropolitan city of Tehran.
Comparison of Offenders With Healthy Subjects
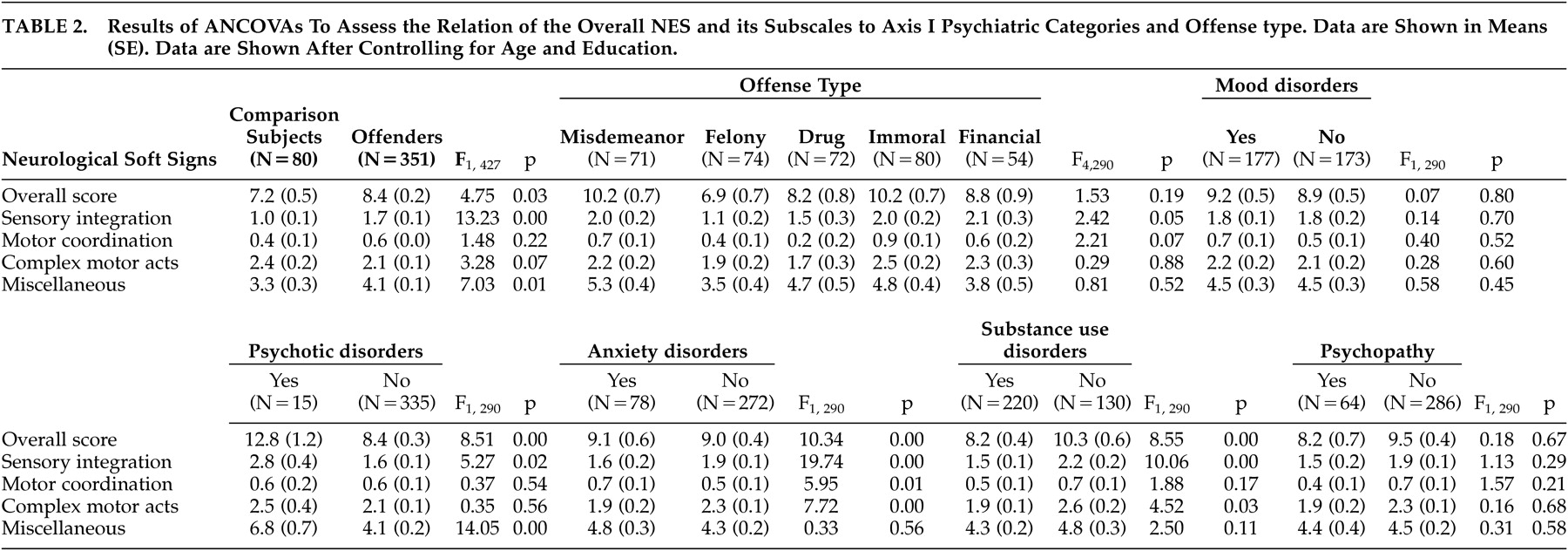
Table 2 shows the data comparing offenders and healthy subjects on the NES. The overall NES score was higher in offenders than in healthy subjects. MANCOVA showed that the main effect of group was significant (
F [4, 424]=8.10, p<0.001). The covariates of age and education were also significant; that is, older age and lower educational level were associated with higher NES scores (
F [4, 424]=10.52, p<0.001 for age, and
F [4, 424]=25.52, p<0.001 for education). The tests of between-subject effects showed that offenders had higher scores on the sensory integration and miscellaneous tests. There was no significant difference between offenders and healthy subjects on the motor coordination and sequencing of complex motor acts.
To ensure that the high NES scores did not merely reflect the psychiatric morbidity in offenders, the analysis was repeated with a subset of offenders (N=70) who had no history of axis I psychiatric diagnosis. Similarly, these offenders had high rates on the overall NES score ( F [4, 146]=4.61, p=0.002), sensory integration ( F [1, 146]=13.85, p<0.001), and miscellaneous tests ( F [1, 146]=4.10, p=0.04) in comparison with healthy subjects.
Effect of Current Psychiatric Diagnoses
The overall NES score was significantly predicted by current diagnosis of psychotic disorders. MANCOVA showed a significant main effect for current psychotic disorders (
F [4, 294]=3.18, p=0.014). No significant main effect was found for other independent variables including current mood disorders (
F [4, 294]=0.64, p=0.64), current anxiety disorders (
F [4, 294]=0.26, p=0.90), current substance use disorders (
F [4, 294]=0.31, p=0.87), psychopathy (
F [4, 294]=0.13, p=0.97), and offense type (
F (15, 1188)=0.66, p=0.84). Both covariates of age and education were significant (
F [4, 294]=3.18, p=0.014 for age, and
F [4, 294]=17.21, p<0.001 for education). Based on interviewers’ impressions, the current diagnosis of substance use disorders was thought to be an underestimate. Moreover, drug and alcohol are generally less available in prison, and current rates of substance use disorders in cross-sectional samples of prisoners will probably underestimate the true prevalence.
24,
29 Thus, we decided to use the lifetime diagnoses for further analyses.
Effect of Lifetime Psychiatric Diagnoses
The overall NES score was significantly predicted by lifetime diagnoses of psychotic, anxiety, and substance use disorders. MANCOVA revealed a significant main effect for lifetime diagnosis of psychotic disorders ( F [4, 287]=4.29, p=0.002), anxiety disorders ( F [4, 287]=6.47, p<0.001), and substance use disorders ( F [4, 287]=2.89, p=0.023). No significant main effect was found for lifetime mood disorders ( F [4, 287]=0.46, p=0.768), psychopathy ( F [4, 287]= 0.93, p=0.448), or type of offense ( F [16, 1160]=1.33, p=0.170). Both covariates were significant (for age F [4, 287]=2.55, p=0.039, and for education F [4, 287]=17.17, p<0.001).
Table 2 shows the main effect of each independent variable on the NES subscales, using the tests of between-subject effects. Psychotic disorders were associated with higher rates on the overall NES score and with more impairment in sensory integration and miscellaneous tests. Substance use disorders were related to lower overall scores on the NES and better performance in sensory integration and sequencing of complex motor acts. Anxiety disorders had mixed effects and were associated with higher rates on the overall NES score and motor coordination but lower scores on the sensory integration and sequencing of complex motor acts. Mood disorders and offense type had no significant association with the overall NES and its subscales.
The lower NES scores in the prisoners with substance use disorders might result from overrepresentation of neurologically impaired prisoners (i.e., those with psychotic and/or anxiety disorders) in the group without substance use disorders. However, the Fisher’s exact test showed that neither psychotic disorders nor anxiety disorders were overrepresented in the latter group. Psychotic disorders were diagnosed in 11 prisoners with substance use disorders (5.0%) and in four prisoners without such disorders (3.1%, p=0.586). Anxiety disorders were seen in 50 prisoners with substance use disorders (22.6%) and in 28 prisoners without such disorders (21.5%, p=0.894).
Comparing Felons and Misdemeanants
MANCOVA showed that the overall NES score was higher in misdemeanants than in felons ( F [4, 114]=5.24, p=0.001). The tests of between-subject effects revealed that the misdemeanor group had significantly higher scores on sensory integration ( F [1, 117]=7.76, p=0.006) and motor coordination ( F [1, 117]=13.01, p<0.001) in comparison to the felony group. The main effect for lifetime substance use disorders was also significant ( F [4, 114]=4.31, p=0.003) but no significant effect was found for other independent variables. The covariates were significant (for age F [4, 114]=3.71, p=0.007 and for education F [4, 114]=13.54, p<0.001).
DISCUSSION
This study investigated the association of neurological soft signs in a sample of 351 male offenders and 80 healthy subjects. Its main findings were that neurological signs, as measured by the overall NES score, were significantly increased in offenders compared with healthy subjects. We also found that offenders with repeated misdemeanors had higher rates of neurological signs than those with a single major felony. Finally, we found increased NES scores in those with current diagnoses of psychoses, and lifetime disorders of most diagnostic groups.
The first finding is consistent with previous studies.
6 –
8 Those studies, however, were conducted on small samples of homicidal and violent criminals and, to our knowledge, neurological soft signs have not previously been examined in a representative sample of all offense groups. Increased neurological abnormalities in offenders with repetitive minor crimes may be consistent with the previous reports that neurological impairment is mainly seen in the unsuccessful criminals who are caught frequently rather than those who are well organized and are rarely caught.
30,
31The finding that psychotic disorders were associated with higher rates of neurological abnormalities replicates various studies that have reported increased rates of abnormal neurological signs in patients with psychotic disorders.
1 –
5 In addition, the association between psychotic disorders and poor sensory integration found in our study is similar to previous reports.
1The results revealed that a history of anxiety disorders had mixed effects. These disorders were associated with higher scores on the overall NES as well as on the motor coordination. Several previous studies have also reported a high level of neurological soft signs in anxiety disorders, including obsessive-compulsive disorder, posttraumatic stress disorder, and social phobia.
15 –
17 In addition, the relationship between motor coordination impairment and anxiety disorders is in line with previous reports.
15,
32 On the other hand, we found that offenders with anxiety disorders, compared to those without anxiety disorders, had lower neurological abnormalities on the sensory integration and sequencing of complex motor acts. This finding may be consistent with the previous studies that showed higher levels of anxiety are relatively advantageous in children with psychopathic tendencies.
33,
34We found that lifetime diagnosis of substance use disorders was associated with lower rates of neurological abnormalities and better performance in sensory integration and sequencing of complex motor acts. A few studies have explored the relation of neurological soft signs to substance dependence or abuse.
13,
14 We could not find any studies that assessed this association in prisoners, despite the fact that substance use disorders are the most common cause of psychiatric morbidity in prison populations.
29 The neurobiological basis of this strong association between crime and substance use is not well explored. Interestingly, an animal study found that nicotine improved motor performance of mutant mice with a hypersensitive α4 nicotinic receptor.
35 Nicotine dependence is not included in the SCID-CV and therefore was not reported in this study; however, there is evidence that cigarette smoking is highly prevalent in substance use disorders
36 and prisoners with lifetime substance use disorders commonly smoked cigarettes in prison. However, interactions among neurological abnormalities, criminal behavior, and substance use disorders are rather complex and other alternative mechanisms cannot be ruled out.
37,
38 Therefore, additional studies are warranted to further evaluate this association.
We could not find a significant relation of neurological soft signs to mood disorders, or psychopathy. This inconsistency with previous studies
6,
11,
12 may have resulted from the fact that we examined the associations after controlling for the confounding effect of demographic characteristics and other psychiatric disorders. Moreover, there is evidence that psychopaths are not a homogeneous group and only a subset of them may have neurological abnormalities.
30,
31 Therefore, in this representative sample, the neurologically impaired psychopaths might fade away among those who had no impairment.
Our study had a number of limitations. First, the sample was only composed of men. It has been reported that there may be a gender difference in neurological soft signs.
32 Second, the sample was recruited from sentenced prisoners and the results cannot be generalized to remand detainees who may have different prevalence rates of psychiatric morbidity and neurological abnormality. No prisoner in the present study was diagnosed with bipolar disorders which are prevalent in remanded populations.
29 Third, although comparison subjects were initially interviewed to make sure that they had no psychiatric illness, they were not assessed with the SCID-CV, possibly rendering their psychiatric assessment less reliable than the offender group’s. Finally, the SCID:CV does not allow nicotine use or multiple substance use diagnoses. Therefore, their impact on neurological performance could not be evaluated in the present study.
In conclusion, we found that offenders had impaired neurological performance. Offenders with repeated misdemeanors had higher rates of neurological soft signs than those with a single major felony. Axis I diagnostic categories were associated with distinct patterns of neurological abnormalities.