A variety of neuroanatomical abnormalities have been described in posttraumatic stress disorder (PTSD). Despite some inconsistencies in findings,
1 –
4 several studies have shown hippocampal volume deficits in patients with PTSD.
5 –
7 While most studies examining neuroanatomical abnormalities in patients with PTSD have focused on the hippocampus, other brain regions appear to be involved as well.
8 Among these are volume deficits in the anterior cingulate cortex,
5,
9 –
12 although far fewer structural studies have examined anterior cingulate cortex involvement in PTSD than have examined hippocampal volume. Li et al.
11 reported an abnormal insula volume in patients with PTSD. Although Myslobodsky et al.
13 reported only questionable overall brain atrophy in combat-related PTSD, Wignall et al.
14 found decreased total brain volume in patients with PTSD.
Another brain region possibly connected to PTSD is the amygdala, which is involved in behavioral regulation,
15 evaluation of potentially threatening stimuli,
16 fear,
17 fear conditioning,
18,
19 and memory for stressful events,
20 all of which suggests a possible role for this structure in PTSD. Furthermore, in an animal model, chronic stress increased dendritic aborization in the extended amygdala and did not cause dendritic atrophy in the central nucleus of the amygdala.
21 In humans, the amygdala shows increased activity in patients with PTSD.
16 Together, the function of the amygdala in fear processing and memory of stressful events, the increased activity of the amygdala in patients with PTSD, and dendritic plasticity to stress in the extended amygdala in animal models provide theoretical support for attempting to better understand amygdala anatomy in PTSD.
In fact, several studies have investigated amygdala volume as related to PTSD.
1,
14,
22 –
28 Pavlisa et al.
28 reported larger left than right amygdala volume in 11 PTSD patients relative to 40 matched healthy comparison subjects whose data were derived from two other reports.
29,
30 Other studies reported no significant group differences between PTSD patients and comparison subjects in amygdala volume.
1,
14,
25,
26 In a meta-analysis, Karl et al.
5 found no differences in right amygdala volume between groups, but did find a smaller left amygdala in PTSD patients compared with healthy comparison subjects who were not exposed to trauma and with healthy comparison subjects who were exposed to trauma but did not have PTSD. Although their meta-analysis provided important findings in amygdala volumetric differences in patients with PTSD, Karl et al.
5 used a sample that included pediatric data,
31 –
33 which may have potentially biased their conclusions, given the evidence that adolescence is a period in which considerable neurodevelopment occurs.
8,
34,
35Although Karl et al.
5 meta-analytically characterized amygdala volume in patients with PTSD using both pediatric and adult data, there has not been a meta-analysis of amygdala volume in adult patients with PTSD to date. Our objective in this study was to meta-analytically examine amygdala volume as determined by MRI in adult patients with PTSD relative to comparison subjects. Based on existing studies, we hypothesized that we would find a smaller left amygdala in PTSD patients compared with healthy comparison subjects who were not exposed to trauma and with trauma-exposed comparison subjects who did not have PTSD.
METHODS
Using the words and terms “posttraumatic stress disorder,” “MRI,” “hippocampus,” and “amygdala,” we searched the electronic databases PubMed and PsycINFO for peer-reviewed articles containing volumetric findings on the amygdala in patients with PTSD relative to healthy comparison subjects who were not exposed to trauma, trauma-exposed comparison subjects who did not have PTSD, or both. After an initial screening of titles and abstracts that met inclusion criteria through 2007, we obtained the full text of those articles that appeared to contain the relevant data. We searched the articles’ reference lists for any additional pertinent papers, and we examined studies evaluating the hippocampus in patients with PTSD for any volumetric data on the amygdala. Because neuroanatomy has been found to differ between children and adults with PTSD,
8,
34,
35 we limited our analysis to subjects who were adults at the time of the MRI brain scan. We included all studies containing amygdala volume data in adult PTSD that met our content-related criteria, regardless of participant gender, type of trauma, duration of PTSD, and number of subjects, even though these factors may potentially confound the interpretation of neuroanatomical studies in PTSD.
8 We did not require that the included studies meet any particular methodological criteria.
One researcher (FLW) experienced in data extraction tabulated the relevant variables from all studies. We also extracted hippocampal volumetric data when available from the studies to investigate whether any volume differences in the amygdala occurred in the context of hippocampal volume differences.
To compare amygdala volume between patients with PTSD and comparison subjects, the Hedges’
g effect size was calculated according to the formula
g =standardized mean difference (
d ) × correction factor (
J ),
36 in which standard mean difference (
d ) scores for amygdala volumes were obtained by dividing the difference between-group means by the pooled standard deviation and controlling for differences in sample size by calculating the correction factor (
J ) according to the formula: in which df=N total−2 to control for differences in sample sizes.
37 In general, effect sizes of 0.20, 0.50, and 0.80 represent a weak, moderate, and strong effect, respectively.
38 Data for the left and right amygdala were pooled separately according to group type to test whether the results differed according to laterality. Only one effect size per study was included in the meta-analysis.
39We used Comprehensive Meta-Analysis, version 2.0 (Biostat, Englewood, N.J.) for all calculations. In our analysis, we used a fixed-effects model, which assumes that underlying effects on measures are identical.
36 The fixed-effects model is also used to address the issue of imprecise estimates of the between-studies variance due to the small number of studies (M. Borenstein, personal communication, August 30, 2007).
Heterogeneity tests, including the
Q statistic and
I -squared test, were done to assess the appropriateness of pooling the data. The
Q statistic was used to assess the heterogeneity of the specific set of effect sizes.
37 The
I -squared test is a more intuitive test of heterogeneity than the
Q test because the former is not directly affected by the number of studies in the analysis.
40 The
I -squared test addresses the degree of variance between studies; indices on the order of 25, 50, and 75 can be considered low, moderate, and high between-study variance, respectively.
40A concern in conducting a meta-analysis is the potential for publication bias, in which small, statistically nonsignificant studies may remain unpublished, thus potentially overestimating the effect sizes in a meta-analysis of published studies. We used three statistical methods to address this problem. First, we performed a classic fail-safe N analysis to determine the number of additional null studies that would be needed to make the results nonsignificant.
41 Second, we calculated an Orwin’s fail-safe N,
42 which indicates how many studies with an effect size of zero would be needed to reduce the combined effect size to a smaller value, such as 0.20 in this case.
43 A larger N indicates that the effect can be further generalized. Third, we performed a trim-and-fill calculation, which uses an iterative procedure to remove the most extreme small studies from the positive side of a funnel plot and recomputes the effect size at each iteration, until the funnel plot is symmetric about the new effect size. A smaller resulting shift in effect size indicates a higher accuracy of the initial effect size.
44 Because only two studies reported the total amygdala volume both for healthy comparison subjects who were not exposed to trauma and for healthy, trauma-exposed comparison subjects who did not have PTSD, we were unable to compute publication-bias statistics for amygdala volume comparisons between these two groups.
RESULTS
Nine articles containing adequate information to calculate effect sizes met our inclusion criteria and were included in the meta-analysis.
1,
14,
22 –
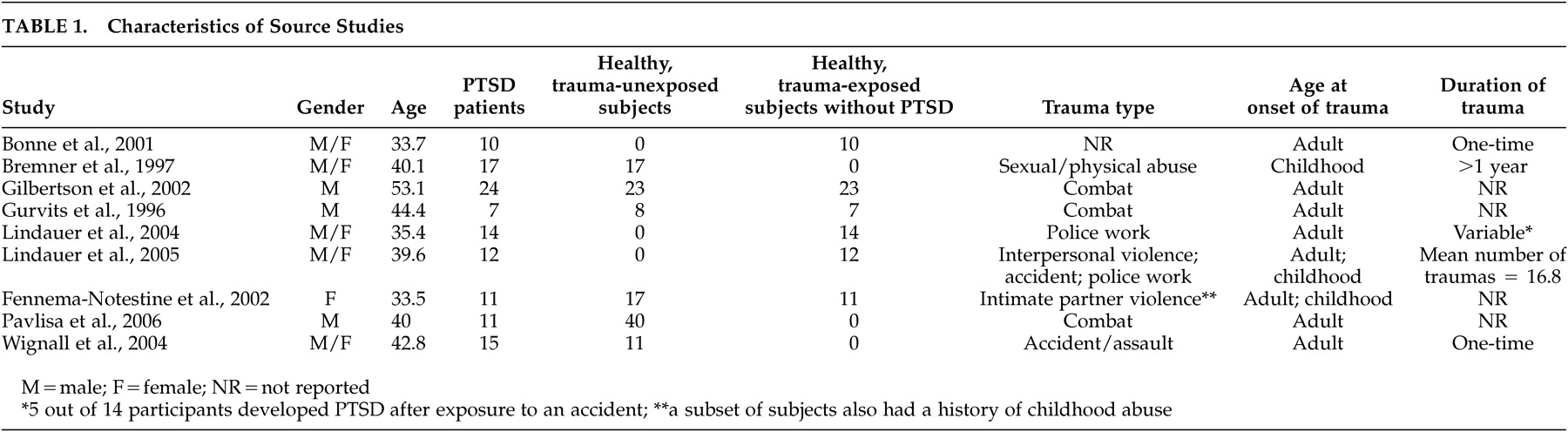
28 The characteristics of the included studies are summarized in
Table 1 . One study
28 used as a comparison group data matched for sex and handedness from two other reports.
29,
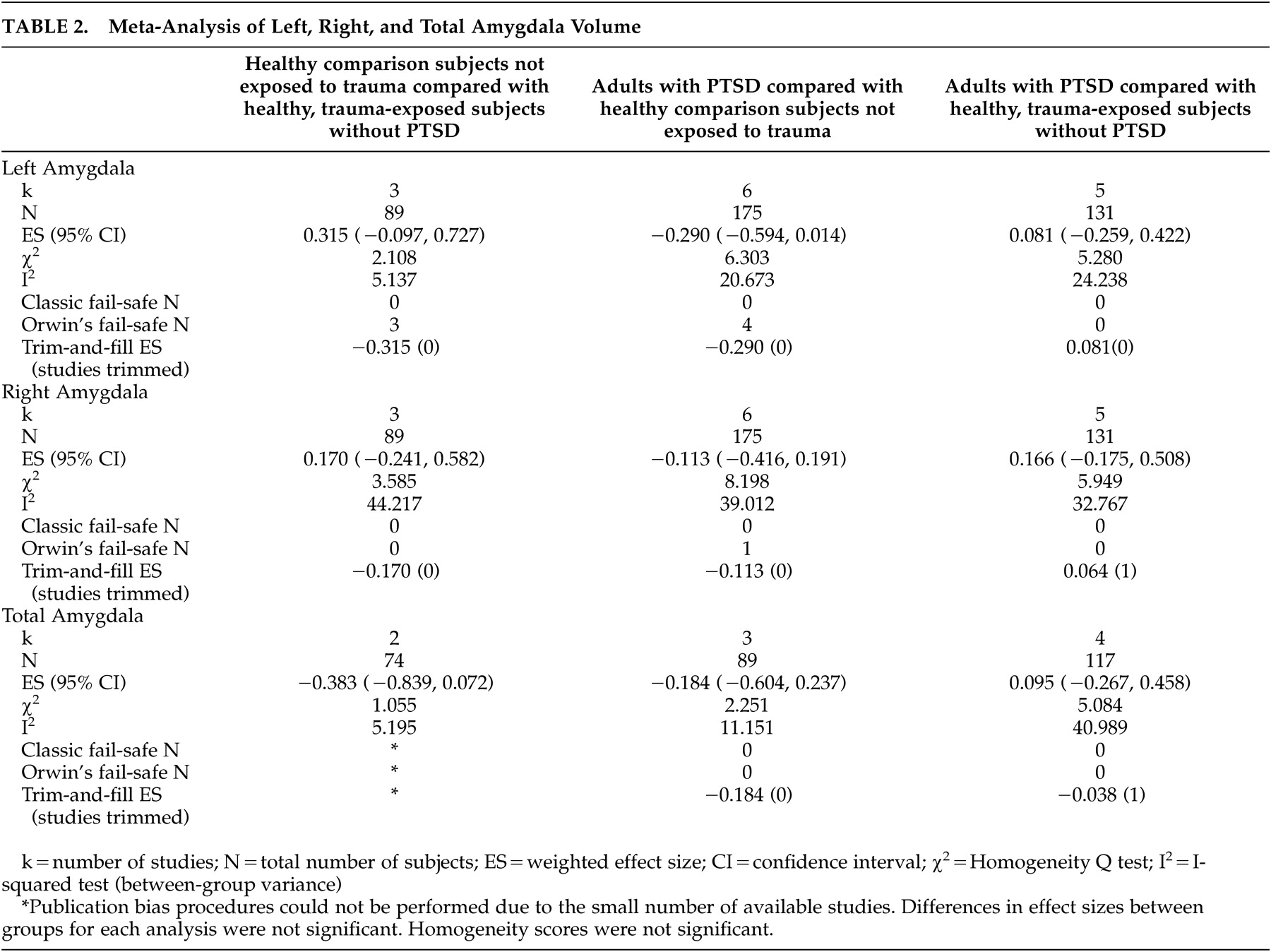
30The numbers of studies and subjects, the effect sizes, publication bias procedures, and analyses of heterogeneity are indicated in
Table 2 . There were no significant differences in total, left, and right amygdala volumes between healthy comparison subjects not exposed to trauma and healthy, trauma-exposed subjects without PTSD. In the comparison between patients with PTSD and healthy, trauma-unexposed subjects, there were no significant differences in total, left, and right amygdala volumes. However, the effect size for the left amygdala was −0.290 with a corresponding
p value of 0.061, indicating a possible trend for a smaller left amygdala volume in the patients with PTSD. There were no significant differences in total, left, and right amygdala volumes between patients with PTSD and healthy, trauma-exposed comparison subjects without PTSD. Analyses of heterogeneity were not significant for the
Q statistic, and the
I 2 dispersion values were within the minimal to moderate range for all comparison groups.
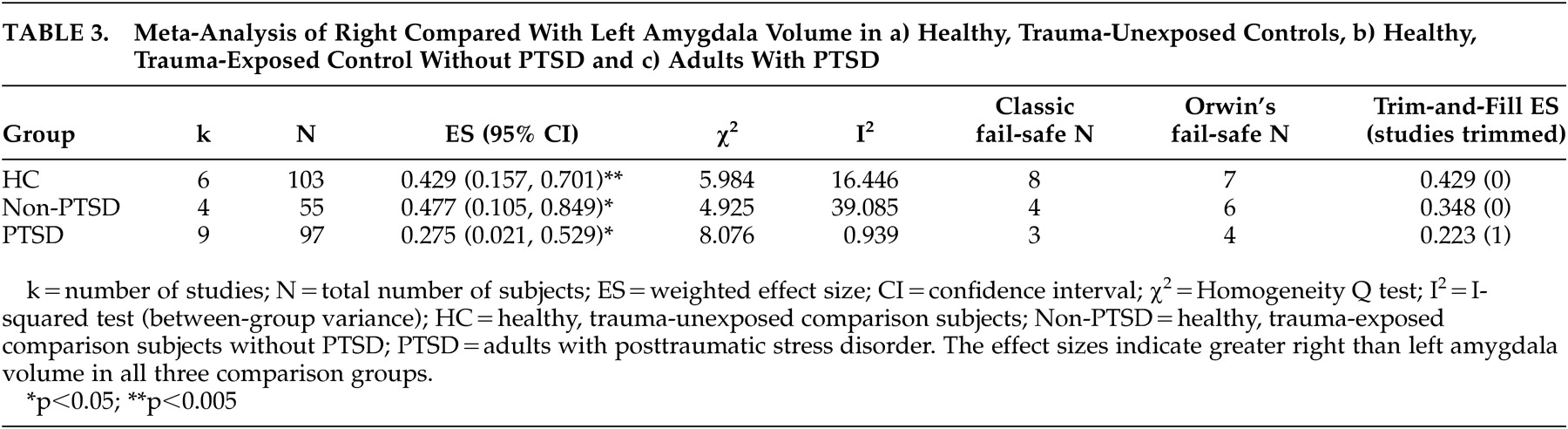
In contrast to the findings that showed no significant differences in amygdala volumes between groups, the right amygdala was significantly larger than the left amygdala in healthy subjects not exposed to trauma [effect size=0.429 (95% CI=0.157 to 0.701), N=206, p<0.005], in healthy, trauma-exposed comparison subjects without PTSD [effect size=0.348 (95% CI=0.017 to 0.679), N=138, p<0.05], and in patients with PTSD [effect size=0.275 (95% CI=0.021, 0.529), N=230, p<0.05] (
Table 3 ).
Several studies reported both amygdala and hippocampal volumetric data,
1,
14,
22 –
27 enabling a determination of whether hippocampal volume deficits were present even if no significant differences in amygdala volumes existed between groups. In contrast to the findings for amygdala volume, in the group of studies reporting volume data for both the hippocampus and amygdala, left and right hippocampal volumes were significantly smaller in the group of patients with PTSD compared with both the healthy subjects not exposed to trauma and with the group of healthy, trauma-exposed comparison subjects without PTSD. Furthermore, the right hippocampus was significantly smaller in the healthy, trauma-exposed group without PTSD compared with the healthy, trauma-unexposed group, although no significant differences were found for the left hippocampus. However,
Q values were significant in the analyses comparing the PTSD groups with both the healthy, trauma-unexposed group and to the healthy, trauma-exposed group without PTSD, precluding effect size calculations for the hippocampus in this sample. In further contrast to the amygdala findings, there were no significant symmetry differences between left and right hippocampal volumes across all three comparison groups in this sample.
DISCUSSION
From this meta-analysis of amygdala volume in adult PTSD, two main findings emerge. First, in both the PTSD and the comparison groups (those not exposed to trauma and those exposed to trauma without PTSD), the right amygdala was significantly larger than the left. The finding of a larger right amygdala than left provides evidence for an asymmetrical lateralization in the volume of the amygdala in healthy comparison subjects that appears to be preserved in patients with PTSD. The findings of amygdala asymmetry are consistent with those of Pedraza et al.,
45 who found right greater than left amygdala volume in their meta-analysis of 51 studies containing 2,000 healthy adult subjects. Our findings are also consistent with Murphy et al.’s
46 findings of amygdala asymmetry in postmortem healthy adult human brains. Our findings of greater volume in the right amygdala than in the left in patients with PTSD and in healthy comparison subjects indicate preserved amygdala asymmetry in adults with PTSD.
The second main finding from our study is that we observed no significant volume differences in the left and right amygdala in comparing subjects with PTSD both with healthy comparison subjects not exposed to trauma and with healthy, trauma-exposed subjects without PTSD. This finding was in contrast to our hypothesis that we would find a smaller left amygdala in patients with PTSD relative to comparison subjects.
In the meta-analysis of those studies containing data for both the amygdala and the hippocampus, left and right hippocampal volumes were smaller in the PTSD group relative to both comparison groups, indicating that amygdala volume in patients with PTSD does not differ from comparison groups even when the hippocampal volume deficits are also present in the PTSD group. The deficits in hippocampal volume further argue that the studies used in our meta-analysis are representative of PTSD patients in whom there are hippocampal volume deficits. In the comparisons showing significant differences in hippocampal volumes between PTSD and comparison groups, the Q statistic was significant, indicating variability between source studies, precluding correlating amygdala effect sizes with hippocampal effect sizes and weakening the conclusions that can be drawn from the hippocampal portion of our meta-analysis.
In contrast to our findings of no significant volume differences in the left and right amygdala between patients with PTSD and comparison groups, Karl et al.
5 found no between-group differences in right amygdala volume in their meta-analysis of amygdala volumes in patients with PTSD relative to both comparison subjects not exposed to trauma (seven studies, 320 subjects) and to trauma-exposed subjects without PTSD (six studies, 213 subjects); however, the meta-analysis did find a smaller left amygdala in patients with PTSD relative to healthy comparison subjects not exposed to trauma (effect size=−0.14). After exclusion of two studies, the left amygdala was also smaller in patients with PTSD relative to trauma-exposed comparison subjects without PTSD (effect size=−0.22). Although not statistically significant and associated with a relatively small effect size (Hedges’
g =−0.290, p=0.061), our finding of a nonsignificant numerical trend for a smaller left amygdala in patients with PTSD relative to healthy subjects not exposed to trauma argues for additional research to clarify further amygdala volume in patients with PTSD. The meta-analysis of Karl et al.
5 included pediatric data, whereas our study included only data from adults, a methodological difference that could account for at least part of the differences in the left amygdala results. In addition to underscoring the importance of analyzing the amygdala volume in adults with PTSD separately from children with PTSD, our numerical trend for a smaller left amygdala in patients with PTSD relative to healthy subjects not exposed to trauma, but not to healthy, trauma-exposed subjects, emphasizes the importance of the type of comparison group used in amygdala volumetric studies in PTSD.
Apparently normal amygdala volumes do not necessarily preclude functional abnormalities in the amygdala in patients with PTSD. As a case in point, the results of a functional neuroimaging meta-analysis in patients with PTSD found evidence of amygdala abnormalities, particularly in the left amygdala, where two distinct clusters of abnormal function were identified: a ventral anterior hyperactivation cluster and a dorsal posterior hypoactivation cluster.
47 The distinct functional expression within the subregions of the amygdala highlights the need for more focused studies of PTSD with high-resolution structural MRI technology.
The comparisons between amygdala volumes in healthy, trauma-exposed subjects and in those not exposed to trauma found no differences. As such, the available findings suggest that exposure to trauma alone may not be associated with volume differences in the amygdala, in contrast to preliminary findings that raise the possibility that trauma exposure in the absence of PTSD may be associated with smaller hippocampal volumes relative to comparison subjects without a history of trauma exposure.
8The relatively small number of studies (nine) limits the generality of the finding of a preserved amygdala volume in patients with PTSD. Despite the prominent role of the amygdala in stress physiology and its structural remodeling in response to stress,
48 surprisingly few amygdala volumetric studies in PTSD have been done compared with studies investigating hippocampal volume. Hence, our results should be viewed as preliminary findings that may be highly susceptible to future studies but nevertheless serve to generate additional hypotheses about neuroanatomical differences in patients with PTSD relative to comparison subjects, as well as relationships between the amygdala and PTSD. Because of the relatively few studies available for analysis, we were unable to classify the available studies into subgroups such as gender and age of the subjects, trauma type, duration of trauma exposure, severity of trauma, and time since trauma—variables that may affect neuroanatomical outcome.
5 –
8 In fact, the nine studies included in our evaluation showed considerable clinical heterogeneity. For example, Wignall et al.
14 studied patients 158 days on average after trauma exposure, whereas subjects in other studies
22,
24,
25 had been exposed to trauma decades before brain imaging occurred. Only longitudinal studies or meta-analyses with access to a sufficient number of subjects at differing times after trauma exposure and PTSD onset can unravel the effects of age at and chronicity of trauma exposure on amygdala volume in patients with PTSD. Furthermore, as shown in
Table 1, the source studies in our analysis showed considerable variation in gender, age, type of trauma, and duration of trauma exposure, differences that may obscure volumetric nuances in the amygdala and lead to inconsistent findings. Consideration of sociodemographic factors, too, may well be important in volume studies of the amygdala, particularly given the findings of Vythilingam et al.
49 that significantly lower IQ scores in deployed veterans with PTSD, deployed veterans without PTSD, and nondeployed reservists relative to healthy comparison subjects might contribute to deficits in hippocampal volumes.
As with all meta-analyses, a concern is that the results may be skewed by publication bias. The potential for publication bias may be partially mitigated in this study because most of the findings of amygdala volume came from studies primarily reporting findings of hippocampal volume. Nonetheless, publication bias may still exist in that negative studies of hippocampal volume containing incidental amygdala data might not have been published. Statistical tests evaluating the potential for publication bias in this study, such as the classic and Orwin’s fail-safe N analysis, showed little evidence of publication bias, further supporting the finding of preserved amygdala volume in PTSD.
In conclusion, we found in this meta-analysis that there were no differences in amygdala volume in patients with PTSD compared with healthy, trauma-exposed comparison subjects without PTSD and healthy comparison subjects who were not exposed to trauma, in marked contrast to the numerous studies reporting hippocampal volume deficits in PTSD. We did find a possible trend for a smaller left amygdala in patients with PTSD relative to healthy, trauma-unexposed comparison subjects. Furthermore, in all three groups, a significantly larger right than left amygdala was found, suggesting an overall asymmetrical lateralization in amygdala volume that is preserved after trauma exposure and in PTSD.