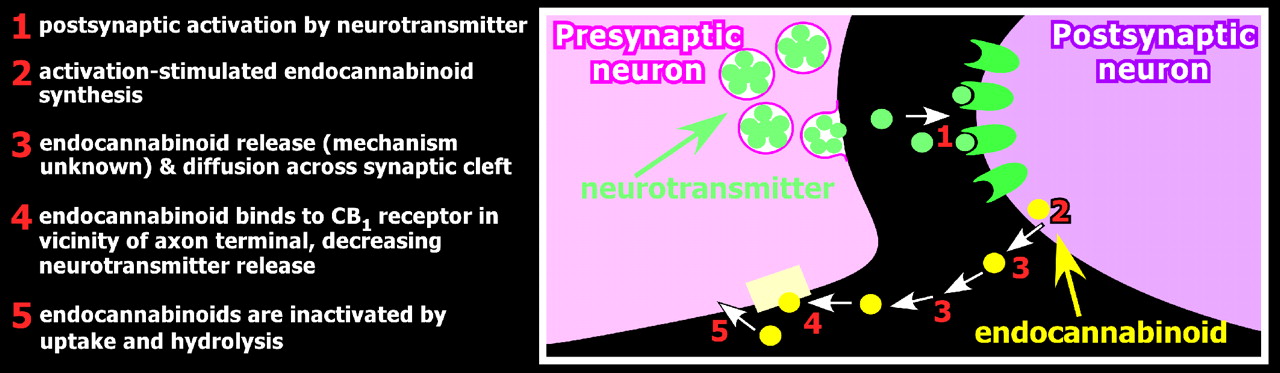
The endocannabinoid system participates in multiple brain circuits implicated in neuropsychiatric conditions such as those modulating stress reactions, learning, and extinction of fear, emotional regulation, and reward processes.
31,
32 CB
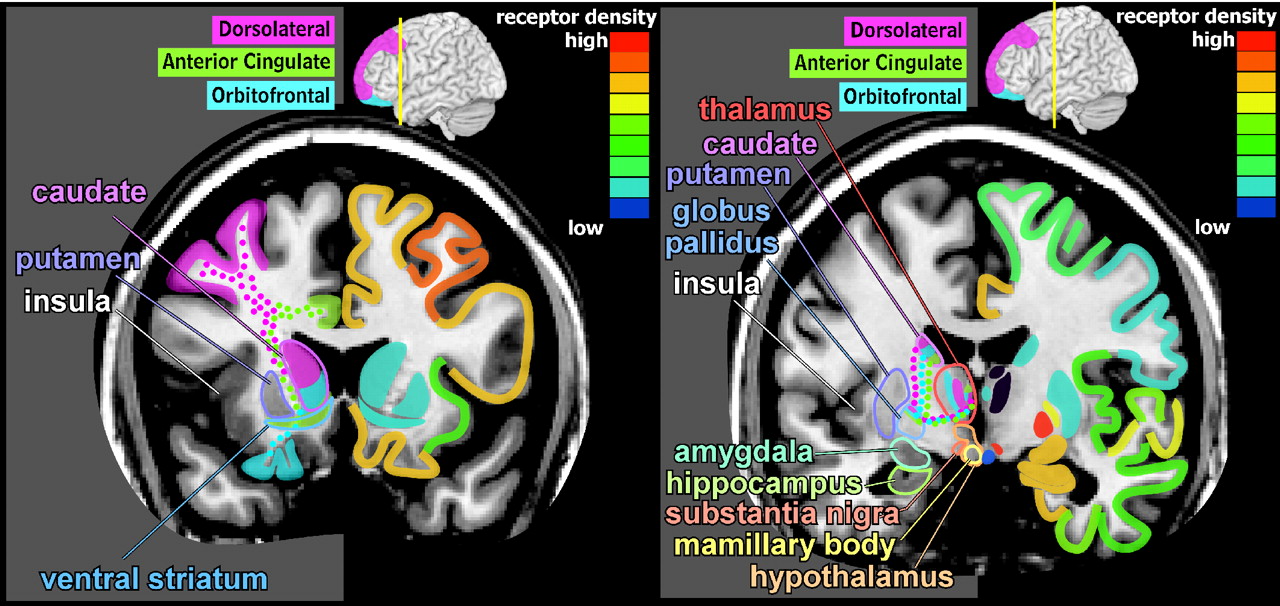
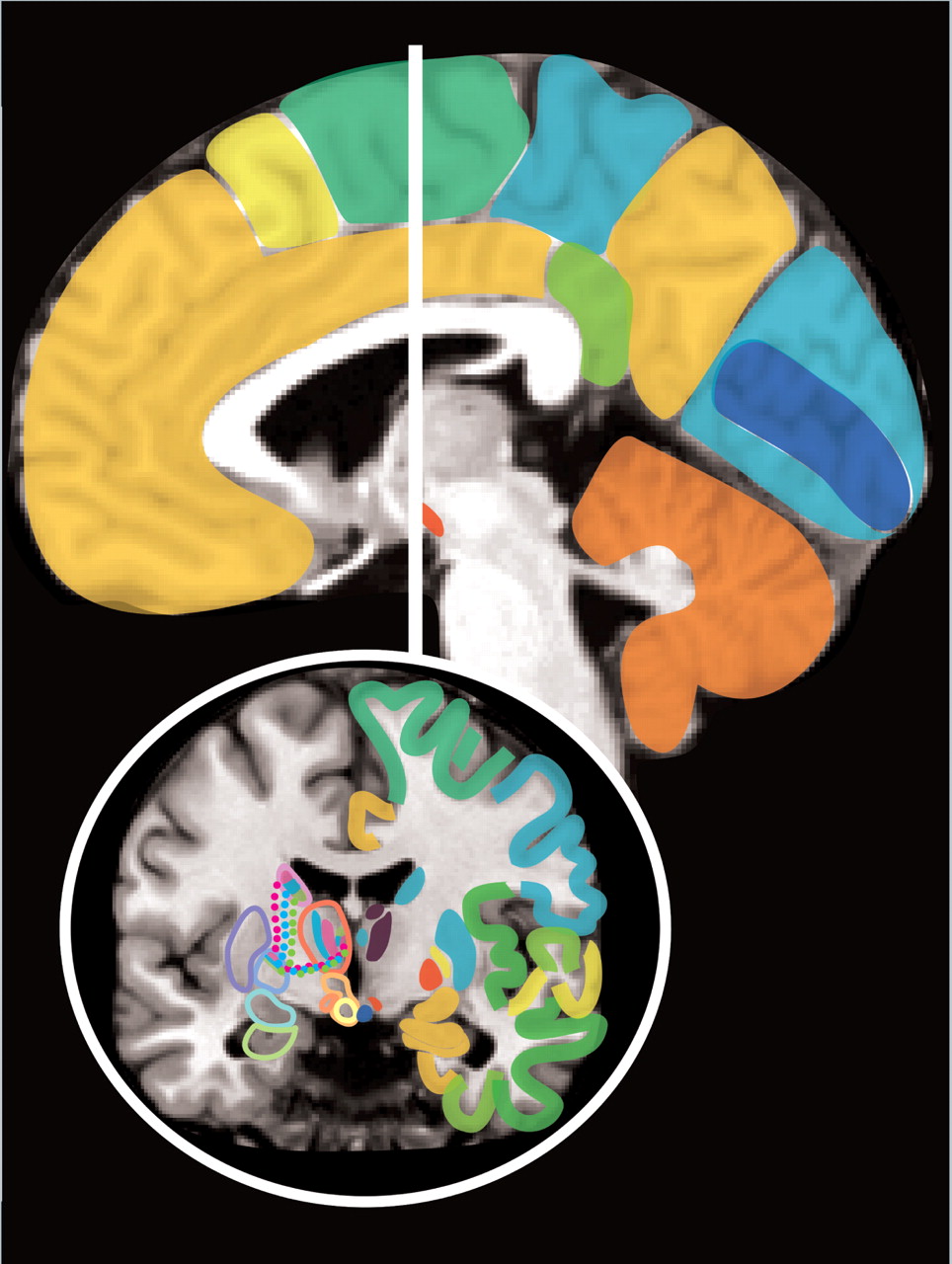
1 receptors are found in many areas involved in regulation of the stress response including the paraventricular nucleus (PVN) of the hypothalamus, corticotroph cells in the pituitary, adrenal glands, and limbic-related areas of the brain.
30 Endocannabinoids inhibit the hypothalamic-pituitary-adrenal (HPA) axis and may well provide an ongoing basal level of inhibition. During acute stress, corticotrophin releasing factor is released into the portal system by neurons in the paraventricular nucleus. Corticotrophin releasing factor (CRF) induces release of adrenocorticotrophic hormone from the anterior pituitary. Adrenocorticotrophic hormone stimulates production of glucocorticoids (e.g., corticosterone) in the adrenal gland. Glucocorticoids, in turn, inhibit release of corticotrophin releasing factor in the hypothalamus and adrenocorticotrophic hormone (ACTH) in the pituitary. Negative feedback in the hypothalamus is mediated by glucocorticoid-stimulated synthesis and release of endocannabinoids within the paraventricular nucleus.
10,
25,
30 Thus, endocannabinoids are released in response to activity in the hypothalamic-pituitary-adrenal axis and serve to bring it back toward its baseline (prestress) state.
10Animal studies indicate that neither acute stress nor chronic predictable stress (which will habituate) alter CB
1 receptor density or affinity in the brain.
33 Both chronic unpredictable stress (which does not habituate) and chronic administration of corticosterone, on the other hand, decrease CB
1 receptor density in the hippocampus.
33 These stress conditions also differentially alter the content of 2-AG and anandamide of many brain regions. Some studies support the theory that a progressive increase of 2-AG and decrease of anandamide within limbic-related brain areas (e.g., medial prefrontal cortex, limbic forebrain, amygdala, hypothalamus) may, in part, mediate behavioral habituation to chronic predictable stress.
33 An opposite pattern (increased anandamide, decreased 2-AG) is seen in the ventral striatum, which may have implications for endocannabinoid-mediated facilitation of reward.
33 An antidepressant-like effect (as indicated by enhanced stress-coping behaviors and decreased anhedonic behaviors), has been reported for both compounds that directly activate CB
1 receptors and those that prolong the action of naturally released endocannabinoids (e.g., inhibit uptake, inhibit hydrolysis).
28 Animal studies of social defeat stress (which produces symptoms of anxiety and depression) indicate that it decreases CB
1 receptor-mediated inhibition of GABA (but not glutamate) neurotransmission in the striatum.
34 This change occurs as a result of stress-induced increases in glucocorticoids, and can be reversed by both natural rewards (e.g., access to sucrose) and administration of drugs with rewarding properties (e.g., cocaine).
34 An important role for the endocannabinoid system in reward-related processes is likely. CB
1 receptor-activation modulates dopamine signaling in both the ventral tegmental area and the ventral striatum.
13,
29 CB
1 receptors also participate in LTD at glutaminergic synapses in both dorsal and ventral striatum.
29 It has been proposed that the endocannabinoid system provides the common neurobiological mechanism underlying both the rewarding aspects of drugs of abuse and relapse, suggesting that blockade of CB
1 receptors may have therapeutic potential.
13,
35 Studies also support the involvement of the endocannabinoid system in extinction of conditioned fear.
10,
25,
28 Endocannabinoid content of the amygdala is increased following exposure to the conditioned stimulus (e.g., tone previously paired to foot shock).
25,
28 Removal of the influence of CB
1 receptors (either by pharmacological blockade or by genetic manipulation) impairs extinction of conditioned fear.
27,
28 Extinction is enhanced by administration of compounds that directly activate CB
1 receptors or prolong the action of naturally released endocannabinoids (e.g., inhibit uptake, inhibit hydrolysis).
10,
27,
28There is growing evidence that another important function of the endocannabinoid system is regulation of energy balance, both in terms of influencing appetite and by modulating metabolism.
36 –
39 Both central and peripheral actions are likely to be involved. CB
1 receptors are present in hypothalamic areas (e.g., mediobasal, paraventricular, lateral) integral to balancing energy intake with energy expenditure.
38 Endocannabinoid levels in the hypothalamus are increased by starvation and decreased by food intake.
36 In rats, food intake is increased following administration of endocannabinoids to either the hypothalamus or mesolimbic forebrain.
36 In addition, studies in both humans and animals have found that that blockade of CB
1 receptors normalizes several metabolic parameters that are risk factors for metabolic syndrome (e.g., decreased triglycerides and insulin resistance, increased high-density lipoprotein cholesterol) in excess of what would be expected from weight loss alone, supporting a role in glucose homeostasis and adipose tissue metabolism.
36 –
40 Research suggests that this system may be overactive in conditions such as obesity and hyperglycemia.
36,
38,
39,
41 CB
1 receptor activation increases fatty acid synthesis in the liver as well as lipid synthesis by adipose tissue, and obesity is associated with increases in CB
1 receptors in both adipose tissue and skeletal muscle.
36