S everal studies have demonstrated that major depressive disorder is associated with impairment in a wide range of neuropsychological domains, including verbal and nonverbal memory, selective and sustained attention, processing speed, and executive function. Executive dysfunction may present with impairments in cognitive flexibility, planning, sequential problem-solving, monitoring, and feedback.
1 –
5 Neuroimaging studies using single photon emission tomography and positron emission tomography have consistently demonstrated decreased regional glucose metabolism and/or regional cerebral blood flow in the dorsolateral prefrontal cortex, the anterior cingulate cortex, the thalamus, the striatum, the basal ganglia, and the hippocampus.
6 Conversely, increased glucose metabolism and regional cerebral blood flow have been observed in the ventrolateral and orbital prefrontal cortex and in the amygdala.
7,
8 It is speculated that impairment in widely distributed brain networks, including the prefrontal cortex, may cause executive dysfunction in patients with major depressive disorder.
6Despite successful treatment, some recent studies have documented that executive dysfunction remains unresolved even after remission of depressive episodes.
9,
10 Results to date are mixed and inconsistent regarding whether executive dysfunction in patients with major depressive disorder resolves following remission.
In addition to depressive episodes, the aging process may also affect executive function. Lockwood et al.
4 demonstrated that older depressed adults demonstrated the poorest performance on tasks that required set shifting, problem solving, and the initiation of novel responses. Furthermore, several recent studies demonstrated that cognitive dysfunction in elderly patients with major depressive disorder persists after remission.
11 –
15 Patients with late-life depression may frequently show multiple small lacunar/cerebrovascular lesions, suggesting that vascular factors are associated with mood changes. Because subcortical vascular lesions further deteriorate frontal-subcortical connections, executive dysfunction observed in depression is likely to be enhanced in elderly patients.
Although a number of researchers documented cognitive dysfunction in major depressive disorder, no studies have directly compared cognitive dysfunction in elderly and adult patients with major depressive disorder after remission. The aim of our study was to examine executive function in remitted major depressive disorder patients by age, and to compare elderly patients with younger patients directly to determine whether patients with late-life depression differ cognitively from adult patients during the remission phase. We evaluated executive functions using the Behavioral Assessment of the Dysexecutive Syndrome (BADS).
16 The BADS is a test battery aimed at predicting everyday problems that arise from the “dysexecutive syndrome,” a term that is used to refer to varied groups of deficits resulting from diverse etiologies, different locations, and variable extents of abnormalities.
17 The BADS is characterized to assess an individual’s problem-solving ability in various everyday situations, thereby providing a measure for assessing executive functions with ecological validity. We hypothesized that major depressive disorder patients would present with executive dysfunction even in the remission phase when compared with healthy comparison subjects. In addition, we postulated that patients with late-life depression are more impaired in executive function compared with adult major depressive disorder patients.
METHODS
Subjects
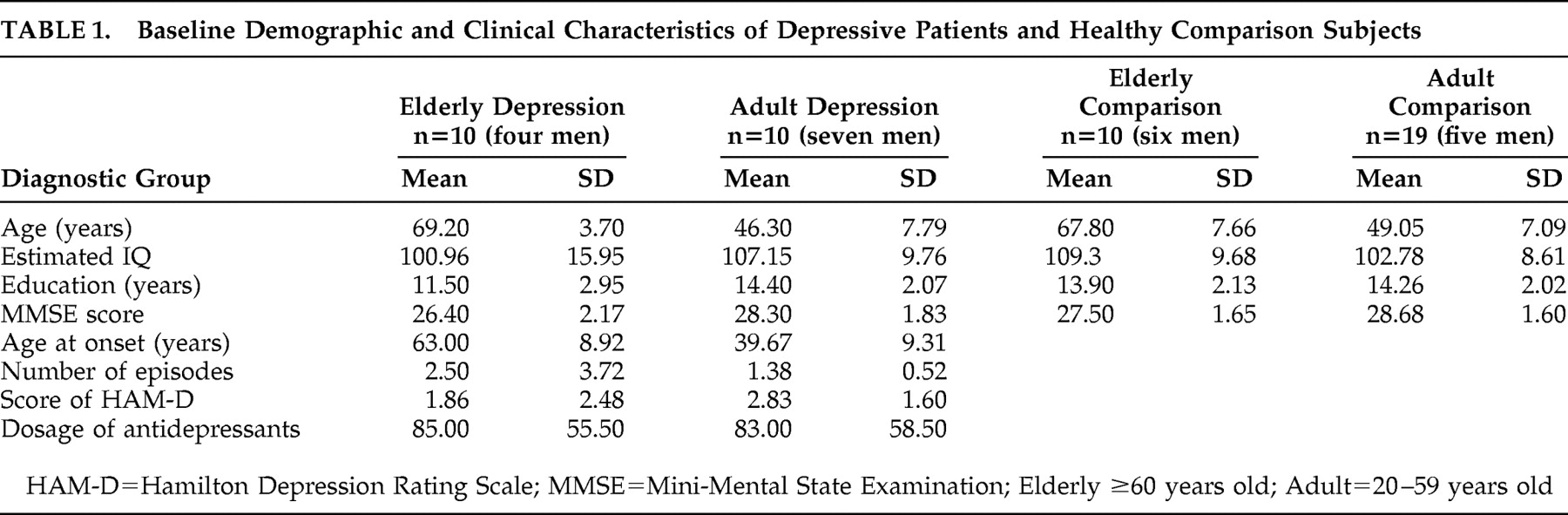
Ten adult patients (20–59 years old) and 10 elderly patients (≥60 years old) with major depressive disorder were recruited for participation through Shimodate Hospital and Juntendo Koshigaya Hospital. Twelve participants were inpatients (seven adult and five elderly), and eight participants were outpatients (three adult and five elderly). Diagnoses were made based on the DSM-IV, and all patients were in remission at the time of testing. Depressive symptoms were evaluated by experienced psychiatrists (HB, IN) using the 21-item Hamilton Depression Rating Scale score, and remission was defined as a score of 7 points or below. All patients were treated with one or two antidepressants, including paroxetine, fluvoxamine, milnacipran, and tricyclic antidepressants. The mean dosages of drugs as imipramine equivalents were not different between adult and elderly patients (
Table 1 ). Some patients were taking benzodiazepine derivatives as well.
Patients were excluded if they had a history of other psychiatric disorders including manic episodes, psychotic features, epilepsy, and substance abuse; a history of neurological disorders including head trauma, brain tumor, and cerebrovascular disease; or a history of ECT. In addition, we excluded those who presented with clinical evidence of dementia or Mini-Mental State Examination (MMSE) score less than 24, and we excluded those with severe physical illnesses in general including myocardial infarction and diabetes mellitus. Adult and elderly healthy comparison subjects were recruited from the community. Those who had a history of psychiatric and/or neurological disorders, including substance use, were excluded. All participants signed informed consent statements.
Participants were grouped by diagnosis (depression versus comparison) and current age (adult versus elderly). Each patient group was equated to a corresponding comparison group for age, education, and intelligence (Mann-Whitney U test, p>0.10). The demographic and clinical characteristics of the four groups are summarized in
Table 1 .
Measures
Neuropsychological assessment of the participants was performed at either Shimodate Hospital or Juntendo Koshigaya Hospital. Hospitalized major depressive disorder patients were examined on discharge after remission. Intelligence was recorded as estimated IQ, using the Japanese National Adults Reading Test,
18 which is the functional equivalent of the widely used JART.
Executive functions were measured by BADS,
16 the total profile score of which was obtained from the summation of each of six subtests, as follows.
The Rule Shift Cards test is believed to reflect cognitive flexibility. The Action Program test examines the ability to solve a close-ended, sequential problem. The Key Search test examines the ability to solve an open-ended problem. The Temporal Judgment test examines the ability of cognitive estimation. The Zoo Map test examines the ability to plan and use feedback in problem solving. The Modified Six Elements test is believed to test the ability to plan, organize, and monitor multitasking behavior.
Statistical Analysis
Although there were no statistically significant differences in education and estimated IQ between groups, we thought that the results could be confounded by their effects. Accordingly, 2 (age: adult versus elderly) × 2 (diagnosis: depression versus comparison) analysis of variance with covariance of education and estimated IQ (ANCOVA) was used to compare the four groups. The significance level was set at 0.05.
RESULTS
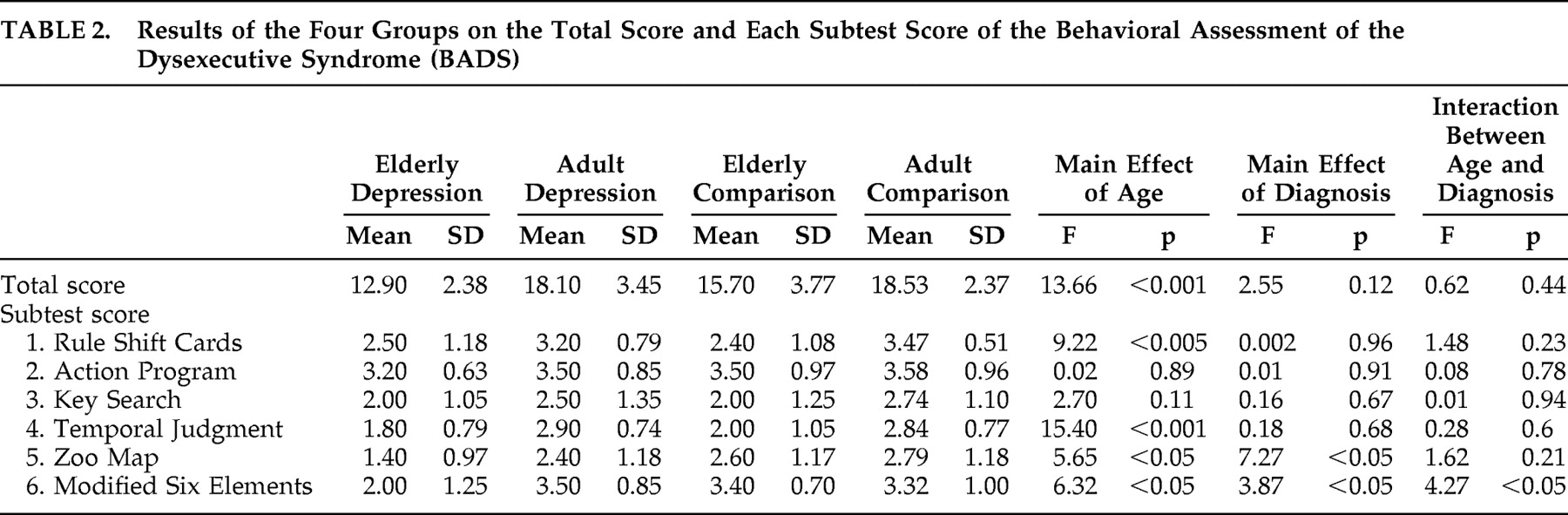
Means and standard deviations of the total and subtest scores of the BADS for the two patient groups and two comparison groups are shown in
Table 2 . The main effects of age (adult versus elderly) and diagnosis (depression versus comparison subjects), as well as the interactions between age and diagnosis, are also shown in
Table 2 . For the total score, the main effect of age was found to be significant (F=13.66, df=1, 45, p<0.001), indicating that elderly subjects (elderly depression patients and elderly comparison subjects) performed significantly lower than adult subjects (adult depression patients and adult comparison subjects). The main effects of diagnosis, as well as the interactions between age and diagnosis, were not significant.
The following results were obtained for each subtest of the BADS. For the Rule Shift Cards and the Temporal Judgment tests, the main effect of age was significant, but the main effect of diagnosis or the interaction between age and diagnosis was not. For the Action Program and Key Search tests, none of the results reached significance. For the Zoo Map test, the main effects of age and diagnosis were significant, but the interaction between age and diagnosis was not. This indicates that elderly subjects performed more poorly than adult subjects, and the major depressive disorder patients performed more poorly than healthy comparison subjects. Finally, for the Modified Six Elements test, both the main effects of age and diagnosis were significant. In addition, a statistically significant interaction between age and diagnosis was obtained, suggesting that the elderly depression group performed more poorly compared with the other three groups.
DISCUSSION
The present study provided two major findings concerning executive dysfunction in major depressive disorder, as indexed by BADS. For subtests 1 (Rule Shift Cards) and 4 (Temporal Judgment), together with the total score, the overall aging effect was remarkable, whereas the diagnosis of depression per se did not seem to impair executive functioning. These results suggest that the abilities of cognitive flexibility and cognitive estimation may decline due to aging. We must withhold strong conclusions concerning negative results for a depression diagnosis on the total score and subtests, as the sample size is small.
On the other hand, for subtests 5 (Zoo Map) and 6 (Modified Six Elements), the effects of diagnosis as well as aging were remarkable. Even in remission, major depressive disorder patients preferentially showed lower performance than healthy subjects in these two subtests of the BADS. Specifically, patients with late-life depression in remission showed significantly lower performance than both adult depression patients and healthy comparison subjects in the Modified Six Elements subtest. Burgess et al.
19 argued that multitasking tests such as the Modified Six Elements subtest might simulate a patient’s everyday situations involving planning and organization, thereby providing an index for ecologically valid executive functioning. In their paper, it was proposed that the following three cognitive components work together to facilitate multitasking: retrospective memory, prospective memory, and planning. Based on their focal brain-damaged patients’ performances, Burgess et al.
19 suggested that the anterior cingulate cortex plays a part in retrospective memory demands, while Brodmann’s area 10 and the immediately adjacent areas play a part in prospective memory components and the dorsolateral prefrontal cortex in planning components. We speculate that residual inability to plan, organize, and monitor multitasking behavior may partially account for poorer social functioning of patients with late-life depression even in the remitted stage. The relation between residual executive dysfunction and social malfunctioning in late-life depression should be addressed in future research.
Brain areas with decreased metabolism and/or perfusion in major depressive disorder have been reported to involve the dorsolateral prefrontal cortex and anterior cingulate cortex. In addition, such hypometabolism/hypoperfusion is state-independent and may remain even during the remission phase.
20 Therefore, we speculate that remitted patients with late-life depression may have some pathology in these brain areas. We conclude that dysfunctions in frontal networks remain unresolved even in the remission phase of late-life depression. Such network dysfunctions may represent an endophenotype of depression in elderly cohorts. Although preliminary, the present study suggests that an impact of late-life depression exacerbates executive function even in the remitted stage.
There are several limitations in our study. First, patients were treated with antidepressants, which may exert deleterious effects on cognition. Accordingly, drug-free euthymic patients should be included in future investigations. Second, we only assessed memory with MMSE. It was possible for elderly subjects to show memory impairment which could not be identified with MMSE regardless of depression status, and such subtle memory impairment may affect executive function. Another limitation is that this study only concerns behavioral measures and that neuroimaging information, including MRI scans, was unavailable for some of the patients. Additional research is warranted to investigate the relationship between executive dysfunction and specific functional brain lesions in major depressive disorder.
CONCLUSION
We found that executive dysfunction remains even in the remission phase of major depressive disorder. Although overall executive function, as indexed by the total score of the BADS, is affected by the aging process, remitted major depressive disorder patients still presented with residual impairment in particular subtests of executive function. Specifically, the Modified Six Elements subtest was sensitive to the dysfunction of remitted patients with late-life depression. We speculate that patients with late-life depression may have residual pathology in several brain areas, including the anterior cingulate, anterior medial prefrontal areas, and the right dorsolateral prefrontal cortex.
Acknowledgments
Kanako Baba carried out the study, supervised the data collection, and wrote the paper. Hajime Baba designed the study, analyzed the data, and assisted with writing the article. K. Baba and H. Baba contributed equally to this work. Iwahide Noguchi and Reiko Arai evaluated the depressive subjects. Toshihito Suzuki analyzed the data. Masaru Mimura chose the statistical design and assisted with writing the article. Heii Arai was responsible for statistical design of the study and for carrying out the statistical analysis.