Impaired social interactions are a key characteristic of schizophrenia. It is tempting to relate this deficit to the well-known inability of patients with schizophrenia to recognize others' emotions.
1 Although, there is still no consensus regarding the nature of this inability,
2 gender does not seem to be a key factor.
3 Also, when using Ekman's classification of primary emotions, no differences seem to appear between various emotions.
4,5 It does not appear that some emotions are more affected than others.
6Patients with schizophrenia are not only deficient in recognizing facial emotions; they are also impaired in producing them. Flat affect is a frequent symptom in schizophrenia (66% of patients).
7 This symptom has been extensively reported in the literature, under a wide range of contexts and stimuli (for reviews: see Kring and Moran
8 and Morris et al.
9), even in drug-naïve patients.
10 However, a review of today's literature shows that no research has studied the ability of patients with schizophrenia to evaluate their own self-generated facial expressions. The present study aims to bring a new light to the understanding of evaluation of facial emotions in schizophrenia.
MATERIALS AND METHODS
Subjects
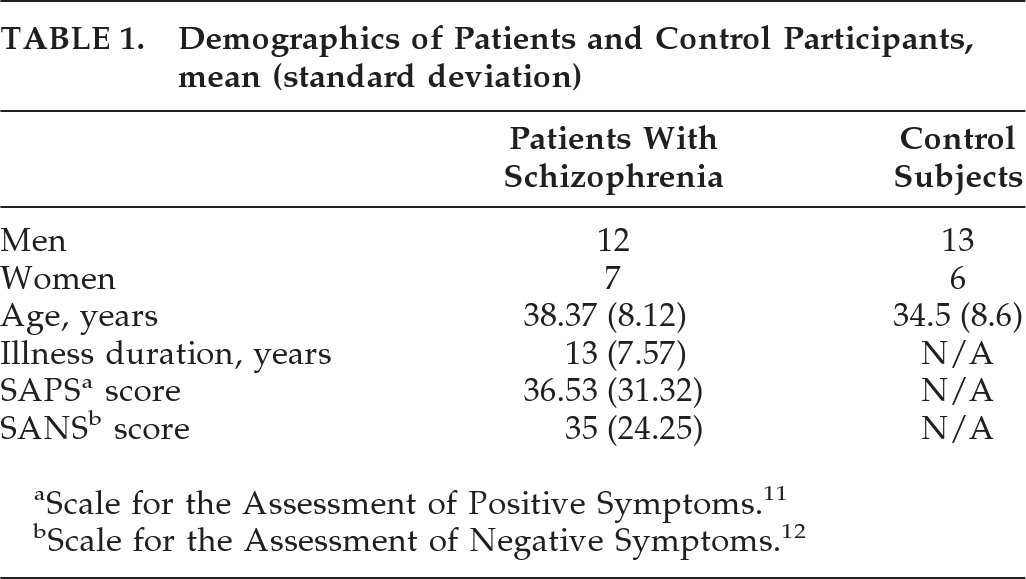
Nineteen patients with schizophrenia were enrolled in the study, recruited from Le Vinatier Hospital. There were all inpatients of the psychiatric unit. All patients met DSM-IV criteria for schizophrenia without other concurrent diagnosis. All of the patients were taking antipsychotic medication monotherapy (without change in the 2 preceding weeks), were clinically stable at the time of the experiment, and had been so for at least 4 weeks. A trained clinician (CD) administered the SAPS (Scale for the Assessment of Positive Symptoms)
11 and SANS (Scale for the Assessment of Negative Symptoms)
12 measurements to obtain ratings for positive and negative symptoms.
Healthy participants (N=19) were free of any Axis I diagnosis, Axis II cluster (schizotypal, schizoid, or paranoid personality disorder) and family history of psychiatric illness. Exclusion criteria included mood disorders (manic or depressive symptoms), neurological disorders, and any medical condition that might alter cerebral functioning. Healthy participants were matched to patients by age, gender, ethnicity, and education. Written informed consent was obtained from all participants after complete information was given.
Twelve healthy individuals also volunteered to rate the expressions produced by the patients and control subjects. These independent raters (mean age: 25.8 [standard deviation{SD}]: 11.6 years) were eligible for the study only if they did not know the subjects tested in the first phase of the experiment and did not work in a hospital, a mental health institution, or a research center.
Procedure
The study was divided into two phases. The first phase was a Production phase: participants had to produce facial emotions in response to a visual model or a written sentence. The second phase (Rating) began after 2 months: participants had to rate the expression they had produced in the first phase. Twelve independent raters also performed the rating of these expressions.
Production Phase
All participants were seated 60 cm. in front of a computer screen, above which there was a digital video camera (Sony HDR-SR1E). The camera recorded, uninterruptedly, the face of the subjects. The experimenter stood 1.50 meters behind the participant and could not see his or her face. This phase was divided into two separate tests:
1.
Imitation of facial expressions: For this first test, subjects viewed six photographs of facial expressions and had to imitate them; 12 black-and-white pictures (19 cm. high and 13 cm. wide), showing faces expressing five emotions (happiness, anger, disgust, fear, and sadness) and neutrality were used. The expressive pictures were taken from Ekman's picture set.
4 The neutral pictures were taken from a database used and validated in a previous experiment.
13 The pictures were randomly presented across subjects. The instructions were to “Imitate the facial expressions you are about to see as an actor would do and do so only with your face.” When the subjects were satisfied with their imitation, they had to rate the intensity of the expression they had just produced on a scale from 1 (very low intensity) to 5 (very high intensity).
2.
Production of facial expressions from a written command (mime): For the second test, the participants saw a sentence on the screen defining an emotion and its related context (for example, fear: “A burglar enters your apartment; you are afraid.”). They had to mime the emotion “as an actor would do, and only with their face.” The emotions were presented to each participant in the same order as the one used for the first test. After each mime, the subjects had to rate the intensity of their expression on the same scale as the one used for the imitation test.
Recognition Phase
Evaluation of Self-Generated Facial Expressions
Two months after Phase 1, the participants were shown the 12 videos of their imitations and mimes. The videos lasted between 1 sec. and 5 sec., depending on the length of the emotional production. The 12 videos were presented in a random order. After each video, a rating screen appeared with five numbers (1 to 5), and the participants had to enter the perceived intensity of their own expressions on the keyboard (1: low; 5: high). Then, they had to determine which emotion was displayed in the video. For each trial, the list of possible emotions to choose from (happiness, anger, disgust, sadness, fear, neutrality) was displayed on a screen that appeared just after the validation of the intensity rating. The subject selected his or her response by using the keyboard. They were told at the beginning of the experiment that a given emotion could occur more than once. In the final step, the intensity rating screen was presented again, and participants were asked to report how confident they were about their recognition (1: not sure at all; to 5: absolutely sure). There was no time constraint, and the participants were free to take as much time as they wanted.
Evaluation of Emotional Productions by Independent Raters
Twelve raters viewed the facial expressions collected from all participants in Phase 1. The 456 videos collected from the control subjects and patients were randomly presented in two sessions of 45 minutes each (228 videos/session). These sessions took place on two different days. The videos were divided between the two sessions in such a way that 1) each emotion was presented the same number of times in each session; 2) each subject appeared the same number of times; and 3) there was the same number of videos associated with the imitation and mime conditions. The rating procedure (intensity, nature of the emotion, confidence) was the same as the one described above for the self-evaluation task.
Data Analysis
We performed 2×2×6 ANOVAs, with Group (Patients, Controls) as a between-subject variable and Production mode (Imitation, Mime) and emotion (Happiness, Anger, Disgust, Fear, Sadness, Neutrality) as within-subject variables. Fisher's least significant different test (Fisher's LSD) was used for post-hoc comparisons of the mean.
RESULTS
The demographic characteristics of the patients and control subjects are presented in
Table 1.
Production Phase
The self-reported ability of patients and control subjects to produce facial expressions was not statistically different (group factor, main effect, and interactions, all p>0.05; F [1, 60]=1.66). All participants rated their expressions as more intense in the Mime condition than in the Imitation one (3.4 versus 3.1; F [1, 36]=11.76; p<0.01). The main effect of emotion was also significant (F [5, 180]=28.65; p<0.0001), indicating that some expressions were more difficult to produce than others (Sadness and Neutral condition).
Recognition Phase
Intensity
The ability of the patients and control subjects to rate the intensity of the facial expressions they had performed 2 months earlier was not statistically different (group factor, main effect, and interactions: F [1, 36]=0.94).
Accuracy/Confidence
The main effect of the group factor was significant (F [1, 36]=18.96; p<0.001), indicating that the patients were impaired at recognizing self-generated facial expressions (correct recognitions: Patients: 49.6%; Controls: 75.4%).
For confidence, a significant interaction was found between emotion and group (F [5, 180]=4.61; p<0.001). This interaction was due to the fact that the control subjects had more difficulties recognizing happiness than the patients (Fisher's LSD, all ps<0.001). However, for a given emotion, no significant difference was found between patients and controls (Fisher's LSD, all ps>0.05).
Ratings During Recognition Phase by Independent Judges
Intensity
The main effect of group was significant (F [1, 36]=13.70; p<0.001). The independent judges rated the facial emotions expressed by Patients as less intense than those expressed by Controls (2.7 versus 3.1).
Accuracy/Confidence
The main effect of group was significant (F [1, 36]=11.16; p<0.01). The independent judges were less accurate at recognizing the emotions expressed by the Patients than those expressed by the Controls (correct answers: 52.0% versus 65.4%). For confidence, the main effect of the group factor was significant (F [1, 36]=13.06; p<0.001). The independent judges were less confident about their answers for Patients than for Controls (3.3 versus 3.6, respectively). An interaction was found between group and emotion (F [5, 180]=2.39; p<0.001). It accounted for the fact that the magnitude of the differences observed between the Controls and the Patients was larger for some emotions than for others.
DISCUSSION
The aim of the present study was to bring new light to the understanding of how patients with schizophrenia assess self-generated facial emotions.
This study shows that patients with schizophrenia are impaired, as compared with control subjects, at recognizing their own facial expressions on videos. Interestingly the patients are totally unaware of this impairment, and they are as confident as healthy subjects in their ability to recognize these expressions. These results are in line with previous observations showing that patients with schizophrenia are dramatically impaired at recognizing the facial expressions performed by others.
14One explanation that can be given is that the inability of the patients to recognize their own expression could be related, at least partially, to their lack of facial expressiveness. Indeed, in agreement with previous studies, we found that patients with schizophrenia were significantly less expressive than control subjects.
15–17 Strikingly, independent judges 1) rated the patients' facial expressions as less intense than the expressions produced by control subjects; 2) were less accurate at recognizing emotions expressed by the patients with respect to the controls; and 3) were less confident in their responses about the patients' expressions.
Although patients with schizophrenia have difficulty in expressing their emotion at a facial level, they report experiencing as much positive and negative emotion as the control subjects.
7 As a consequence, it seems that the lack of facial expressiveness of patients misrepresents their actual emotional experience. Consistent with this idea, we showed that the patients were as confident as the control subjects in their ability to express the emotions they wanted to convey and recognize these emotions on videos. However, a major difference between the controls and the patients lies in the fact that the control subjects were capable of recognition when they were unsure about an expression. This was not the case for the patients, who reported the same level of confidence for their right and wrong recognitions.
Thus, it seems that the patients acted as if they had a fixed confidence level for all their judgments. Overall, these results are consistent with recent data showing that preserved implicit emotion contrasts with impairments to explicit emotion-classification in schizophrenia.
18 Thus, the major result of our study is that patients with schizophrenia seem not to be aware of their impairment in facial expressiveness. Such an unawareness of impairment has also been reported in several domains, for example, in assessment of their cognitive impairment level,
19 functional disabilities,
20 and decision-making skills.
21 This lack of awareness, that could hypothetically be caused by impaired self-monitoring,
22 may then be a core aspect of schizophrenia.
A limitation of the present study lies in the fact that we did not considered other components of emotional expression, such as voice pitch or hand/body gestures. These dimensions could be worth considering in further studies. In the same way, it could be important to investigate self-recognition in other psychiatric pathologies, including depression. Indeed, depressed patients have been reported to be as impaired as patients with schizophrenia in posed emotional expression.
This being said, one may also argue that our results were affected by the fact that the subjects had different (uncontrolled) cultural backgrounds. Although plausible in theory, this hypothesis seems unlikely, considering that all participants lived in France and that the six facial expressions assessed in our study are known to be cross-culturally comparable. In the same way, one may claim that our conclusions were affected by the fact that the patients were treated with antipsychotic medication. Again, this does not seem to be a likely possibility, considering that the lack of expressiveness in patients with schizophrenia is independent of antipsychotic treatment,
10 especially for the second-generation antipsychotic monotherapy that was used in the present study.
In summary, patients with schizophrenia show a generalized impairment in their ability to recognize and express facial emotions. This deficit is likely to have dramatic consequences on interpersonal relationships. It may be a partial explanation for the social-cognition disabilities of these patients. The observed lack of facial expressiveness among the patients contradicts their perception that their emotional expressions are normal. This may be one aspect of the expression of Bleuler's
Spaltung.
23 Developing cognitive remediation strategies that would aim specifically at the impairment of expressing and recognizing facial expressions could be a promising mode for the treatment of schizophrenia.
24,25