To the Editor: Brain tumors may present with multiple psychiatric symptoms, such as depression, anxiety disorders, panic attacks, personality change, abulia, auditory and visual hallucinations, mania, or memory difficulties. In the present study, we discuss a case of a 50-year-old man who was treated for 7 years for anxiety disorder and depression but did not respond to treatment. At that period, he did not develop any major neurological signs or symptoms. When he complained of headache, he was examined by a neurologist, and MRI scans (MRIs) were performed. MRIs of the brain revealed a glial tumor in the left temporal lobe, and he underwent surgical treatment and subsequently received chemotherapy and radiotherapy.
We conclude that brain tumors can be neurologically silent and only present with psychiatric symptoms. Therefore, we emphasize the need for brain imaging studies in a patient with resistance to psychiatric drugs and without neurological signs or symptoms.
Case Report
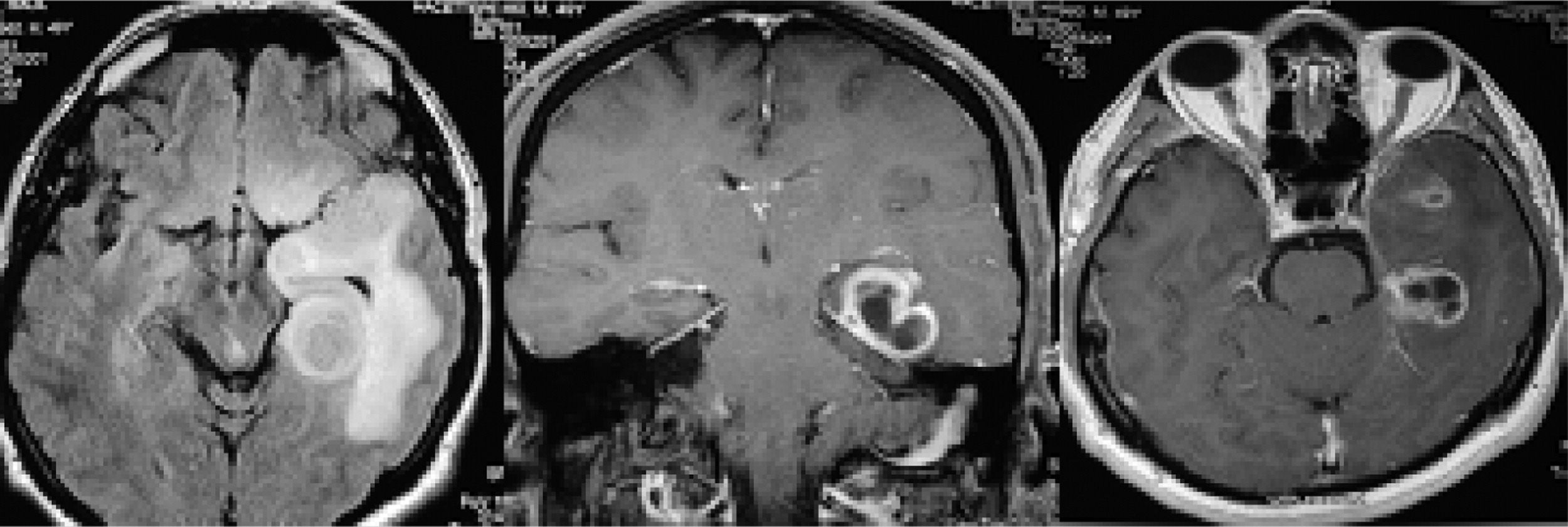
During the previous 7 years, a 50-year-old man had been treated in various psychiatric departments for recurrent depressive and anxiety disorders several times. He continued individual psychotherapy with his psychologist and was tried on several psychotropic agents, with poor response. His symptoms did not improve. He was prescribed paroxetine 30 mg/day and mirtazapine 30 mg /day after his last visit. When he complained of persistent headache, he was referred to a neurologist, and his neurological examination did not show any abnormal signs; MRIs were then performed. A contrast-enhanced MRI of the brain revealed a glial tumor in the left temporal lobe involving limbic structures and the anterior part of the corpus callosum (
Figure 1). The patient underwent osteoplastic craniotomy, with partial resection of the mass. Histopathology confirmed an anaplastic astrocytoma Grade III. He underwent chemotherapy and radiotherapy, and his condition improved.
Discussion
Brain tumors can be associated with a variety of psychiatric symptoms, such as anxiety disorders, panic attacks, personality changes, mania, psychosis, apathy/abulia and cognitive deterioration, without any physical or neurological signs.
1,2This case illustrates the need for prompt assessment for brain imaging when patients present with any atypical psychiatric symptoms or changes in the mental state. Our patient was treated in psychiatric services for 7 years before the brain tumor was diagnosed. It is unclear in our case whether his psychiatric symptoms were of functional origin or were caused by the brain tumor. It is possible that an MRI/computerized tomography scan with contrast may have detected the mass.
3 A thorough neurological evaluation is important to assist in the diagnosis. Atypicality of presentation, poor response to treatment, or waxing and waning of symptoms should lead to suspicion of organic etiology.
When brain tumors develop in patients with established psychiatric disorders, detailed history, neurological examination, and brain imaging become essential, as psychiatric patients are known to have difficulties in reporting and describing their own symptoms.
4 It is recommended that any patient over 40 years of age with a change in neurobehavioral status should have neuroimaging of the brain.
4 The same applies to patients with psychiatric presentations accompanied by specific neurologic or neurobehavioral changes or with poor response to psychopharmacologic treatment. We recommend that any change in the clinical presentation of patients with well-established psychiatric histories or the emergence of atypical psychiatric symptoms should be further explored through neuroimaging.