Parity for mental health benefits returned to the Congressional spotlight last month. The Senate Health, Education, Labor, and Pensions (HELP) Committee heard testimony in support of a parity bill from APA, several legislators, a national managed care company, an administrator of the Federal Employees Health Benefits Program (FEHBP), and a patient with mental illness.
APA is one of 121 organizations eager to see the bill, known as the Mental Health Equitable Treatment Act (S 543), passed this year. The legislation, introduced in March by Senators Pete Domenici (R-N.M.) and Paul Wellstone (D-Minn.) (Psychiatric News, April 6), is a significant improvement on the 1996 parity law, which mandated parity for mental and physical disorders in the lifetime and annual dollar limits insurers can impose on treatment costs. The new bill is also modeled on the parity requirements for the FEHBP, which went into effect in January.
The bill would prohibit health plans from limiting the scope and duration of mental health treatment more than they do medical treatment and imposing discriminatory copays, deductibles, and co-insurance caps on mental health benefits.
The Mental Health Equitable Treatment Act, like the 1996 law, does not dictate that health plans offer mental health benefits but expands the definition of benefits in the 1996 law to include all categories of mental health conditions listed in the most recent edition of DSM.
Another provision states that the bill does not preempt stronger state parity laws. However, it does cover all self-insured plans that were previously exempted by ERISA —which cover at least half of all privately insured beneficiaries. The bill also exempts employers with 25 or fewer employees, compared with 50 in the 1996 law.
The business and health insurance industries have long opposed full parity on the grounds that it would put health insurance out of reach for some Americans due to increased treatment and premium costs.
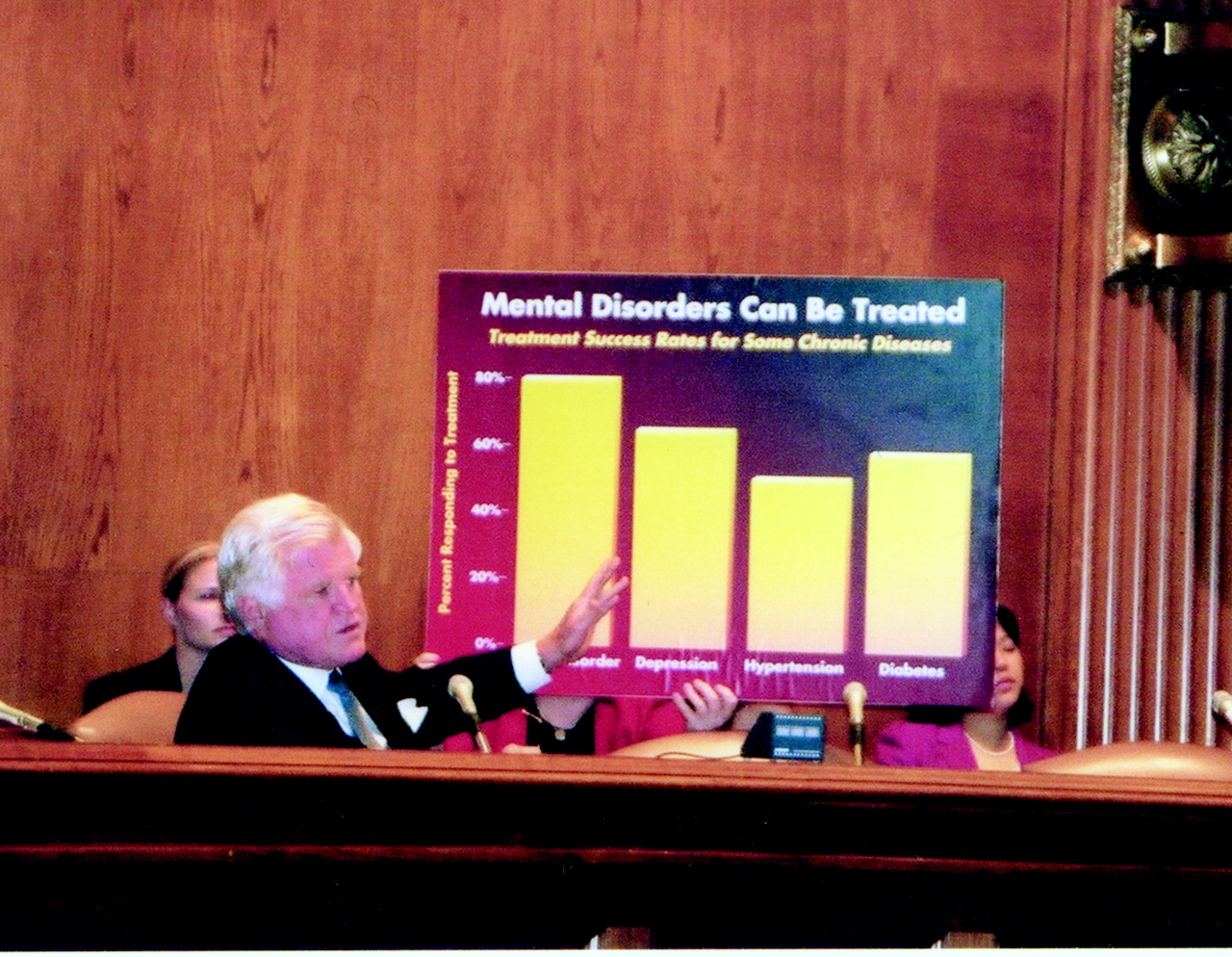
That fear is not based on fact, according to Darrel Regier, M.D., M.P.H., executive director of the American Psychiatric Institute for Research and Education (APIRE). He testified last month before the Senate HELP committee, chaired by Sen. Edward Kennedy (D-Mass.), a cosponsor of the bill. Regier told senators that mental disorders are real, treatable, and cause high levels of disability. Parity insurance coverage for mental disorders, he said, is affordable, addresses a specific market failure, and can support cost-effective treatment to reduce disability.
Included in the data he presented showing parity insurance coverage for mental disorders is affordable was his citation of Texas’s and North Carolina’s experience. In those states parity insurance coverage for state employees, which was introduced along with managed care, dropped costs 30 percent to 50 percent, while the percentage of the population accessing some care increased 1 percent to 2 percent.
Regier noted that while mental health care costs were controlled in this model, universal parity is imperative to ensure that people have access to the care they need. He warned, “There is now evidence that managed behavioral health care in the absence of parity benefits may result in overly restrictive control and even denial of needed mental health benefits. . . . The new potential for abuse or ‘moral hazard’ is no longer the use of unneeded care, but the inappropriate denial of needed care, as not being ‘medically necessary’ treatment.”
Regier pointed out that “the most important reason for improved mental health insurance coverage is that mental disorders exact a terrible toll on our society that can be greatly reduced by scientifically validated treatments.”
He cited the Nobel Prize to psychiatrist Eric Kandel, M.D., which he won for his work on the “molecular basis for understanding the basic cognitive function of memory,” and said “it telegraphed to the world that the scientific basis for understanding mental disorders is accelerating at equal or faster rates than for other medical and surgical disorders.”
“Setting aside the economic and scientific issues for a moment,” Regier told the senators, “I would like to comment as a psychiatric physician who continues to treat patients. For my patients, mental health parity legislation is seen much like civil rights legislation as an essential first step in recognizing the value of a previously oppressed and often stigmatized minority—namely, our patients, our family members, and our fellow citizens with mental disorders. However, even if such legislation is passed, the right to equal treatment in the health care system, as in the larger society, will only be achieved by careful attention to the implementation of parity and other such rights through an ongoing evaluation of our progress.”
Federal Parity Experience
The FEHBP was required by a 1999 executive order to implement parity by this year in the approximately 250 health plans with which it contracts. APIRE is conducting a three-year evaluation of the FEHBP experience.
“The Office of Personnel Management (OPM) has provided an excellent roadmap for implementation of parity benefits in the FEHBP—building on past experience and including an evaluation to make necessary adjustments for assuring access and quality of care,” said Regier.
William E. Flynn, associate director for retirement and insurance at OPM, told senators that his preliminary data on parity this year show that the aggregate total increase in premiums was only 1.3 percent.
Flynn also testified that OPM dropped an initial requirement that health plans could limit parity for mental health benefits for patients who didn’t comply with their treatment plans. When patient advocacy groups expressed concern that the provision would be used to cut off needed treatment, OPM dropped the requirement.
Next Steps
Although the bill had 49 bipartisan cosponsors at press time, a full vote by the Senate HELP committee may be delayed until after this month’s recess. Ranking minority member Sen. Judd Gregg (R-N.H.) objected to the hearing’s short notice last month and excused himself from the hearing. Kennedy offered to schedule a second hearing before the committee begins its deliberations.
Sen. Bill Frist (R-Tenn.) supports parity but indicated he would like some changes made to the current bill. These issues will undoubtedly be discussed when the committee takes up the bill. Frist prefers limiting the definition of parity to “biologically based illnesses with strong scientific evidence” rather than including all DSM illnesses.
Because there is a shortage of health and mental health care professionals in rural areas, patients may have to go out of network, thus potentially increasing insurance premiums, explained Frist.
He also recommended that the committee consider the impact of the proposed parity legislation on employers whose “ability to manage health care is more limited under the sweeping new patient protection rights legislation” passed by the Senate last month (Psychiatric News, July 20).
Regier’s testimony is posted on APA’s Web site at www.psych.org/pub_pol_adv/drregiertestimony71301.cfm. ▪