State officials are attempting to rein in the escalating costs of prescription drugs as they struggle to balance Medicaid budgets.
The most publicized effort occurred in Michigan, where the legislature established a formulary that requires authorization from a “state technician” if a drug is not on the list. The effort was budgeted to generate $42 million in savings (Psychiatric News, January 18).
The first successful state attempt to institute a formulary took place in May 2001, when the Florida legislature established a “preferred drug list” (PDL) that consisted of drugs for which manufacturers would grant supplemental rebates of 10 percent. Drugs used to treat mental illness and HIV are exempt from the legislation (Psychiatric News, March 1).
The formulary and PDL are not the only strategies being used to contain costs. In its advocacy guide, “Access to Medications,” the National Mental Health Association (NMHA) warned that Medicaid officials are focusing on new or enhanced prior-authorization requirements, putting limits on the number and amount of prescriptions per month, and imposing tiered copayments.
Oregon, according to the NMHA, is creating a “reference-based formulary” in which the most effective drug in a class will serve as the reference drug, and its price will be the maximum reimbursement for similar drugs. Georgia implemented tiered copayments ranging from 50 cents to $3, and Louisiana is instituting a formulary based on the Florida law, but without an exemption for drugs used to treat mental illness.
The National Conference of State Legislatures found that as of October 2001, 26 states had passed laws to regulate medications under Medicaid.
Impact of Cost-Containment Measures
What impact have these cost-containment measures had? The short answer is that no one knows.
Leighton Ku, senior fellow in health policy at the Center on Budget and Policy Priorities, said, “[M]ost states are completely clueless with respect to how well these programs are working except from the perspective of. . .saving money or not.” He added that states were not looking very hard to determine if there were negative effects for beneficiaries.
Jeff Farkas, a principal at Health Strategies Consultancy, told attendees at the National Managed Care Congress in April that a drawback of the Florida formulary program is the lack of a plan for evaluation of its impact on patients.
“While all state Medicaid programs provide outpatient prescription drug coverage, slightly more than 1 in 4 Medicaid patients aged 18 to 64 could not afford to fill at least one prescription in the last year,” concluded a study issued in April titled “Affording Prescription Drugs: Not Just a Problem for the Elderly.”
The study was directed by Peter J. Cunningham under the auspices of the Center for Studying Health System Change, a nonprofit policy research organization funded by the Robert Wood Johnson Foundation.
He found that cost barriers were highest for those most likely to need prescription drugs, namely, persons with chronic illness. More than 40 percent of Medicaid recipients with two or more chronic conditions reported not obtaining medications because of cost.
Beneficiaries in states that have implemented four or five cost-control measures were twice as likely to report cost barriers as those living in states with either one or no cost-control policies.
Reports From Psychiatrists
An informal request for information from members of the American Association of Community Psychiatrists (AACP), however, did not reveal significant problems in terms of access to medication for persons with mental illness.
AACP President Jacqueline M. Feldman, M.D., posted a request on the members’ list serve for information about their experiences securing prescription drugs for Medicaid beneficiaries. E-mail requests for information were sent to AACP board members.
Barbara Rohland, M.D., chair of the psychiatry department at Texas Tech University, wrote, “I have not experienced this problem in Texas. I work 10 hours per week at the state agency service for persons with Medicaid. . . and have been impressed by the good access that patients have to medications, including atypical antipsychotics.”
Benjamin Crocker, M.D., medical director of the Maine Department of Mental Health, Area II, wrote, “I have had to put in some paperwork for some meds, but I always got what I felt was needed.”
Jack Haggerty, M.D., director of the Division of Social and Community Psychiatry at the University of North Carolina, commented, “Right now obtaining prior approval for Medicaid patients is less hassle than it is with managed care plans. Most psychotropics are excluded from the preauthorization process, but we anticipate that North Carolina will be moving to a formulary that will require sequencing of meds of all types.”
However, Charles Huffine, M.D., assistant medical director for child and adolescent programs of the King County (Washington) Mental Health, Chemical Abuse, and Dependency Services Division, wrote, “Due to a budget catastrophe this year, we have seen the initiation of a ‘sort of’ voluntary constriction on formulary in Washington state and a dampening of our freedom to prescribe.”
Trouble Ahead?
Both NMHA and the National Alliance for the Mentally Ill (NAMI) warn about the future impact of state budget cuts to Medicaid.
NAMI spokesperson Bob Carolla told Psychiatric News, “I suspect that the reason your members have not reported significant problems in access to medication is that the full effect of the policies has not been felt.”
Mike Fitzpatrick, NAMI’s director of state policy, concurred, saying many state legislatures are considering bills to restrict access to medications.
Dave Nelson, NMHA’s vice president for health care reform, said, “I strongly disagree with the idea that the impact of restrictions has not been felt. In Mississippi, for example, a mental health consumer died as a result of a physical illness and a limit on the number of Medicaid prescriptions that could be filled in a one-month period.”
NMHA has produced a two-volume advocacy resource manual to help members fight restrictive legislation and is conducting training sessions for advocates throughout the country.
Analysis of data on Medicaid expenditures on drugs used to treat mental illness suggests that those advocacy efforts will be needed.
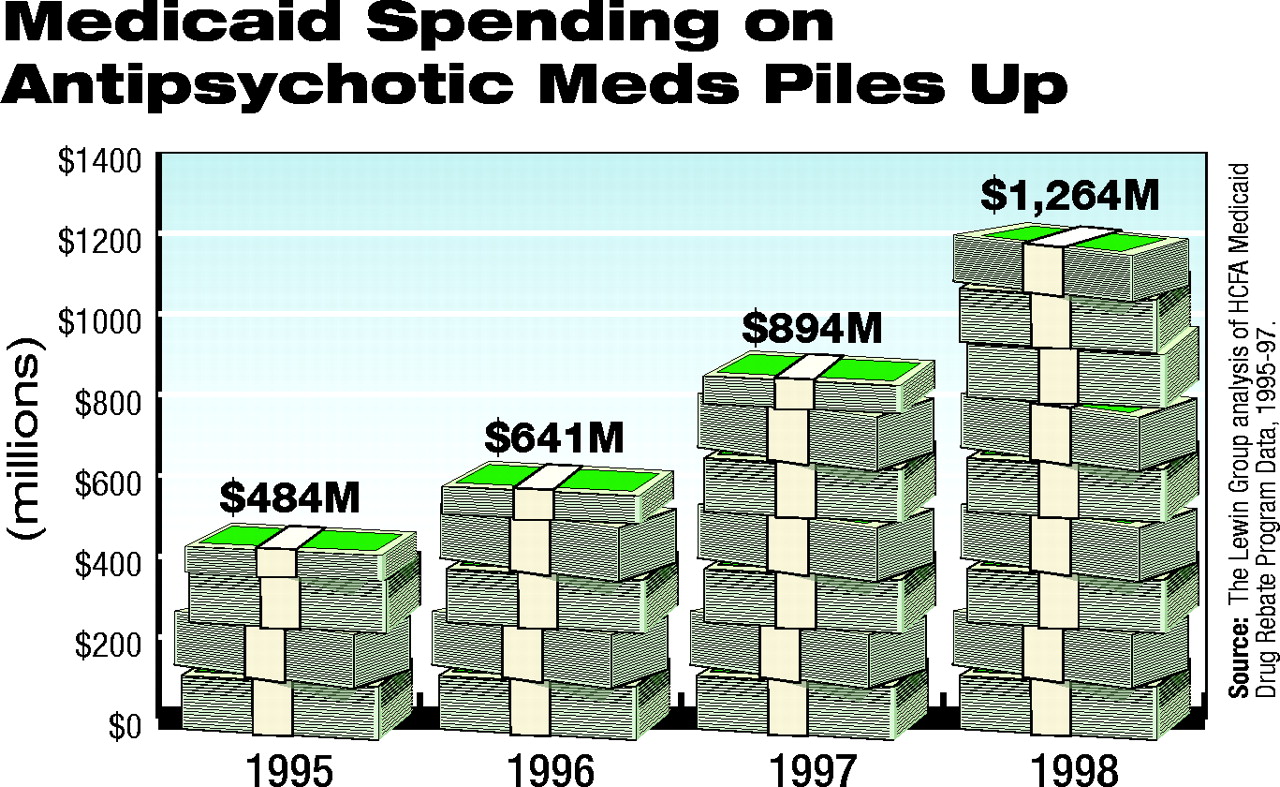
The National Institute of Mental Health funded the Lewin Group to study issues concerning access to and utilization of new antidepressant and antipsychotic medications. Its report, issued in January 2000, found no evidence that formularies were restricting access to newer psychotherapeutic agents.
The researchers did find, however, that newer medications are often considerably more expensive than the medications they are intended to replace. For example, the average wholesale price for the antidepressant fluoxetine is $150.10 for a 30-day supply of an average therapeutic dose, while a 30-day supply of the older antidepressant, amitriptyline, lists for $3 for a generic version.
From less than $500 million in 1995 to more than $1.2 billion just four years later, the rising cost of antipsychotic medications for the cash-strapped Medicaid program may lead to compromises in care.And, according to the report, the use of atypical antipsychotics in Medicaid has grown dramatically since 1995. Spending on those drugs jumped 160 percent. The introduction of atypical antipsychotics did not merely replace older therapies, but instead expanded the market for use of those agents (see chart).
State Medicaid budgets have come under increasing pressure since the Lewin Group collected its data. According to NMHA, in 2001 over half of the states reported cost overruns in their Medicaid programs and projected double-digit growth rates for 2002 expenditures.
A survey by the Kaiser Commission on Medicaid and the Uninsured in October 2001 found that in most of the 20 states they surveyed, the governor had directed Medicaid officials to prepare proposals to reduce the current-year spending below the level authorized by the legislature (Psychiatric News, December 7, 2001).
The Urban Institute estimated that Medicaid spending for outpatient prescription drugs increased by an average of 18.1 percent per year from 1997 to 2000, compared with 7.7 percent for all Medicaid expenditures.
Incoming APA President Paul Appelbaum, M.D., told Psychiatric News, “Policies that restrict access to psychiatric medications hurt patients in ways that are both obvious and more insidious. When patients can’t get the medications they need, because the copays are unaffordable or because the medications are not covered at all, the harm is blatant.
“But patients are also negatively impacted when their psychiatrists are diverted from patient care to completing forms or making phone calls to get an exception to rigid formulary policies. This is not the right answer to shortfalls in state budgets.”
(Psychiatric News would like to hear from psychiatrists about their experience with the effects of cost-containment measures on the availability of prescription drugs for Medicaid patients. Please send your comments to Kate Mulligan by e-mail at [email protected].)
The Web site for NMHA is www.nmha.org. The Web site for NAMI is www.nami.org. The report by the Lewin Group is posted on the Web at www.aspe.hhs.gov/health/reports/psychmedaccess/. ▪
Escalating costs of antidepressant and antipsychotic medications are taxing the resources of already constricted Medicaid budgets. Will patients pay the price?
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
To download the citation to this article, select your reference manager software.
There are no citations for this item
View Options
View options
Get Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.