Back in the 1990s, Patricia Hamilton, a financial analyst with IBM, decided to give up her job because she had spinocerebellar ataxia, an autosomal dominant disorder of the cerebellum that she had inherited from her father and her grandfather.
“Increasing difficulty with balance in walking, problems with slurred speech, and trouble focusing made it clear to me that I had to stop working there,” Hamilton wrote on her Internet homepage.
Usually patients like Hamilton are not on the radar screen of psychiatrists. But maybe they should be, a new study conducted by Johns Hopkins University scientists and published in the August American Journal of Psychiatry suggests. The study has found that a number of persons with diseases like Hamilton’s also have psychiatric disorders.
True, the cerebellum has long been known to be concerned with muscle tone, balance, conversion of muscle contractions into smooth, coordinated movements, and other physical movement matters. And diseases of the cerebellum have long been known to lead to deterioration in physical movements. But during the past decade or so, evidence has started cropping up that the cerebellum may influence cognition and emotions as well. What’s more, some case reports have suggested that degenerative cerebellar diseases can trigger psychological disturbances.
Russell Margolis, M.D., an associate professor of psychiatry at Johns Hopkins University School of Medicine, and both psychiatric and neurological colleagues at that institution, decided to conduct a study to determine whether the latter is truly the case, and if so, what types of psychological disturbances such patients might have.
Margolis and his colleagues recruited 81 persons to participate in their study. Thirty-one had degenerative cerebellar diseases—spinocerebellar ataxia or multisystem atrophy—for five years or more. Twenty-one had Huntington’s disease, a disease that impairs physical movement, but that arises from damage to the basal ganglia of the brain, not to the cerebellum. These subjects had had Huntington’s for about the same length of time that the cerebellar subjects had had their diseases and thus served as a disease-comparison group. Twenty-nine individuals who were neurologically normal served as a control group. Subjects in all three groups were similar in age, sex, race, and educational level.
Each subject underwent a comprehensive psychiatric assessment by a neuropsychiatrist experienced in the assessment and treatment of patients with movement disorders. An “informant” for each subject supplied more information. Informants were specifically asked about distinct, enduring changes in personality since the onset of the movement disorder or, for the healthy control group, over recent years. To avoid the assumption of a causal relationship between personality change and cognitive impairment, the diagnosis of the former was made independently from that of the latter. The data on each subject were then reviewed by a second neuropsychiatrist who was unaware of the neurological diagnosis, and a consensus psychiatric diagnosis (or diagnoses) for the subjects was established. The investigators then compared findings among the groups.
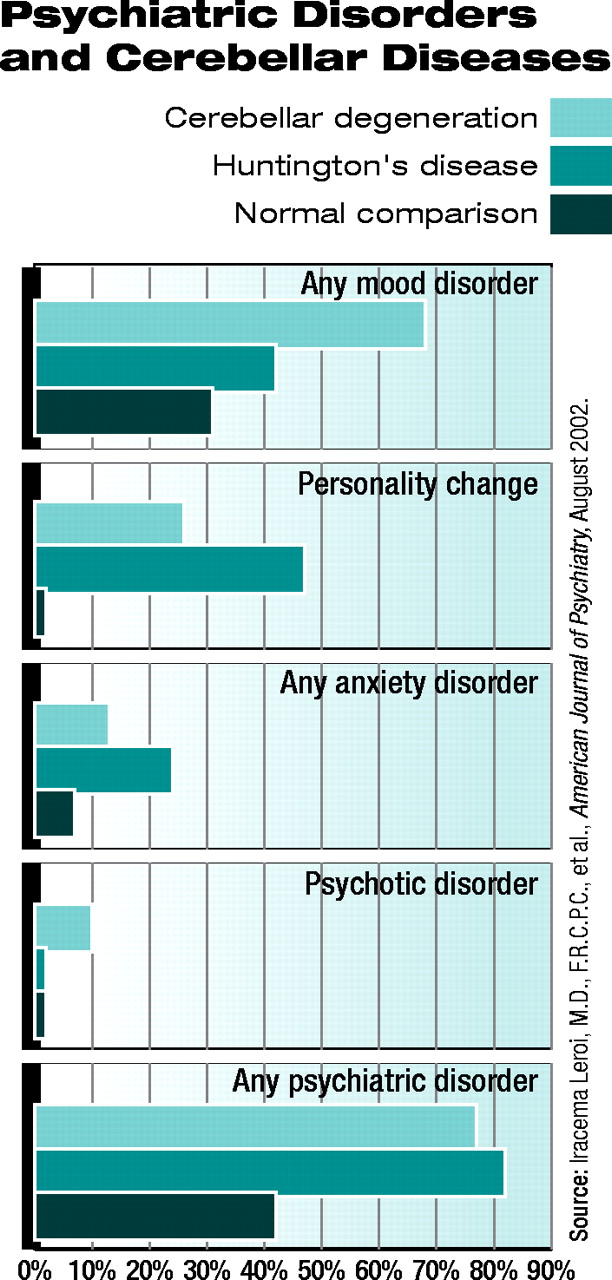
Researchers were surprised to find that the prevalence of noncognitive psychiatric disorders in the cerebellar-degeneration group was nearly the same as in the Huntington’s-disease group.First, there was a highly statistically significant difference in the prevalence of noncognitive psychiatric disorders between the degenerative cerebellar disease group and the healthy control group, which did not surprise the researchers. Specifically, the overall rate of noncognitive psychiatric disorders in the cerebellar group was 77 percent (24 of 31 subjects) versus 41 percent (12 of 29 subjects) in the control group. Sixty-eight percent of the cerebellar group (21 of 31 subjects) had mood disorders, whereas only 32 percent of the healthy control group did (nine of 29). Twenty-six percent of the cerebellar group had experienced a personality change, whereas none in the healthy control group had.
Second, the prevalence of noncognitive psychiatric disorders in the cerebellar group—77 percent—was nearly the same as that in the Huntington’s group, which was 81 percent. This finding surprised the researchers. They did not expect the cerebellar group to have nearly as many psychiatric problems as the Huntington’s group, since Huntington’s is such a devastating neurological disease.
Granted, the Huntington’s group had a much higher prevalence of cognitive impairment than the cerebellar group did—71 percent versus 19 percent—but the 19 percent is still noteworthy, the investigators believe.
Thus, the high rates of psychiatric disorders and the fairly high rate of cognitive impairment found in the degenerative cerebellar disease subjects suggest that many, if not most, persons with such diseases would profit from psychiatric help, Margolis and his team concluded in their study report.
“Although the underlying neurodegeneration in degenerative cerebellar diseases may not yet be treatable,” they explained, “management of the accompanying psychiatric disorders and cognitive impairment with a combination of education, pharmacotherapy, and supportive psychotherapy may have a major impact on quality of life for patients and their families.”
Unfortunately, most persons who could use such help are probably not getting it because of American psychiatry and American neurology having been split into discrete medical specialties, Stuart Yudofsky, M.D., and Robert Hales, M.D., observed in an accompanying editorial. Yudofsky is chair of psychiatry at Baylor University and editor of the Journal of Neuropsychiatry and Clinical Neurosciences. Hales is chair of psychiatry at the University of California, Davis, associate editor of the journal, and editor-in-chief of American Psychiatric Publishing Inc.’s book division.
The study was funded by the National Alliance for Research on Schizophrenia and Affective Disorders and by the National Institutes of Health.
Patients with cerebellar diseases may experience not just deterioration in physical movements, but also psychiatric disorders. Thus, patients with cerebellar diseases may need psychiatric as well as neurological help.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.