Physicians are scheduled to receive a 4.4 percent cut in Medicare reimbursement on January 1, 2003, with similar cuts projected for the next two years.
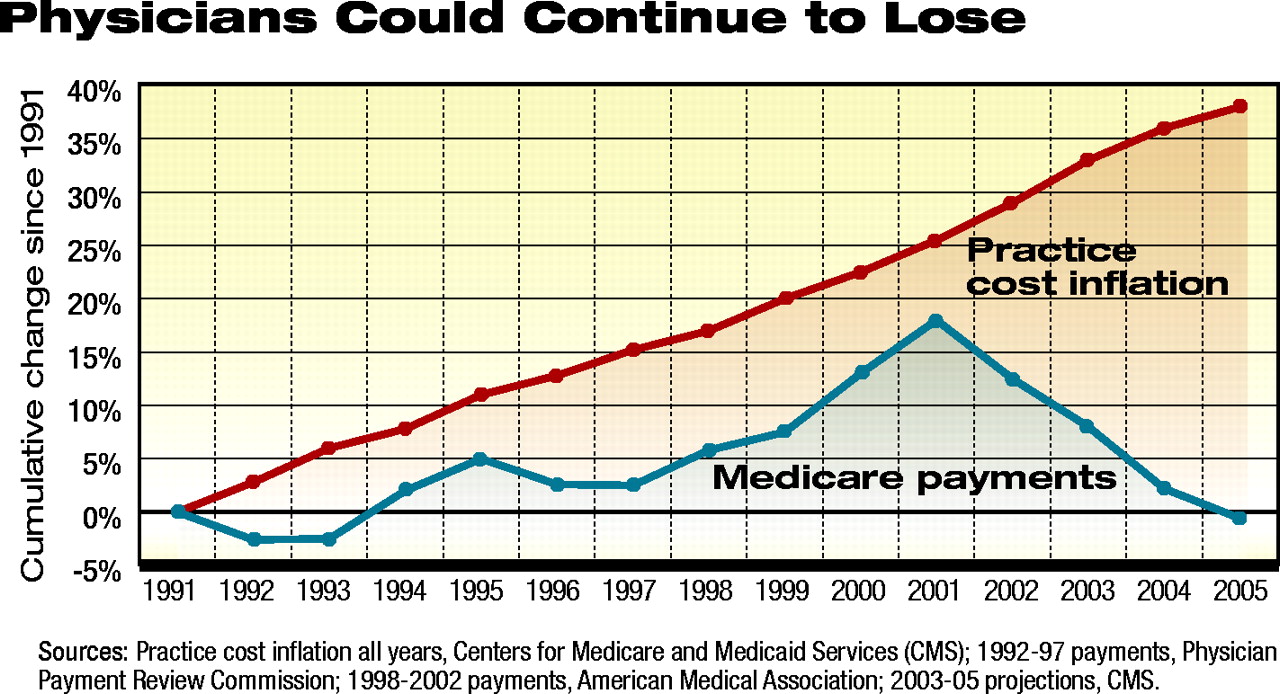
The costs of providing medical care to Medicare beneficiaries in 2005 is projected to be 40 percent higher than 1991 costs. Medicare payments are projected to be somewhat less in 2005 than they were in 1991.From 1991 through 2005, projections are that inflation in practice costs will have risen nearly 40 percent. In 2005 Medicare physician payment rates will be below their 1991 levels, unless Congress and the president act to reverse the scheduled cuts (see graph).
What impact have the 2002 cut and the likelihood of future cuts had on Medicare patients who need psychiatric services?
Psychiatric News sent several questions about access via e-mail to members of APA’s Medicare Advisory Corresponding Committee, which has a representative in each state.
General Psychiatrists May Drop Out
Allan Anderson, M.D., chair of the Geriatric Psychiatry Committee for the Maryland Psychiatric Society, said, “I predict that if further cuts occur, many general psychiatrists who see some geriatric patients will stop doing so. Many psychiatrists will stop consulting in nursing homes and assisted-living facilities. Even prior to the 2002 cut, psychiatrists were penalized for caring for patients in long-term-care facilities because of a lower reimbursement rate.”
Gary Moak, M.D., a solo practitioner in Westborough, Mass., specializing in geriatric psychiatry, agreed with Anderson’s prediction about general psychiatrists. “Remember,” he told Psychiatric News, “only a very small percentage of psychiatrists have practices with large numbers of geriatric patients. They are dedicated to that population. The cuts will have the greatest impact on the willingness of general psychiatrists to treat Medicare patients. Even now, the geriatric population is greatly underserved.”
Several psychiatrists commented, however, that Medicare reimbursement is better than that from other payers. David M. Tobolowsky, M.D., a solo practitioner, wrote, “In my city of Miami, Medicare fees are higher than Blue Shield and many PPO fees. I stopped seeing new Medicaid patients because Medicaid pays around 55 percent of Medicare fees.”
Big Picture Said to Be Worse
Alan Seigel, M.D., is one of three psychiatrists in a multidisciplinary group practice that is the largest provider of geriatric mental health services in southern Connecticut. The practice evaluates 1,000 new patients a year, provides ongoing treatment, and is the largest provider of treatment for Alzheimer’s disease in the state.
He told Psychiatric News, “We’re maxed out and constantly have patients referred to us that we can’t accept. Access has deteriorated greatly during the last five years. It’s frustrating because we have better interventions now that would enable people to stay in their homes.”
Instead, said Seigel, many patients who would have profited from early interventions end up in emergency rooms and hospitals. They are hospitalized for dementia, suicidal depression, and failure to thrive.
Nearly one-fifth of Connecticut’s population is over 65. The aging of the baby boomers will further exacerbate the problem. (See box for story about impact of cuts on a geriatric clinic in Washington state.)
Several psychiatrists noted that state fiscal constraints were adding to the problem of Medicare cuts. John J. Wernert, M.D., told Psychiatric News, “In Indiana, the Medicaid program has been picking up the 50 percent copay for those patients who are eligible. But because of the fiscal pressures on Medicaid, state officials have announced the end of that practice. So, psychiatrists will be taking another cut from Medicare at the same time they lose Medicaid reimbursement for those patients who cannot afford the 50 percent copay.”
Wernert and three other geriatric psychiatrists in a group practice manage psychiatric care in 42 nursing homes and three inpatient hospital units.
He added, “Geriatric patients are sicker, cognitively challenged, on a plethora of medications, and usually living on a tight budget. When a doctor receives only 32 percent of his charge for a difficult appointment and has Medicare billing and administrative hassles to deal with, it is no wonder that many seriously consider dropping or restricting their Medicare caseload.”
Anderson told Psychiatric News, “The mental health system in Maryland already is in a state of crisis. Clinics across the state are closing. Medicaid does not pick up the full copay for patients with both Medicare and Medicaid coverage.”
Increased Cost Shifting
At an invitational meeting about cost-shifting, Paul B. Ginsburg, Ph.D., president of the Center for Studying Health System Change, a nonprofit organization that conducts research about health care and provides analysis, told the audience, “The Medicare payment reduction is one of four factors resulting in increased policy interest in cost shifting” (see page 15).
In fact, two psychiatrists reported that their institutions were absorbing some costs associated with treating Medicare patients.
Eric Larson, M.D., chair of the mental health department at Park Nicollet Health Services in Minneapolis, told Psychiatric News, “Clearly, Medicare is the lowest payer for Park Nicollet, an integrated multispecialty care system. Accepting Medicare patients costs our organization money, but we feel providing treatment to them is part of our mission as a nonprofit health care system.”
Michael J. Vergare, M.D., chair of the department of psychiatry at Thomas Jefferson University-Jefferson Medical College in Philadelphia, told Psychiatric News that the Jefferson Health System and its hospitals were underwriting a portion of the costs of caring for Medicare patients.
He added, “The problem has been exacerbated by the extraordinary cost of malpractice insurance, which now ranges from $18,000 to $23,000 in the Philadelphia area.”
The Jefferson Health System includes the Albert Einstein Healthcare Network, Thomas Jefferson University Hospital, and other health care providers in the Philadelphia area.
Donald W. Fisher, Ph.D., president and chief executive officer at the American Medical Group Association, said at the meeting that the Mayo Clinic in Minnesota anticipated a loss of $34.2 million total for 2002 and 2003 that could be attributed to the physician reimbursement cuts, assuming the 4.4 percent cut is not reversed.
What’s Next?
Fisher told attendees, “I think the ultimate shift here is going to be not only from the government to the commercial players, but it’s already begun to the individuals themselves through more out-of-pocket costs [higher premiums] and higher copays and deductibles.”
Chester Schmidt Jr., M.D., chair of APA’s Committee on RBRVS, Codes, and Reimbursements, noted a similar pattern in mental health services.
He believes that the Medicare payment cuts are exacerbating a trend toward a multitiered mental health system in which access to psychiatrists may be determined by the ability to pay.
“Persons on Medicaid and the uninsured or underinsured frequently receive care through university-based community psychiatry programs from nonphysician mental health professionals who are supervised by a psychiatrist. With cuts in reimbursement and decreased access to psychiatrists, an influx of Medicare patients to these programs is likely.”
Schmidt is a professor of psychiatry at Johns Hopkins School of Medicine.
In the private sector, administrative restrictions and low payments associated with managed care caused many psychiatrists to refuse to participate in managed care panels, he said. Now, those psychiatrists set their own fees and expect patients to pay the full amount and collect what they can from insurance.
On November 14 the House of Representatives passed legislation, HR 5063, that would have allowed the administration to revise the Medicare physician payment formula, correcting errors that date back to 1998 and 1999.
Under the most favorable interpretation, the legislation would have permitted a positive update of 1.5 percent in 2003 and positive updates in 2004 and 2005. The Senate adjourned without acting on its version of the legislation.
Jay Cutler, J.D., APA’s director of the Division of Government Relations, told Psychiatric News, “Psychiatric physicians have every right to challenge the Senate and demand an explanation for its failure to act to correct a mistake that is threatening access to psychiatric and other medical care for America’s seniors.”
There will be a window of opportunity in which Congress could act to rescind the cuts. The Centers for Medicare and Medicaid Services intended to publish the Medicare physician payment rule in early December, after which there is a 60-day congressional review period before the 2003 cuts take place.
Cutler urged members to contact their elected officials through the AMA Grassroots Hotline at (800) 833-6354 or e-mail them through the AMA at the Web site <www.ama-assn.org/go/grassroots>. “The message is ‘Fix it,’” he said. “Give examples of how the cuts will affect access to care and your own ability to maintain a practice.”
APA has worked closely with the AMA on the physician reimbursement cuts during the last year. Cutler and his staff have also issued a series of action alerts to members and press releases describing the effect of the cuts on access to psychiatric services.
Action alerts on Medicare are posted on APA’s Web site at www.psych.org/pub_pol_adv/Action_alerts.cfm. The list of state representatives of the Medicare Advisory Corresponding Committee is posted at www.psych.org/pract_of_psych/index.cfm. Members with concerns can contact state representatives or APA staff member Ellen Jaffe at [email protected]. Psychiatric News would also like to know about problems resulting from payment cuts; information may be e-mailed to [email protected]. ▪
Psychiatrists report an erosion in access to care because of cuts in Medicare reimbursement. APA urges Congress to seize its opportunity to act before the situation becomes worse in early 2003.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.