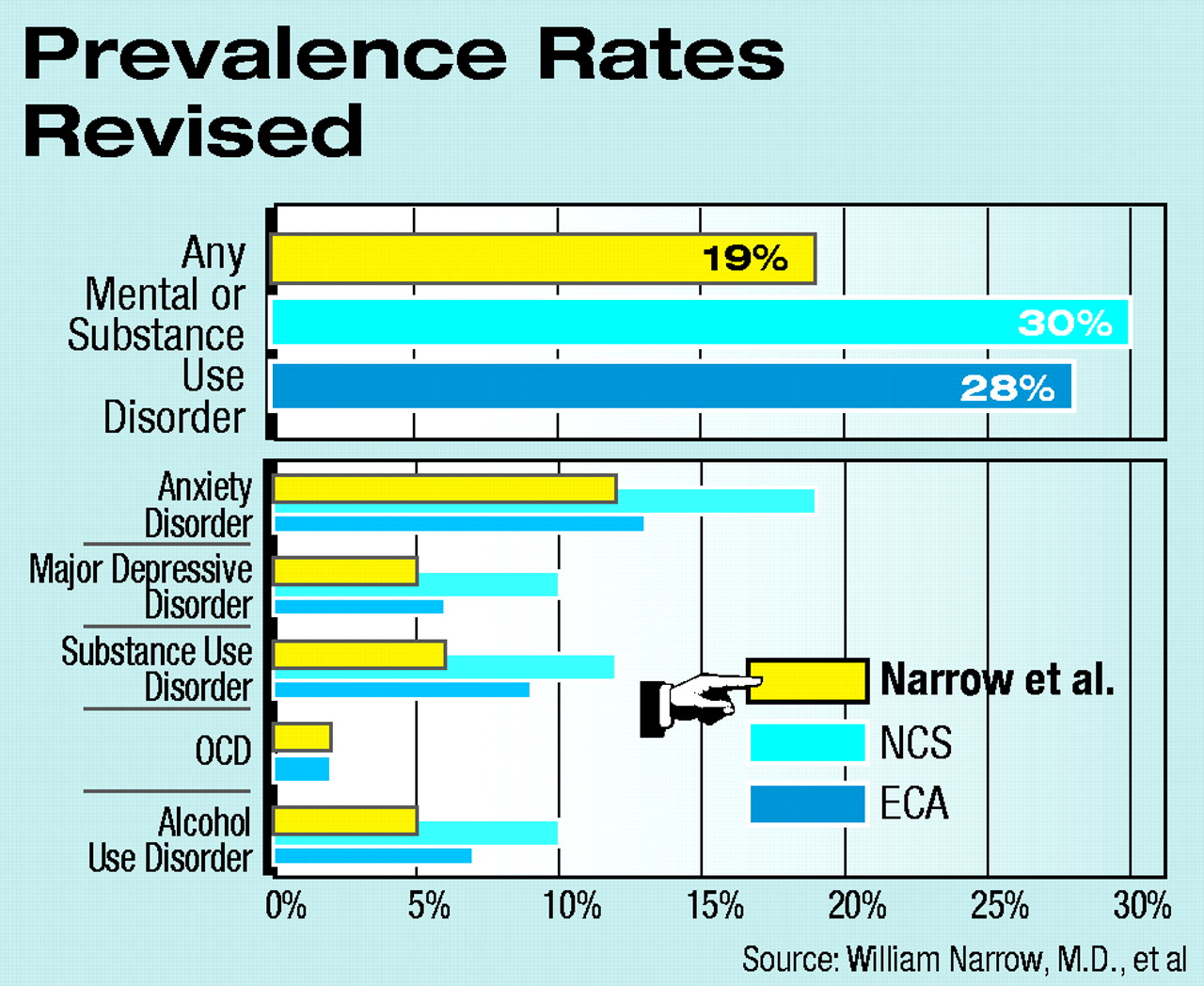
What is the one-year prevalence rate for any mental or substance use disorder in the United States? Two large community surveys have provided answers in recent years, and the answers have been 28 percent to 30 percent.
Now a lower figure—19 percent—is reported in the February Archives of General Psychiatry by a team of psychiatric epidemiologists. This new figure represents about 19 million Americans fewer than the 28 percent rate. The new figure also more accurately reflects the true picture than the old rates, according to the epidemiologists.
The epidemiologists are William Narrow, M.D., Darrel Regier, M.D., and Donald Rae of the American Psychiatric Institute for Research and Education (APIRE), along with Lee Robins, Ph.D., of Washington University School of Medicine.
The National Comorbidity Survey (NCS) and the National Institute of Mental Health Epidemiologic Catchment Area Program (ECA) are the two large community surveys that yielded the one-year prevalence rates for any mental or substance use disorder of 30 percent and 28 percent, respectively. They are also the surveys that have provided one-year prevalence rates for specific mental or substance use disorders.
However, there are several problems with these surveys: They have produced discordant results, and the prevalence rates that they have yielded are considered by some authorities in the psychiatric epidemiology field to be implausibly high. In fact, as Narrow and his colleagues pointed out in their study report, “If these prevalence rates are taken as a proxy for mental health treatment need, the mental health system would have to expand enormously to meet this need. . . .”
So Narrow and his team decided to reanalyze data from the two surveys, requiring that a “clinical significance” criterion be met before any mental health symptoms could be classified as mental disorders. The rationale? It would be in keeping with the DSM-IV specification that mental health problems must be “clinically significant” before they can be truly considered mental disorders.
The researchers analyzed the answers of survey participants to questions such as whether the symptoms they were experiencing were interfering with their lives, whether they had told a professional about their symptoms, and whether they were using medication for their symptoms. If answers to such questions were yes, then the participant’s symptoms were considered a mental disorder. If the answers were no, then the symptoms were not considered a mental disorder.
For instance, the NCS’s one-year prevalence rate for any anxiety disorder had been 19 percent before Narrow and his colleagues applied a clinical-significance criterion to the data. Afterward, the prevalence rate was 12 percent. The ECA’s one-year prevalence rate for bipolar I disorder had been 0.9 percent before the clinical-significance criterion was applied; afterward it was 0.5 percent.
The investigators then pooled their revised findings for the two surveys to come up with one-year prevalence rates for specific mental disorders and for all disorders combined. If there was a difference between the two surveys regarding a particular disorder, they conservatively selected the lower estimate. If only one survey addressed a particular disorder, then they used the results from that survey. For instance, their revised prevalence rates for generalized anxiety disorder and posttraumatic stress disorder were based on the NCS data. Their revised prevalence rates for obsessive-compulsive disorder, antisocial personality disorder, and anorexia nervosa were based on the ECA data.
By using this methodology, Narrow and his team reported, the discrepancies between the results of the two surveys declined, and the prevalence rates for mental disorders were generally lower than what they had been before.
Researchers have found new one-year prevalence rates for mental and substance use disorders by reanalyzing data from the National Comorbidity Survey and the NIMH Epidemiologic Catchment Area study.The lower rates (see chart on page 2), they believe, more realistically reflect the true incidences of mental disorders in the United States than had the older rates. “These revised rates represented a group of persons with higher levels of disability and suicidal ideation than in previous estimates, which we consider preliminary evidence of the validity of the data,” they pointed out in their report.
The good news about these new figures, Narrow and his fellow epidemiologists wrote, is that they are more likely to represent people in need of mental health services than the old figures showed. The bad news, however, is that “even when disorders are restricted to those with clinical significance, their numbers are still overwhelming for planning purposes.”
Also, they commented, “very little is known about the clinical significance and treatment needs for disorders that are not currently included in epidemiologic surveys, such as most personality disorders, adjustment disorders, and impulse control disorders.”
In an accompanying editorial, Jerome Wakefield, Ph.D., at the Institute for Health, Health Care Policy, and Aging Research, and Robert Spitzer, M.D., a psychiatrist at Columbia University who led the development of DSM-III and DSM-III-R, agreed with Narrow and his team that the two surveys had some serious problems. But they questioned whether adding a clinical-significance criterion to analysis of the surveys’ data really provided more valid mental disorder prevalence rates than those that had been initially reported. In fact, Wakefield and Spitzer wrote, the new analysis by Narrow and his colleagues addresses not disorder rates but a different entity: treatment need. The authors offered no conceptual argument that the addition of their clinical significance criterion “represents a valid redefinition of disorder.”
The research that Narrow and his team undertook to revise the prevalence rates was funded by the American Psychiatric Foundation and by the van Ameringen Foundation.
By applying a “clinically significant” criterion to previous survey results, psychiatric epidemiologists find that the one-year prevalence rate for any mental or substance use disorder is 19 percent rather than about 28 percent.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
To download the citation to this article, select your reference manager software.
There are no citations for this item
View Options
View options
Get Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.