Employers are beginning to take a serious look at how the health of their employees affects the bottom line, according to information presented at the Washington Business Group on Health (WBGH) meeting in March (Psychiatric News, April 19).
Walter Stewart, Ph.D., M.P.H, director of the AdvancePCS Center for Work and Health and an adjunct professor at Johns Hopkins University, spoke on “Getting a Handle on the True Costs of Illness to Improve Productivity” and later expanded on his comments in an interview with Psychiatric News.
AdvancePCS provides pharmacy benefits management (PBM) and other health-related services.
Stewart said that a key element in persuading employers to act on the link between health and productivity is providing them with quantitative data on actual costs and an easy-to-understand metric that translates into a direct dollar value and applies broadly across all occupations and work settings.
“Most employers know there’s a link between health and productivity, but because the link has been difficult to quantify, they have chosen not to act,” he told Psychiatric News.
In part, quantification has been difficult, according to Stewart, because research has focused on productivity (how much an employee produces) as opposed to productive time (number of effective hours worked) and because easy-to-use measurement tools are not available.
Business factors such as the work environment can affect productivity, weakening a causal relationship between the health of an employee and what he or she accomplishes at work.
American Productivity Audit
Stewart and his colleagues began the American Productivity Audit last July with telephone interviews of a random sample of U.S. workers each day. The first full year of the survey will be completed June 30, with a total of 25,000 interviews.
The five- to 15-minute survey interview covers items such as occupation description, health assessment, missed days of work due to health conditions (self and others), reduced performance at work because of health conditions, and demographic factors such as age and sex.
Before beginning the audit, the research team tested six different questionnaires and two time periods of recall. Two weeks was the longest period for which recall was deemed reliable, according to Stewart.
After validation of the interview questions, the research team began conducting 2,000 telephone interviews of workers in randomly selected households each month. The database now includes results of more than 17,000 interviews.
Stewart analyzed the prevalence of 11 common ailments during a two-week period of recall among subjects in the database. For purposes of his analysis, he separated “fatigue” and “sad/blue,” although he recognizes an overlap. Sad/blue is not synonymous with a diagnosis of depression. Stewart plans follow-up studies to determine what percentage of workers reporting feeling sad/blue meet diagnostic criteria for depression and the implications of that diagnosis on an employer’s costs.
Headache and other pain conditions were reported most frequently. Fatigue was second, with 42 percent reporting at least one episode during the preceding two weeks. About 29 percent of the respondents reported feeling sad/blue.
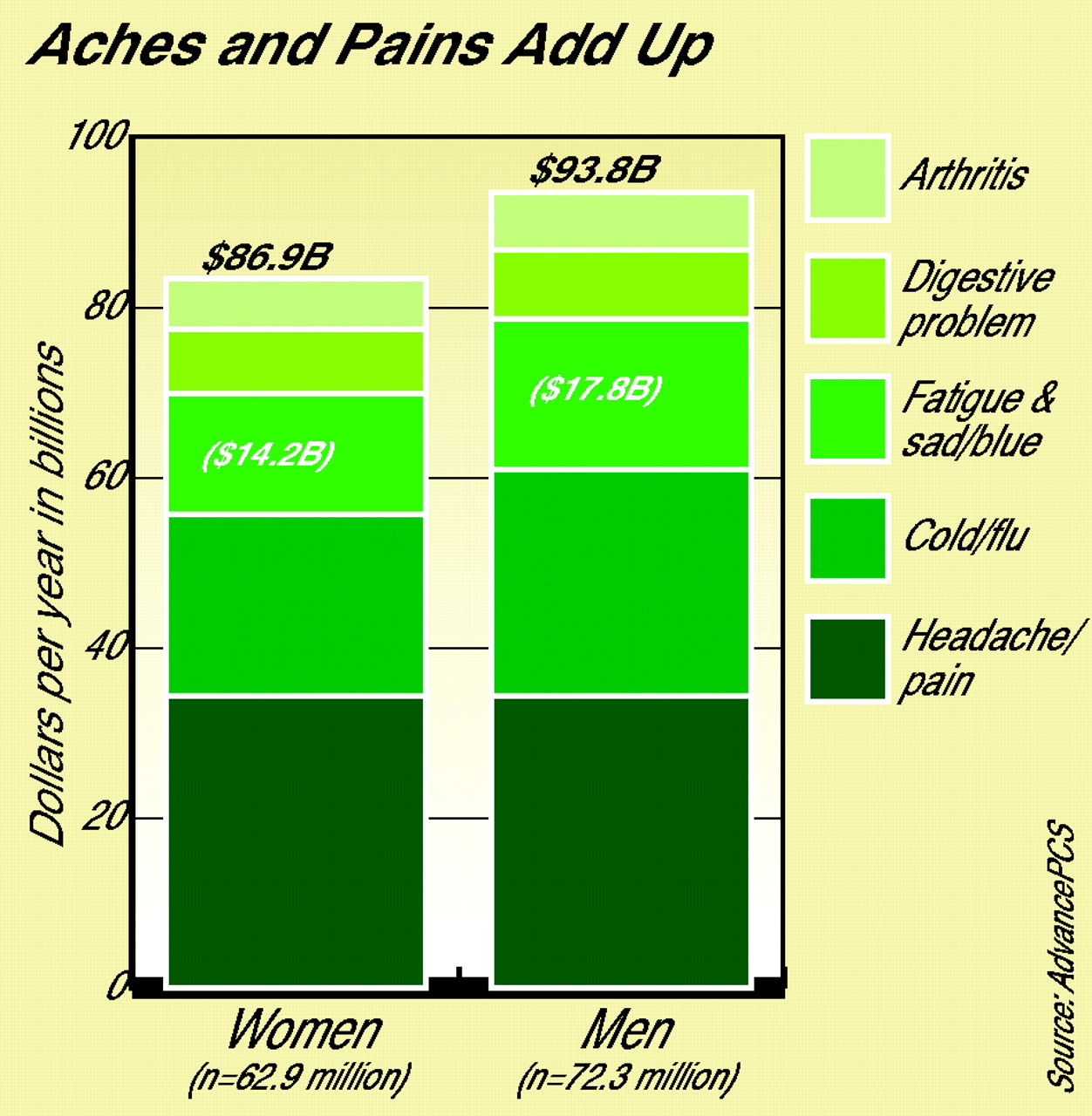
The annual cost of employees’ lost productive hours due to the conditions above is more than $180 billion.Using the interview results, Stewart developed data on hours of lost productive time (while an employee was at work or absent from work) among those with one of the ailments specified (see chart). Fatigue and sad/blue were outranked by cold/flu, headache/pain, digestive problems, and arthritis in terms of number of lost productive hours.
Stewart also tested his methods of calculating lost productive hours with the staff of the AdvancePCS call center. He had access to records showing productivity of employees in terms of calls answered and time on line and compared those records with self-reports.
Extrapolating from the database, Stewart estimated the total cost each year of the top five episodic health conditions in the U.S. workforce by gender. He combined the categories of fatigue and sad/blue because he is still developing a method of separating the costs.
The combined category of fatigue and sad/blue ranks third, with estimated annual costs of $17.8 billion for men and $14.2 billion for women. These costs include lost work time due to missed days and hours and reduced performance translated into lost hours.
Next Steps
Stewart envisions a five-stage implementation plan with employers. As the first stage, he will offer an employer a free estimate of the costs of work-related illnesses at that company or organization.
Stewart can tailor his database to fit the demographics of individual companies. “For example,” he said, “the average age of employees at AdvancePCS is about five years lower than the national average.” The age and sex distribution of a workforce, as well as other demographics, have implications for the prevalence of various ailments, as well as for the amount of time lost because of the illnesses of family members.
The second stage would be to conduct an employer-specific audit. Research, such as pilot studies and focus groups, is being conducted now to determine how best to communicate with employees and to understand how receptive they are to this work. Stewart would then work with the employer to prioritize illnesses in terms of their impact on costs and the likelihood that they can be successfully addressed with low-cost interventions.
He said, “For any one condition, 70 percent to 80 percent of the lost productive time is concentrated in 20 percent to 35 percent of the employees.”
The fourth stage would be to develop tools and services to address the conditions, and the fifth stage would be to evaluate the benefits of the interventions by conducting follow-up surveys where the costs of lost productive time are compared with estimates obtained in previous surveys.
AdvancePCS is conducting pilot studies with five companies on this implementation approach. Stewart said, “One of those companies (which cannot be named) has a workforce of about 23,000 individuals. We’re estimating that the company loses $60 million each year due to all illnesses. Five conditions account for 65 percent of the loss.” The figure includes lost productive time (due to missed days or missed hours and reduced performance at work) translated into lost hours.
Lloyd Sederer, M.D., director of APA’s Division of Clinical Services, said, “At the heart of our business initiative program is the belief that treatment for depression and other mental illnesses is important for the individual and is also good business. That is the message that we take consistently to employers.”
The program is an APA effort that started two years ago to educate the business community that providing good mental health services can positively impact their bottom line (Psychiatric News, July 20, 2001).
Sederer, along with Ron Z. Goetzel, Ronald J. Ozminkowski, and Tami L. Mark of the MEDSTAT Group, published an article, “The Business Case for Quality Mental Health Services: Why Employers Should Care About the Mental Health and Well-Being of their Employees” in the April issue of Journal of Occupational and Environmental Medicine. The MEDSTAT Group is a health information company.
The authors reported available information on employee depression and its impact on business, including the results of a recent analysis that found that depressed workers cost their employers 70 percent more in annual health costs when compared with nondepressed colleagues.
They also suggested promising research opportunities in light of their relevance, time feasibility, data availability, and affordability.
The Web site of AdvancePCS is www.advanceparadigm.com, and the Web site for the Washington Business Group on Health is www.wbgh.com. ▪
Researchers say that employers will take action when they are offered easy-to-use, verifiable methods of determining how employee illness affects profits.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Get Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.