Image (Irqi_soldiers_cover) is missing or otherwise invalid.Every armed conflict involving U.S. troops has produced psychiatric casualties. Operation Iraqi Freedom is no exception, although most of the casualties that occurred during the first three weeks of Operation Iraqi Freedom were not combat related.
“We know that no soldiers in direct combat were evacuated for psychiatric reasons from Iraq to Germany or the United States,” said Col. Theodore Nam, chief of inpatient psychiatry services at Walter Reed Army Medical Center in Washington, D.C. Nam is also president of the Society of Uniformed Services Psychiatrists, an APA district branch.
“The soldiers who were evacuated for psychiatric illnesses were en route to Iraq or in military support positions, such as cooks and supply personnel, and had pre-existing psychiatric problems,” said Nam.
Lt. Col. Cameron Ritchie: “We are preparing for the possibility that some [returning soldiers] may need psychiatric care in our military hospitals.”
An estimated one-quarter to one-third of U.S. troops in combat during World War I and II and the Korean War experienced acute stress reactions. The psychological reactions were referred to as “shell shock” in World War I and “battle fatigue” in World War II and the Korean War, said Lt. Col. E. Cameron Ritchie, a psychiatrist who heads the program for mental health policy and women’s issues in the Office of the Assistant Secretary for Health Affairs in the Department of Defense.
“We began seeing fewer acute stress reactions during the Vietnam War and in subsequent wars, but a significant number of troops developed posttraumatic stress disorder [PTSD] following combat in Vietnam,” said Ritchie, who is also the public affairs representative for the Society of Uniformed Services Psychiatrists.
The term PTSD was coined after the war in Vietnam to describe certain symptoms associated with combat, although undoubtedly soldiers in previous wars experienced PTSD. “We will be monitoring soldiers for PTSD when they return from Operation Iraqi Freedom. We are preparing for the possibility that some may need psychiatric care in our military hospitals,” said Ritchie.
Another reason for the decline in psychiatric casualties is that the role of the military has changed. Operations are smaller and often last months instead of years and include peacekeeping and humanitarian missions, said Nam.
Richard Carmona, M.D.: “When I came back from Vietnam, I didn’t experience PTSD, but it took a while for me to want to become part of society. . . .”
Helping the troops keep “mentally fit” has become an important part of military training, said U.S. Surgeon General Richard Carmona, M.D., in an interview with Psychiatric News. “Troops learn about the psychological aspects of warfare, including how to cope with stress before and during military operations, based on our knowledge accumulated from previous wars,” he said.
Combat stress control programs were announced by former President Bill Clinton at the 1999 landmark White House Conference on Mental Health.
Military training also includes how to handle being captured by enemy forces. “More intensive training called Survival, Evasion, Resistance, and Escape (SERE) is given to Special Forces troops and pilots because of their highly visible and vulnerable positions,” said Ritchie. She declined to describe SERE training due to security concerns.
The military may consider expanding its training to include soldiers not directly engaged in combat, such as soldiers in supply units. During Operation Iraqi Freedom, their vulnerability became apparent when several members of the 502nd infantry, a rear supply unit, were captured and held by Iraqi forces for 21 days until being rescued by Marines last month, according to a military source.
The military now routinely sends teams of psychiatrists and mental health professionals to help U.S. troops cope with stress associated with military operations overseas. These combat stress control (CSC) units typically are made up of a military psychiatrist, psychologist, social worker, and enlisted personnel with mental health training, said Ritchie. The size of a CSC unit depends on the number of troops involved in a mission and the type of mission.
The CSC unit is designed to function independently and brings its own military equipment and supplies including psychiatric medications, said Ritchie, who served in a CSC unit sent to Somalia in 1992.
She added that CSC units have been sent to Bosnia, Kosovo, Afghanistan, Somalia, and Haiti.
Nam coordinated the deployment of CSC units when he was in Germany in the 1990s following terrorist attacks on U.S. military and government facilities. Teams were sent after the U.S. Embassy was bombed in Kenya in 1998 and the Khobar Towers military housing complex in Saudi Arabia was bombed in 1996 killing 19 soldiers and injuring more than 200 personnel.
In Somalia, Ritchie worked with the military psychiatrist there, and they each covered a specific geographic area. “I conducted stress-management classes for the troops in which we discussed what they faced, their reactions, and effective ways of coping,” said Ritchie.
In Somalia, Ritchie also conducted debriefings for troops trying to cope with a fellow soldier’s death. “Soldiers described what happened and how they reacted to it. They were educated in normal reactions to abnormal situations and what to do if their psychological difficulties persisted,” said Ritchie.
She saw several cases of psychosis including two severe ones while stationed in Somalia. One soldier had hallucinations due to cerebral malaria, and a second soldier had psychotic delusions. The first case resolved quickly with medical treatment, and the second was stabilized with psychotropic medications. The second soldier was evacuated several days later for further evaluation and treatment, she noted.
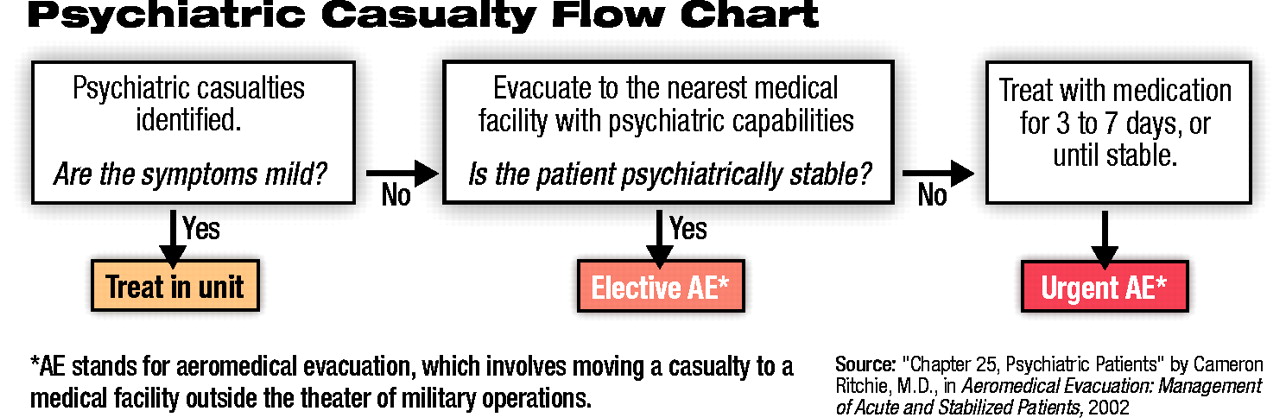
“In deciding whether to evacuate [a person with a psychiatric problem], we look at the severity of the psychiatric symptoms and other factors such as whether the person can be stabilized and treated in a temporary mental health unit,” said Ritchie. (see chart).
Soldiers who have significant suicidal ideation or are psychotic are usually evacuated out of the area of military operations.
Since World War II, to avoid unnecessary evacuations, the military has emphasized treating soldiers in close proximity to their units, immediately, and with the expectation of returning them to their units. This treatment relies on simple methods including provision of hot meals, rest, and supportive therapy, said Ritchie.
“Using these principles, we have returned 60 to 80 percent of soldiers treated in the field to active duty,” said Ritchie. The principles were implemented after World War I because so many shell-shocked soldiers were evacuated to the United States for treatment that it impeded the war effort, Ritchie explained.
“We also discovered during the Korean War that evacuating soldiers to comfortable, clean hospitals in Japan made it harder to return them to the war,” said Ritchie.
When units return to the United States from Operation Iraqi Freedom, they will be educated about common signs of stress and PTSD.
“We tell them it’s normal to experience some psychological symptoms of trauma, but if the symptoms continue for more than a month or so, we advise them to seek professional help,” said Ritchie.
Specially trained SERE psychologists cared for Pfc. Jessica Lynch and the seven other American prisoners of war after they were freed and evacuated from Iraq last month, according to an April 22 American Forces Information Service news article.
The soldiers underwent an established process of debriefings, decompression time, and reintegration into society, Ritchie added.
The debriefings are intended to solicit time-sensitive information that may be useful to the military, according to the article.
The former captives are given several days to unwind, interact with each other, and come to terms with their experiences. Their families may also be counseled as to what to expect from the soldiers before they are reunited, said Ritchie.
“The decompression time is essential to avoid sensory overload. In captivity, the soldiers may have experienced isolation, sensory deprivation, beatings, and other harsh treatment,” said Ritchie.
As members of the armed forces return home, Carmona said it is important that psychiatrists and mental health professionals reach out to them to help them reintegrate into society.
“When I came back from Vietnam, I didn’t experience PTSD, but it took a while for me to want to become part of society rather than just to socialize with my war buddies,” said Carmona.
The April 22 American Forces news article is posted on the Web at www.dod.gov/news/Apr2003/n04222003_200304222.html. ▪
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.